Primary squamous cell carcinoma PSCC of the breast is extremely rare [1]. The histogenesis of this tumour is debatable but compelling evidences have been traced to the skin epidermis, the nipple or epithelium of a skin adnexae and deep-seated dermoid cyst or squamous metaplasia of the ductal epithelial cells following chronic inflammation [2].
Pure squamous cell carcinoma of the breast is very rare. Strict histological criteria must be followed before the diagnosis can be made. Squamous cell carcinoma of the skin and/or its appendages in which the squamous cell carcinoma is a portion should be excluded. Areas of metaplastic change in an otherwise ductal carcinoma should not be diagnosed as pure squamous cell carcinoma. Squamous cell carcinoma from other parts of the body with metastasis to the breast should also be excluded.
We report a case of primary squamous cell carcinoma of the breast in a 60-year-old woman.
It is a breast carcinoma entirely composed of squamous cells that may be keratinized, non-keratinized or spindled. The pure squamous cell carcinoma usually presents with central cystic cavity, which we also found in our case. The squamous cells seen in this case was supported by immunohistochemical evidence.
Although a rare breast cancer subtype, pure squamous cell carcinoma of the breast is of considerable interest due to its pathological heterogeneity and differences in clinical behavior.
Squamous cell carcinoma is a well-known malignancy of the skin and other organs that are lined with or covered by squamous epithelial cells. Squamous cell carcinoma of the breast is very rare. It is important to differentiate this entity from malignancies of the overlying skin of the breast or metastasis of a squamous cell carcinoma somewhere else in the body. In the literature only some small series are reported. Reported incidences of primary squamous cell carcinoma of the breast vary between 0.04% to less than 0.1% of all breast carcinomas [1].
Clinical and radiographic characteristics are not specific, and the tumours are usually hormone receptor negative. In general, they are known to be very aggressive and treatment-refractory tumours with poor prognosis. We report a case of a rare breast malignancy and we review the literature.
A 60-year-old woman presented with left breast lump of 3-month duration. The lump was painless and progressively increasing in size. There was no associated nipple discharge and no ulceration of the overlying skin. There was no swelling in the contra lateral breast and the axilla. No other lesions were found elsewhere in the body. The patient gave no family history of breast cancer and there was no history suggestive distant metastasis.
Physical examination revealed a non-tender mass measuring 4 × 4 cm in the upper medial quadrant of the left breast. It is firm and has irregular edge. There were matted left axillary lymph nodes. Fine needle aspiration cytology of the mass was done and was reported as malignant (C5). Chest radiograph and ultrasound scan of the abdomen showed no evidence of chest or abdominal tumour. Other haematologic investigations were within normal limits.
The patient had 3 courses of neoadjuvant chemotherapy with Adriamycin and Cyclophosphamide and subsequently underwent simple mastectomy and axillary clearance. The mastectomy specimen weighed 250 g and measured 16 × 10 × 3 cm. The overlying skin measured 15 × 9 cm. Serial cut sections of the specimen show a tumour mass measuring 4 × 3.5 × 2 cm. The tumour is located at the upper medial quadrant and located 4 cm below the upper resection margin.
Microscopically, histologic sections of the tumour show infiltration by malignant squamous epithelial cells that are disposed in cell nests. The cells are large and pleomorphic with glassy appearance. They have vesicular nuclei and scanty cytoplasm. They show individual cell keratinization and intercellular bridges with areas of intratumoural infiltration by mononuclear inflammatory cells, comprising lymphocytes and plasma cells. Keratin pearls and areas of dystrophic calcification are seen. No ductal or glandular element is seen. The overlying skin is unremarkable (Figure 1, Figure 2 and Figure 3). The overall features are in keeping with pure squamous cell carcinoma of the breast (large cell keratinizing variant). The resection margins and the axillary lymph nodes are free of the malignant cells. Immunohistochemical staining of the tumour cells are negative for ER, PR and HER2/neu but are strongly positive for CK5/6 (Figure 4, Figure 5, Figure 6 and Figure 7).
