Objetive: The purpose of this investigation was to find the anxiety levels, physical data and subjetive perception and explore the relationship between demographic, clinical and cancer patients' variables, pre and post-procedure during a PET/CT scan.
Patients and methods: The sample was distributed in five groups: 54 in one of the four experimental groups and 54 inthe control group (oral information, witten information, music, meditation induction). The study was conducted using an ad hoc questionnaire and the standardized State-Trait Anxiety Inventory (STAI).
Results: We found a significant effect on the level of post-intervention subjective anxiety, controlling for the effect of pre-intervention anxiety levels. With respect to the effectiveness of music and meditation induction on the post-intervention STAI state anxiety score we found significant differences between the intervention group and controls.
Conclusion: Our work shows that music and meditation induction can be used as a relaxation and anxiolytic mechanism as an integral multimodal part in patients during the uptake phase before PET-CT studies.
Nuclear Medicine is the medical specialty that uses radioactive isotopes and nuclear radiation for the study of biological phenomena caused by the use of radioactive isotopes for medical use and the application in diagnosis and treatment.
This diagnostic imaging technology uses radiopharmaceuticals and the most widely used is 2-[18F]-fluor-2-deoxy-D-glucose (18F-FDG). Among the different applications of 18F-FDG PET-TAC, it stands out its application in Oncology being a fundamental tool for the diagnosis, staging, treatment control and detection of recurrence in these patients.
Anxiety is an emotion experienced by all people and accompanying the human being throughout their existence. It is a complex reaction of the individual to situations and stimuli potentially dangerous or subjectively perceived as fraught with danger. It can be considered as a trait, tendency over a long period of time to confront or interact with the environment with an excessive degree of anxiety, or as a state presence of anxious symptoms at a specific and definite moment [1,2].
A high percentage of patients who go to the Nuclear Medicine service for an exploration or administration of a treatment do not know why they have been referred, what will be administered, the test to be performed or whether they will have to be isolated by the radiopharmaceutical. Attending an Image Diagnosis Service such as the Nuclear Medical Service to undergo an 18F-FDG PET/CT, therefore, leads to high levels of anxiety, distress and unease in cancer patients [1,3-7]. In some cases, may even lead to false positives, 18F-FDG uptake in muscles and brown fat, with a decrease in image quality and lower diagnostic performance [8-11].
Therefore, it is very important to know the emotional impact in the patients who come to the Nuclear Medicine Service to perform a PET-CT study. Several interventions have been developed to improve the patients' experience in diagnostic tests, and to reduce the feelings of anxiety before and after the tests. There are diverse proposals whose intention is to reduce adverse emotional responses in patients. These include providing the patient with more information about the procedure itself [4,9,12], giving the patient leaflets, comics, etc., to read [13], providing music and relaxing images or sounds from nature [5,11,14], training the patients to relax with progressive muscle relaxation or abdominal breathing [15,16], sedation through the administration of anxiolytic drugs such as diazepam [17,18], improving the conditions in which they rest in waiting room and manipulation of environmental factors, such as pleasant stay, temperature [19,20] applying meditation or full attention, or mindfulness programs [21-23] or hypnosis techniques, etc [24-26].
These interventions or techniques have had positive effects in improving anxiety levels and obtaining benefits and satisfaction with the procedure. Therefore, in order to reduce the negative repercussions of a patient with high anxiety, it seems advisable to develop different interventions from the Nuclear Medicine Services in order to reduce, mitigate or prevent such fear, pain, uncertainty, discomfort and anxiety [27].
The presence of anxiety in patients undergoing a PET-CT study is a challenge on the part of the health personnel to respond and that can generate difficulties in the normal operation of the service and of the test, as a greater time in need of being attended, activation of brown fat, presence of muscular tension, appearance of an anxiety attack and that the test can not be carried out. All this, as a whole, would cause the presence of a worse quality of care where the patient felt that it is not the center of health care, which is not important in the context of care and is not taken into account [1,4].
The aim of the present work is an evaluation of the anxiety (subjective and objective) and comparative study of the effectiveness of different interventions for the reduction of anxiety in a sample of cancer patients that go to the Nuclear Medicine Service for the accomplishment of an 18F-FDG-PET-TAC.
Therefore, it is postulated that the application of the different modalities of intervention: Oral information, written information, listening to music and hypnotic induction will produce a reduction in the degree of anxiety measured, both subjectively and objectively, measured physical parameters in a sample of cancer population that goes to a Nuclear Medicine Service to perform a PET-CT study.
The present study is an analytical epidemiological study with pre/post-intervention measures with four intervention groups and a control group, recruiting a total of 270 patients undergoing a PET/CT study. Randomization was performed using the function "sample" in a random sofware R32 [28,29]. The sample was distributed in five groups (four experimental groups and one control group), with 54 subjects in each group.