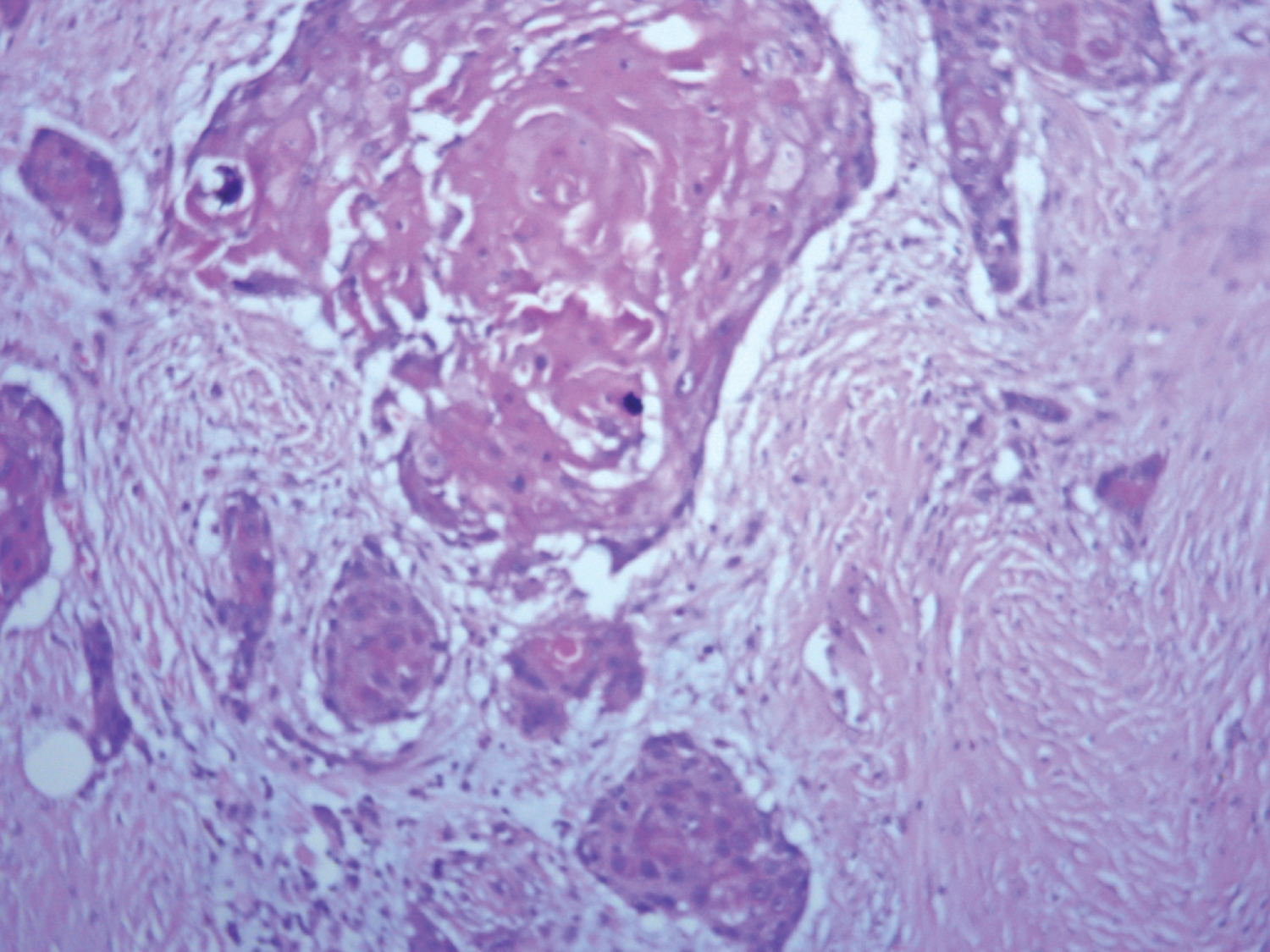 Figure 1: Tumour cells stained with Haematoxylin and Eosin (H&E).
View Figure 1
Figure 1: Tumour cells stained with Haematoxylin and Eosin (H&E).
View Figure 1
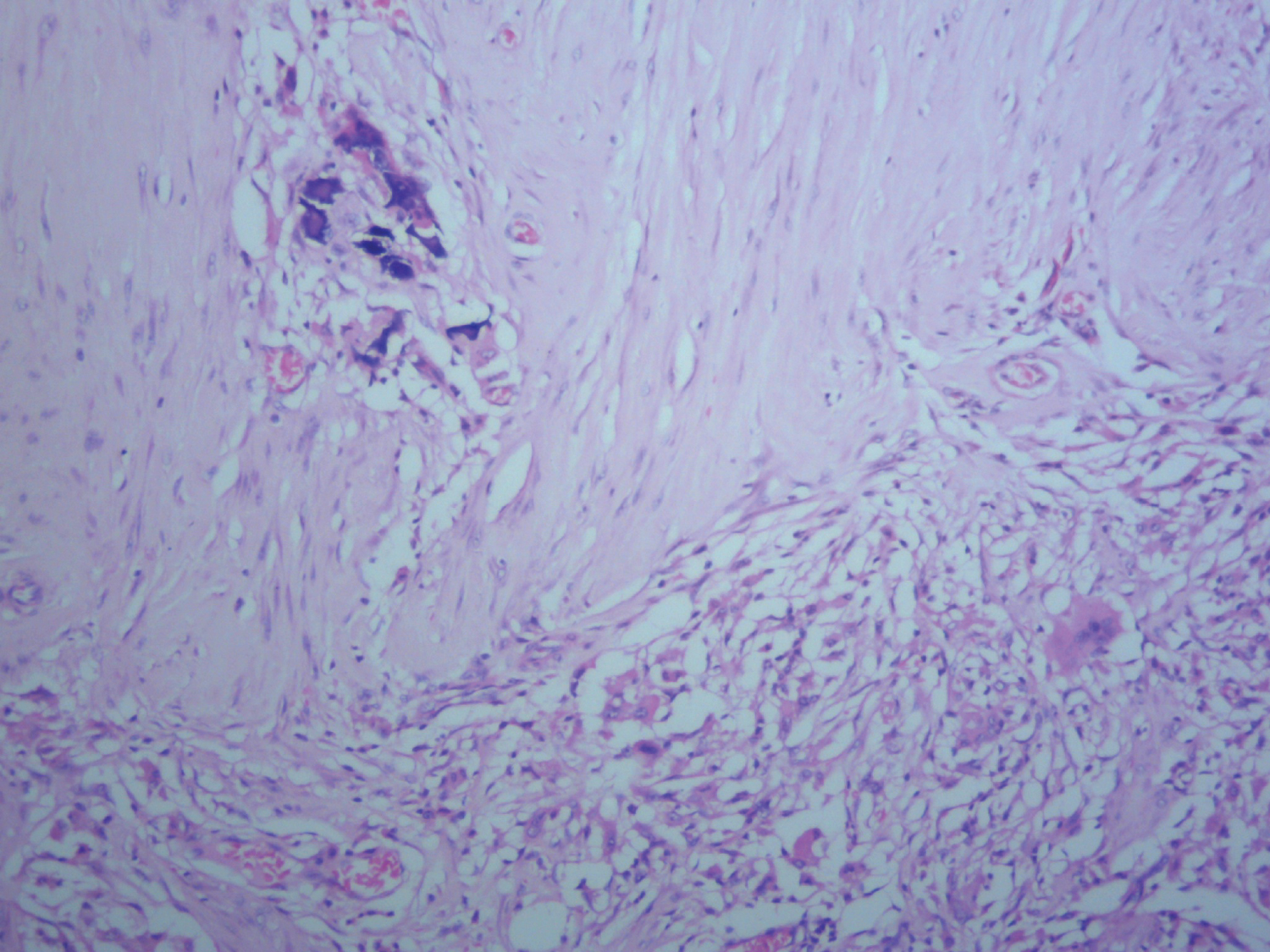 Figure 2: Focus showing area of dystrophic calcification with H&E stain.
View Figure 2
Figure 2: Focus showing area of dystrophic calcification with H&E stain.
View Figure 2
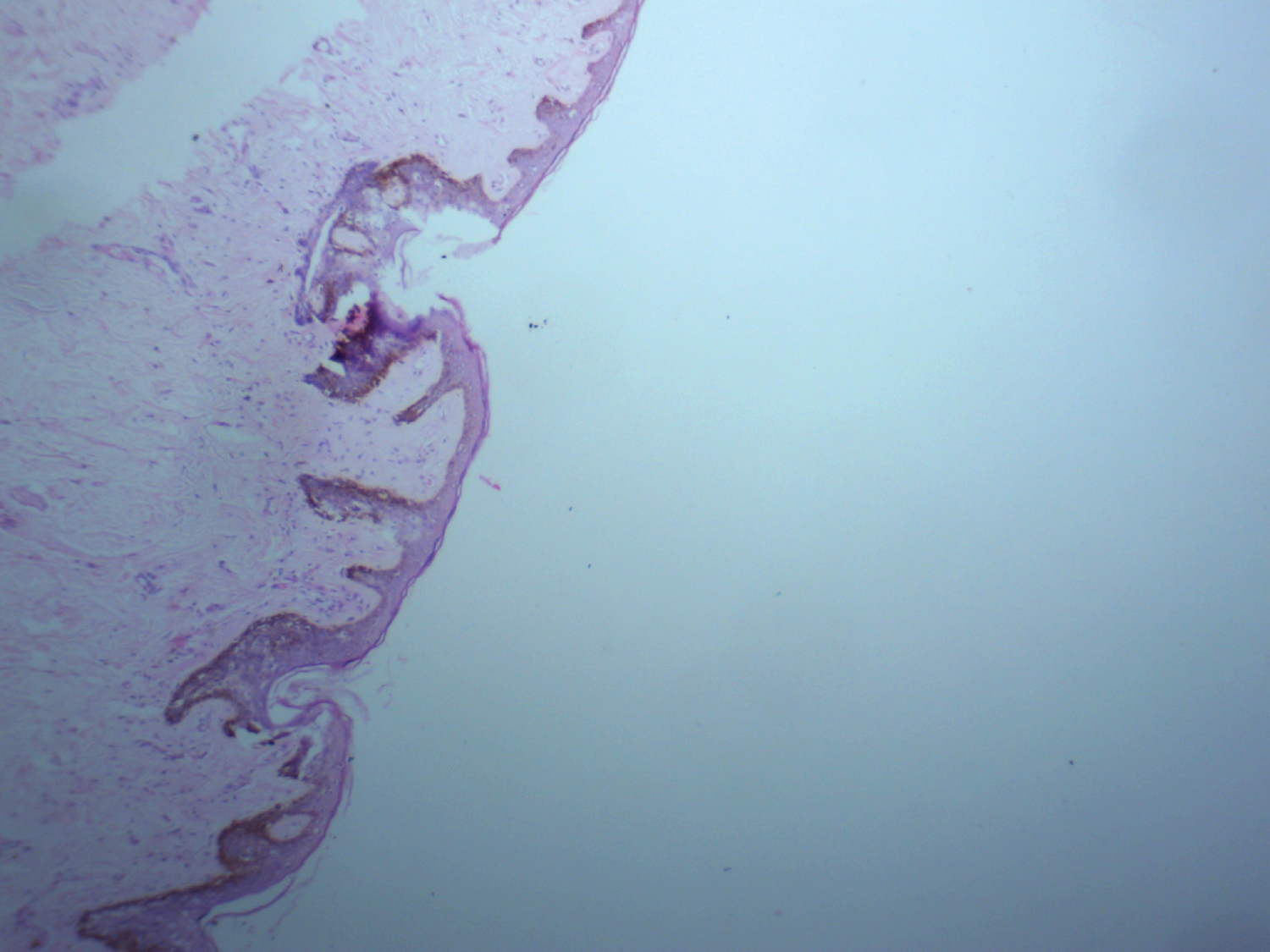 Figure 3: Histological