Patients are eligible if they meet the following criteria: 1) Over 18 years of age, 2) Oncological patients (i.e., those who had diagnosis of previous cancer of at least 2 months), and 3) Able to hear audio recordings. Patients are excluded if they are 1) Considered by the clinician to be too unwell to participate or 2) Unable to understand and complete the self-administered questionnaires.
Mean age was 59.68 years (SD = 13.91) with 121 men (44.8%) and 149 women (55.2%). The majority nationality was Spanish (93.3%) and in the civil status the married ones predominated (68.1%). Academic training represented the highest percentage of basic and high school studies (64%) and only 31.9% of the subjects in the sample were working.
Most of the subjects in the sample (94.4%) had no psychopathological antecedents and 93.3% of the subjects in the sample had no family history of anxiety or depression. Only 8.1% had knowledge of relaxation techniques.
This study was approved by the Clinical Research Ethics Committee (La Paz University Hospital, Madrid, Spain) (HULP: 4286), and has followed the basic principles of "good clinical practice". Set out in the Harmonized Tripartite Guideline of the International Conference on Harmonization (ICH).
After acceptance and signing of informed consent by the patients to participate, they were administered the "ad hoc" qestionnaire, STAI and different measures of BP and HR baseline (pre-test application).
After that, they were immediately assigned to one of the five groups: 54 in one of the four experimental groups and 54 in the control group. Immediately following 18FFDG was injected in the waiting room and during this time each participant was in an intervention group or in a control group where they were rested. Once the waiting time was over, the patients in all groups were taken for the PET/CT scan.
Subsequently, after performing the diagnostic test, they were re-applied the same "ad hoc" and STAI evaluation questionnaire (postest application), as well as some of the most relevant questions that have been previously made and taking physical symptom measures.
In the development of the procedure, the usual procedure was defined as that performed according to the protocol of the Normalized Working Procedure of the patients in the PET-CT Unit of the Nuclear Medicine Service of the La Paz University Hospital.
In relation to the development of the interventions, the proposed interventions consisted of: 1) Oral information where the PET-CT test was reported in a detailed and accurate manner, adapting the language making the verbal language (what we say), paralanguage (tone that we use) and non-verbal language coherent and ensuring that the patient understood the process; 2) Written information providing an informative leaflet in the form of a triptych made ex profeso in which it is explained in a simple way in which PET-process to which the patient is going to submit, allowing the opportunity for the patient to clarify the doubts that have arisen once read all the information in case you need it; 3) Listening to music that consisted of listening to music during the 50-60 minutes of waiting time since the injection of the radiopharmaceutical 18F-FDG was carried out until the time when the study was performed using an MP3 device choosing the music of Dan Gibson selected in this study based on recommendations and guides in which they recommend a series of characteristics (Reporting Guidelines for Music-based Interventions). The music selected was a music with sounds of nature; 4) Hypnotic induction which consisted of the fact that during the 50-60 minutes of waiting time from the time the injection of the 18F-FDG radiopharmaceutical was carried out until the time of the test, the patient listened to a hypnotic induction recording in support MP3 made ad hoc by Dr. Roberto Aguado, Dr. in Psychology and Psychologist Specialist in Clinical Psychology and president of the European Institute of Limited Time Psychotherapy. It contained background music and sounds of nature over which an off-voice made descriptions in order to guide the patient and induce a state of deep relaxation with the fomentation of selfobservation and the acceptance.
The study was conducted using an "ad hoc" questionnaire and the standardized State-Trait Anxiety Inventory (STAI) [2]. It is a questionnaire with 40 items aimed at assessing the level of anxiety in healthy adults. It includes scales to measure different but related facets of anxiety, such as trait anxiety (TA or STAI-T) and state anxiety (SA or STAI-S). In general, trait anxiety reflects a relatively stable emotional state and measures a person's general tendency to perceive day-to-day situations as threatening, as well as the person's baseline feelings. In contrast, state anxiety refers to subjective and transitory feelings of tension, apprehension, and fear, which can vary over time and fluctuate in intensity, how a person feels in a concrete stressful situation and increases in response to various situations and occurrences. Trait anxiety and state anxiety are theoretically independent constructs [2]. Its two subscales include items that refer to behavioral, cognitive, emotional and physiological aspects.