section showing intact skin on H&E stain.
View Figure 3
Figure 3: Histological section showing intact skin on H&E stain.
View Figure 3
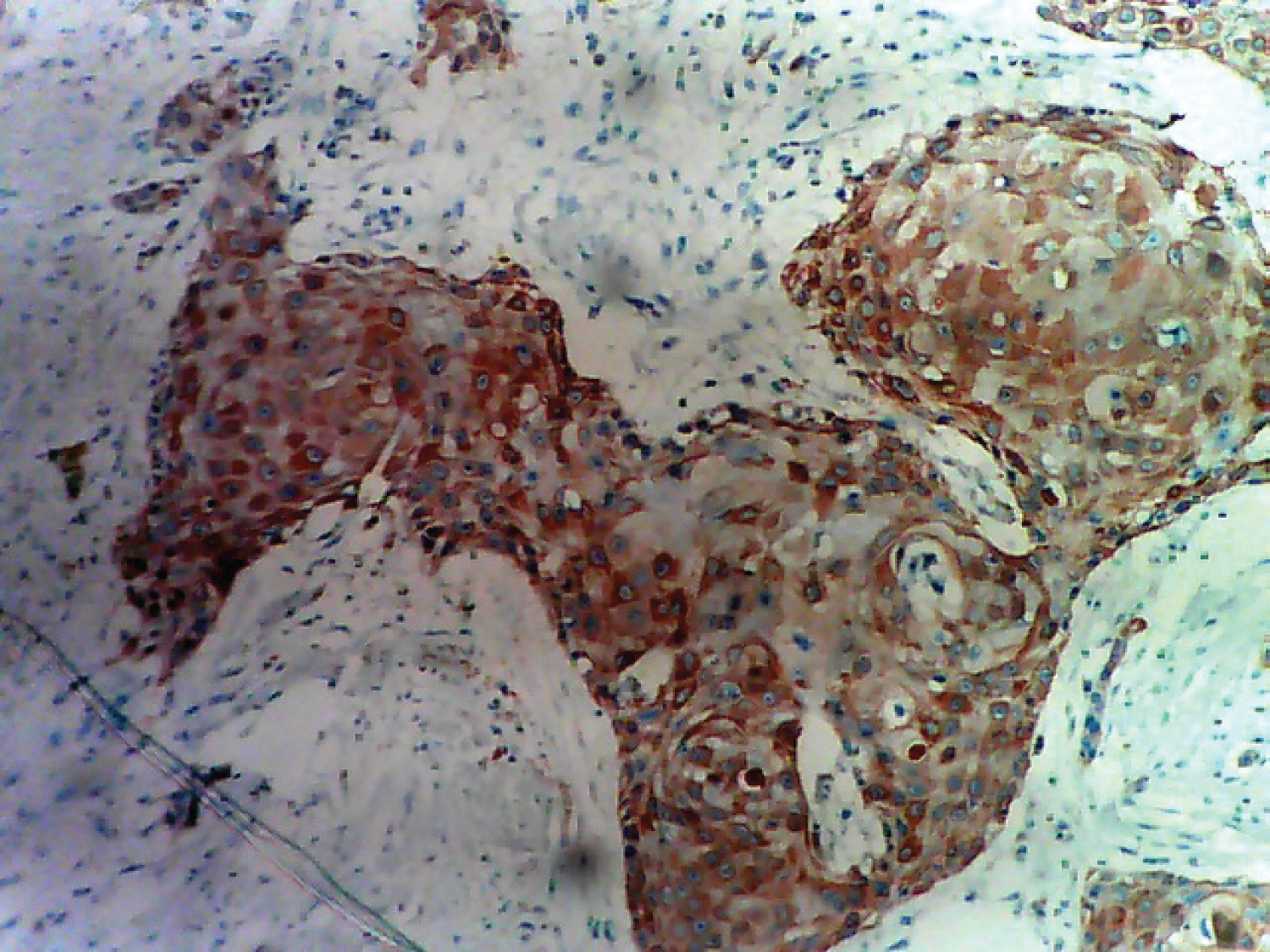 Figure 4: Tumour cells showing cytokeratin (CK) 5 and 6 positivity.
View Figure 4
Figure 4: Tumour cells showing cytokeratin (CK) 5 and 6 positivity.
View Figure 4
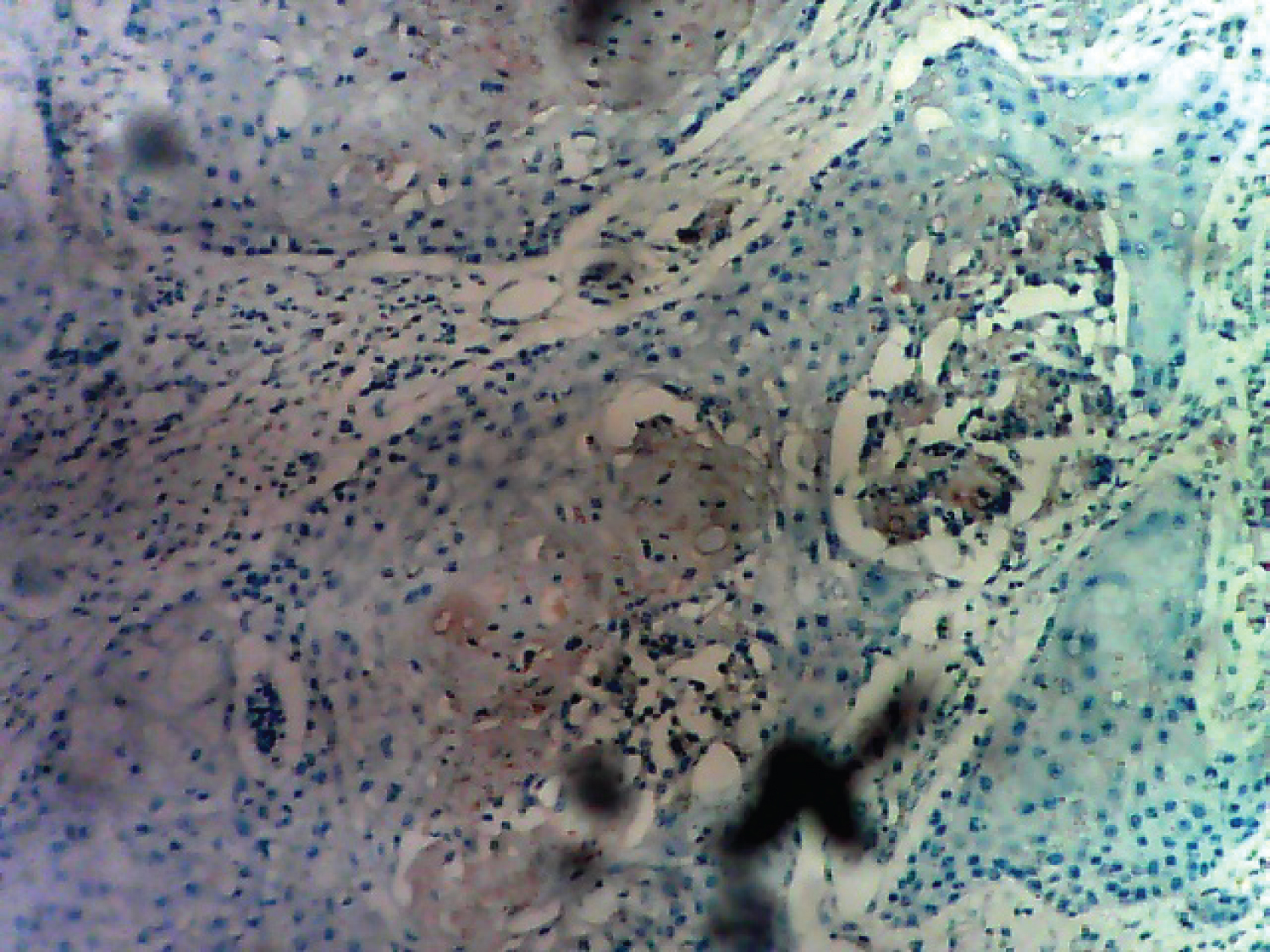 Figure 5: Tumour cells showing estrogen receptor ER negativity.
View Figure 5
Figure 5: Tumour cells showing estrogen receptor ER negativity.
View Figure 5
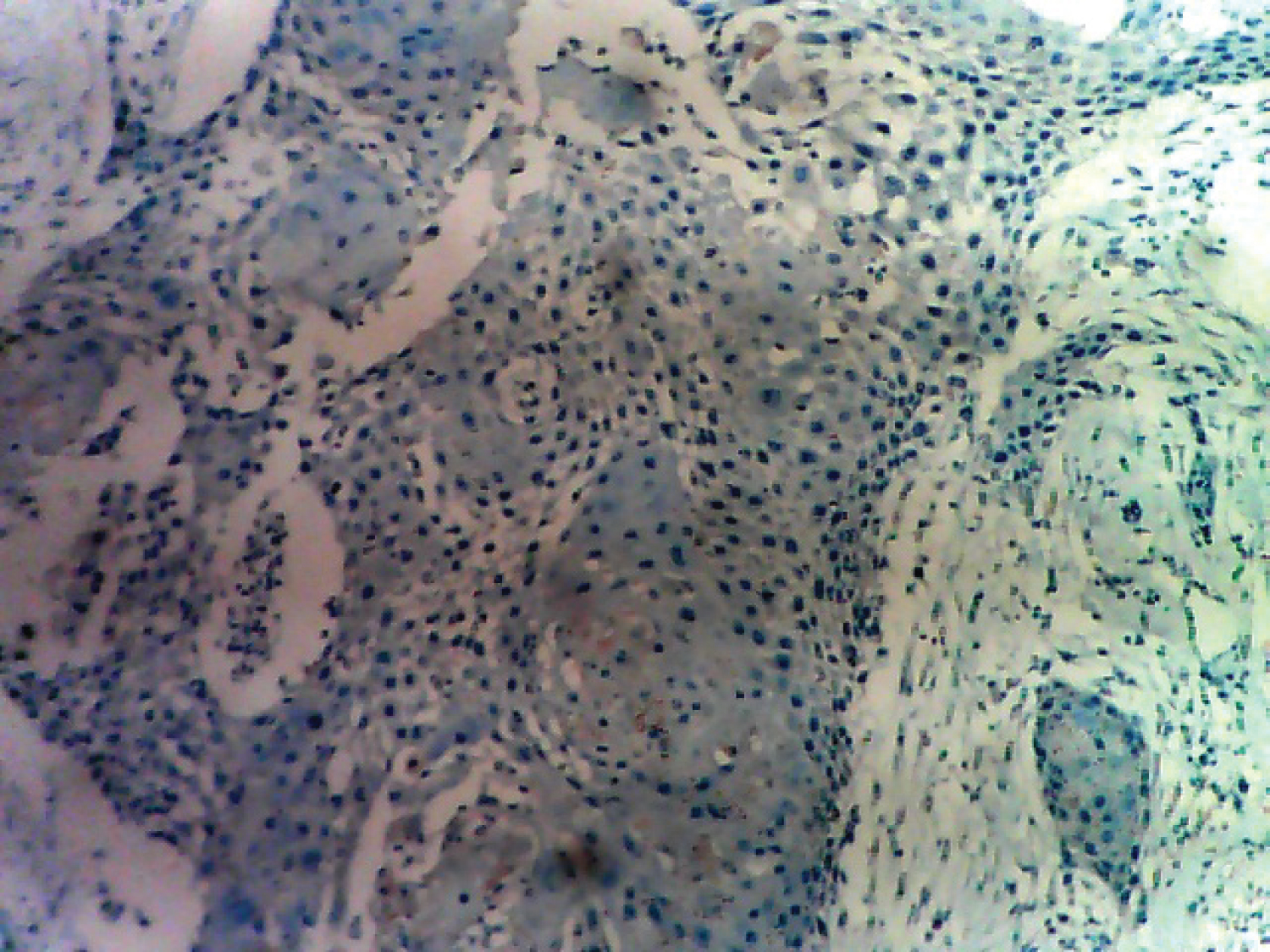 Figure 6: Tumour cells showing progesterone receptor PR negativity.
View Figure 6
Figure 6: Tumour cells showing progesterone receptor PR negativity.
View Figure 6
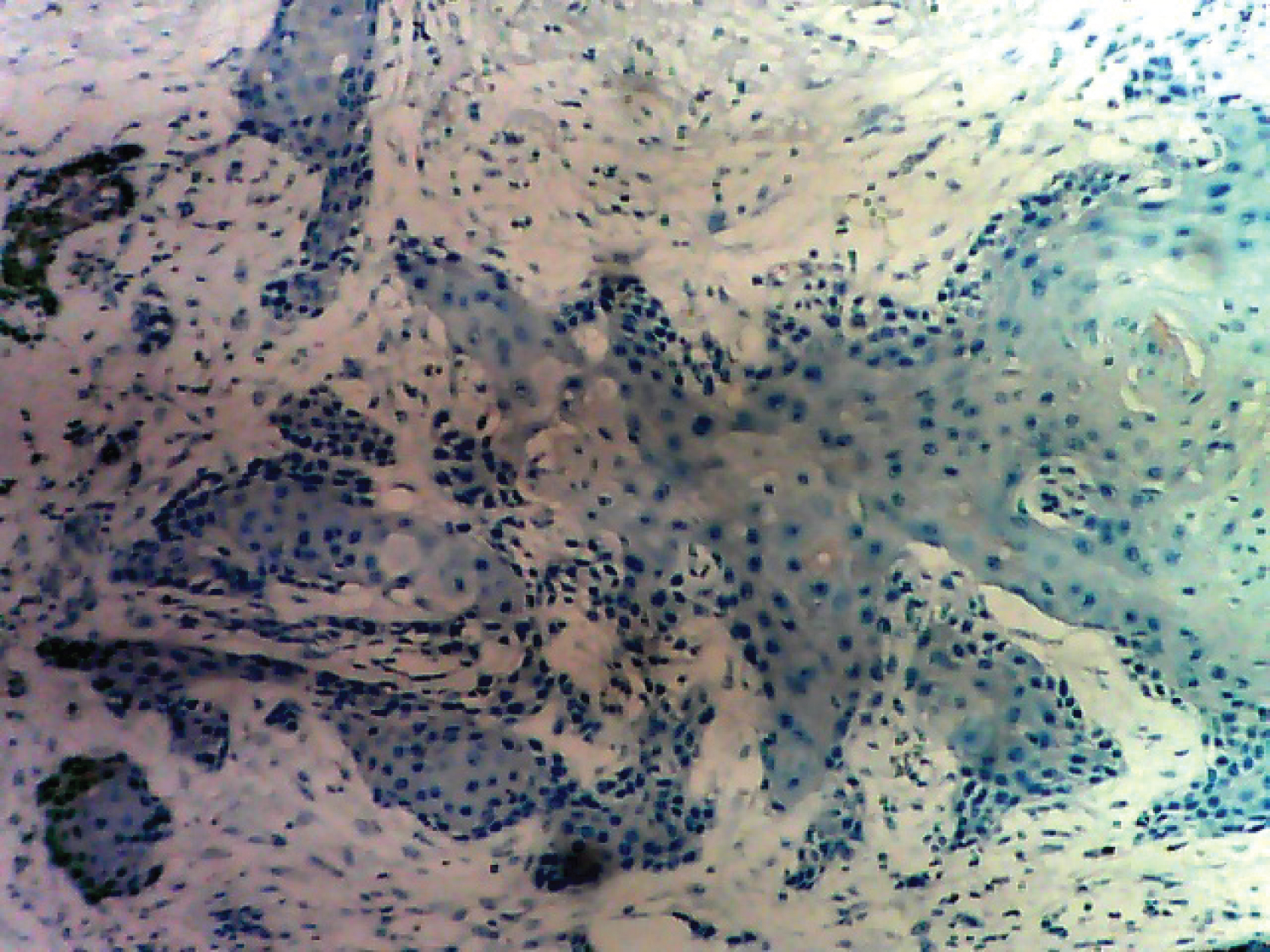 Figure 7: Tumour cells negative for HER2/neu.
View Figure 7
Figure 7: Tumour cells negative for HER2/neu.
View Figure 7
The postoperative course was uneventful. Patient had 3 courses of adjuvant chemotherapy with Adriamycin and Cyclophosphamide. She also had radiotherapy to the chest wall and was on follow-up with no evidence of loco regional recurrence or metastatic deposits 12 months after surgery.
Squamous cell carcinoma SCC of the breast is rare. Incidence for SCC breast is 0.04-0.1% of all malignancies of breast. A pure form of primary SCC breast is also described and its incidence is still less. It most often affects post-menopausal women; however cases in younger patients have been recorded [3,4].
The histogenesis of this rare malignancy is unclear. Theories include malignant growth of intrinsic epidermal elements, epidermal or dermoid cysts and metaplasia from breast parenchyma or from chronic abscess. Not surprisingly, these tumours have varying degrees of homogeneity [5]. A tumour is considered pure squamous cell carcinoma if it meets Macia, et al. criteria [6].
a) No other neoplastic components such as ductal or mesenchymal elements are present in the tumour.
b) The tumour is independent of adjacent cutaneous structures.
c) No other primary squamous epithelial tumour is present in the patient (oral cavity bronchus, oesophagus, renal pelvis, bladder, ovary, and cervix).
Pure squamous cell carcinoma of the breast most often affects post-menopausal women. However cases in younger patients have been recorded [4]. It has been diagnosed in adult women of ages ranging from 29 years to 90 years, with a median of 52 years of age. The youngest patient reported in the literature so far (Raje, et al.) was 27-years-old [4] and to date over 100 cases have been reported [7,8].
In contrast to most breast cancers, PSCC are unusually rapidly growing. The clinical presentation is variable. There are several published cases in which the patients presented with breast abscesses, intracystic lesions or solid masses. The tumours tend to be relatively large (range 2-5 cm, median 4 cm) [1,9]. Our case is a 60-year-old with 3-month duration of the disease which is consistent with many cases reported in the literature [1,9].
Most of these tumours present either as cystic masses or have a cystic component with central necrosis [9,10]. Our case presented with a solid mass, although central areas of necrosis are seen on histology. PSCC of the breast was found to be associated with lower rate of lymph node metastasis at presentation (22% vs. 40-60% for infiltrating ductal carcinoma) and a significant rate of distant metastasis without lymph node involvement. This is in contrast to squamous cell carcinomas appearing at other parts of body which metastasis frequently to regional lymph nodes [7,8].
Most cases of PSCC of the breast do not show hormonal (oestrogen, progesterone and HER-2/neu) expression. The oestrogen ER and progesterone PR receptor expression are negative in more than 90% of the cases [5,7,8,10,11]. This is consistent with our finding in this case as ER, PR and HER2/neu are all negative while CK5/6 is strongly positive. In the literature, only 4 cases of HER-2/neu over-expression in PSCC of the breast have been reported in the literature. One case was reported by Karamouzis, et al. [12] while in a series reported by Shui, et al. in Shanghai, China; 3 cases of HER-2/neu over expression was reported out of 30 cases of PSCC of the breast [13]. Most cases of PSCC of the breast are characterized by lack of micro calcification on mammogram. In the literature, there are 2 reported cases of SCCB that show micro calcifications on mammogram [14,15]. The case we report did not do mammography, although areas of calcification are seen in histological sections.
The outcome and prognosis of PSCC of the breast are subjects of debate but these appear to be dependent upon several factors, most importantly tumour size and tumour stage. The SEER database from 1988 to 2001 which included 137 cases of SCCB showed a 5-year survival rate of 64% [11]. The initial management of SCCB is modified radical mastectomy with adjuvant radiotherapy and/or chemotherapy. The addition of hormonal therapy depends on the hormonal status of the tumour. Since squamous cell carcinomas are often radiosensitive, Hennessy, et al. proposed early adjuvant radiotherapy despite being unable to demonstrate a difference (presumably because of small numbers) in the loco-regional relapse-free rate of 45% among those receiving vs. 33% among those not receiving radiotherapy [11].
In this case, the patient had 3 courses neoadjuvant (preoperative) chemotherapy with Adriamycin and Cyclophosphamide. Postoperatively, the patient had another 3 courses of adjuvant chemotherapy with Adriamycin and Cyclophosphamide in addition to radiotherapy of the chest wall. The postoperative period course was uneventful and was on follow-up with no evidence of loco regional recurrence or metastatic deposits. Definitive management of patients with pure squamous cell carcinoma is still not clear. Dejager, et al. [16] and many other authors [3,16] postulated that cisplatinum-based chemotherapy should be considered in the treatment regimen of this disease. In this type of cancer, Weigel, et al. [17] recommended the same multi-modality management as adenocarcinoma at the same stage. It is noteworthy to report that the patient reported in this case did well even with an unusual chemotherapeutic combination of Adriamycin and Cyclophosphamide.
Pure squamous cell carcinoma of the breast is a rare but generally aggressive disease. Current surgical management is similar to that for the more common adenocarcinoma. However, because effective adjuvant or neoadjuvant therapy is not readily available, future research should focus on the molecular biology, (e.g., epidermal growth factor receptor), to develop tumour-specific therapy. Treatment should be stratified in order to give a tumour/patient-specific treatment. The patient we report in our case did well even with an unusual chemotherapeutic combination of Adriamycin and Cyclophosphamide.
The case was attended to by the surgical team of Dr. Abiyere OH. Dr. Omotayo JA and Dr Soremekun AI handled the surgical mastectomy specimen; Dr. Omotayo JA and Dr Erinomo OO made the histopathology diagnosis of the case. Dr. Omotayo JA and Dr. Abiyere OH prepared the manuscript.
Subsequently all the authors formulated the manuscript. The manuscript has been read and approved by all the authors, the requirements for authorship have been met, and each author believes that the manuscript represents an honest work.
The authors express their indebtedness to Mr. Jonathan Madukwe who helped to perform the immunohistochemical procedure.
The authors declare no conflict of interest.
The patient paid for her surgical care including the cost of histopathology (except the cost of immunohistochemistry). This case report was entirely funded by the authors including the cost of immunohistochemistry, (as our centre is yet to commence routine immunohistochemistry services).
Written informed consent was obtained from the patient for publication of this case report and accompanying images. Copy of that consent can be produced whenever required.