It is validated in Spanish language [2]. The questionnaires query subjects regarding both types of anxieties by measuring the intensity with which they feel emotions and sensations of anxiety at aparticular moment, choosing among four possible responses: Nothing, something, a fair amount, and very much (0, 1, 2, and 3 points, respectively). Both questionnaires include 20 questions, with possible scores ranging from 0 to 60 points per question, the highest score indicating the highest level of anxiety. These points give a numerical value for TA and another for SA, and their sum is the STAI Sum. The STAI-Total is the absolute value of the difference between the two values and offers information about whether an event causes anxiety. Are considered anxiety-inducing in those who obtain a value greater than 10 points (STAI-Total > 10) [30]. The STAI are adapted and validated in the Spanish population with a Cronbach's alpha of 0.93 for STAI-T and 0.92 for STAI-S [31].
To assess the variables most directly related to patients' personal and medical data, an adhoc questionnaire was designed including the most representative and characteristic variables relevant to the study. This adhoc questionnaire contained questions on the following categories: (1) Sociodemographic data (age, gender, date of birth, educational background, job, marital status, number of children); 2) Family history of psychopathology (personal historyof depression or anxiety, family history of depression oranxiety, knowledge of relaxation techniques or similar); 3) Data on current diagnosis (primary location of tumor, treatment received, reason for PET/CT); 4) Pre-intervention physical data (blood pressure [BP], heart rate [HR], feeling of dyspnea, digestive problems [nausea, vomiting], muscle tensión and stiffness, dizziness and instability; level of subjective anxiety [0-10] at current time); and 5) Post-intervention physical data (blood pressure [BP], heart rate [HR], feeling of dyspnea, digestive problems [nausea, vomiting], muscle tension and stiffness, dizziness and instability; level of subjective anxiety [0-10] at current time).
Once the data were collected, we conducted statistical análisis using SSPS 22. For the variable distribution analysis, the Shapiro-Wilk statistic was calculated using a Lilliefors significance level to study the normal variable distribution. We performed a univariate analysis to compare frequency distribution. We also conducted descriptive analyses (mainly means and standard deviations) and covariance analyses, which were used to measure the effectiveness of the interventions in modifying anxiety and different biomedical parameters. For the analysis, we took the post-intervention measures of anxiety, heart rate and blood preassure as dependent variables. The independent variable was the intervention groups vs. control group. Finally, we took the preintervention measures as covariates. Thus, we assessed the effects of the intervention on the five groups, taking into account the prior levels of each group. A 5% confidence level was established.
Table 1 shows the Patients characteristics. The primary cancer was breast (21.5%), lymphoma (17.8%) and lung (15.9%). As regards the type of treatment received prior to the PET/CT study, the most frequent treatment was chemotherapy (16.7%), although a 29.3% had not yet started treatment.
Table 1: Patient characteristics. View Table 1
The motives for performing the PET/CT study were monitoring treatment response (41.5%), initial staging (31.5%), and detection of recurrence (27%). This was the first PET/CT study for the majority of the patients (55.9%), compared with 44.1% who had previously undergone one or more studies. The mean number of previous PET/CT studies per patient was 0.98 with a standard deviation of 1.52.
No antihypertensive treatment was required by 86.7% of the sample before PET/CT; nobody needed anxiolytic treatment due to anxiety crisis during the procedure. Prior to the PET/CT, participants exhibited no dyspnea (98.9%), digestive problems (98.1%), muscle stiffness (99.6%), or dizziness (93%). Similarly, after the test, they exhibited no problems of dyspnea or digestive problems (98.91%), muscle stiffness (99.6%), or dizziness (93.6%).
The PET/CT results showed that 59.6% of the participants tested positive for metabolically active tumor tissue, compared with 27.8% who tested negative for tumor viability with 18F-FDG affinity. An associated infectious inflammatory process was clearly detected in 7.4% of participants, while 5.2% presented doubtful findings which might be related to an acute infectious inflammatory process, but the existence of metabolically active tumor tissue could not be ruled out. As regards tumor staging, 32.6% exhibited no staging; the tumor was metastatic in 21.1%, localized in 28.5%, and locoregional in 17.8%. No artifacts were detected in the immense majority of patients (95.9%), meaning no problems were encountered for diagnostic interpretation. Artifacts were detected in 3.7% of studies as a result of movements and due to patient preparation only in the control group (χ2(2) = 7.010, p < 0.030). Presence of artifacts was never a consequence of Brown fat or muscle tension.
In Table 2, we can see the mean scores in subjective anxiety and STAI statistics before and after the PET/CT in all the sample.
Table 2: Descriptive statistics of the different pre and post-intervention measures of anxiety. View Table 2
Regarding the effectiveness of the different interventions (Figure 1), we found a significant effect on the level of post-intervention subjective anxiety, controlling for the effect of pre-intervention anxiety levels (F, 236.280; p = 0.001; η2 partial = 0.81). Statistically significant differences were found between the control group (5.41) and the written information (4.64), music (1.15) and hypnosis (0.70) in the corrected means of the level of post-intervention anxiety.
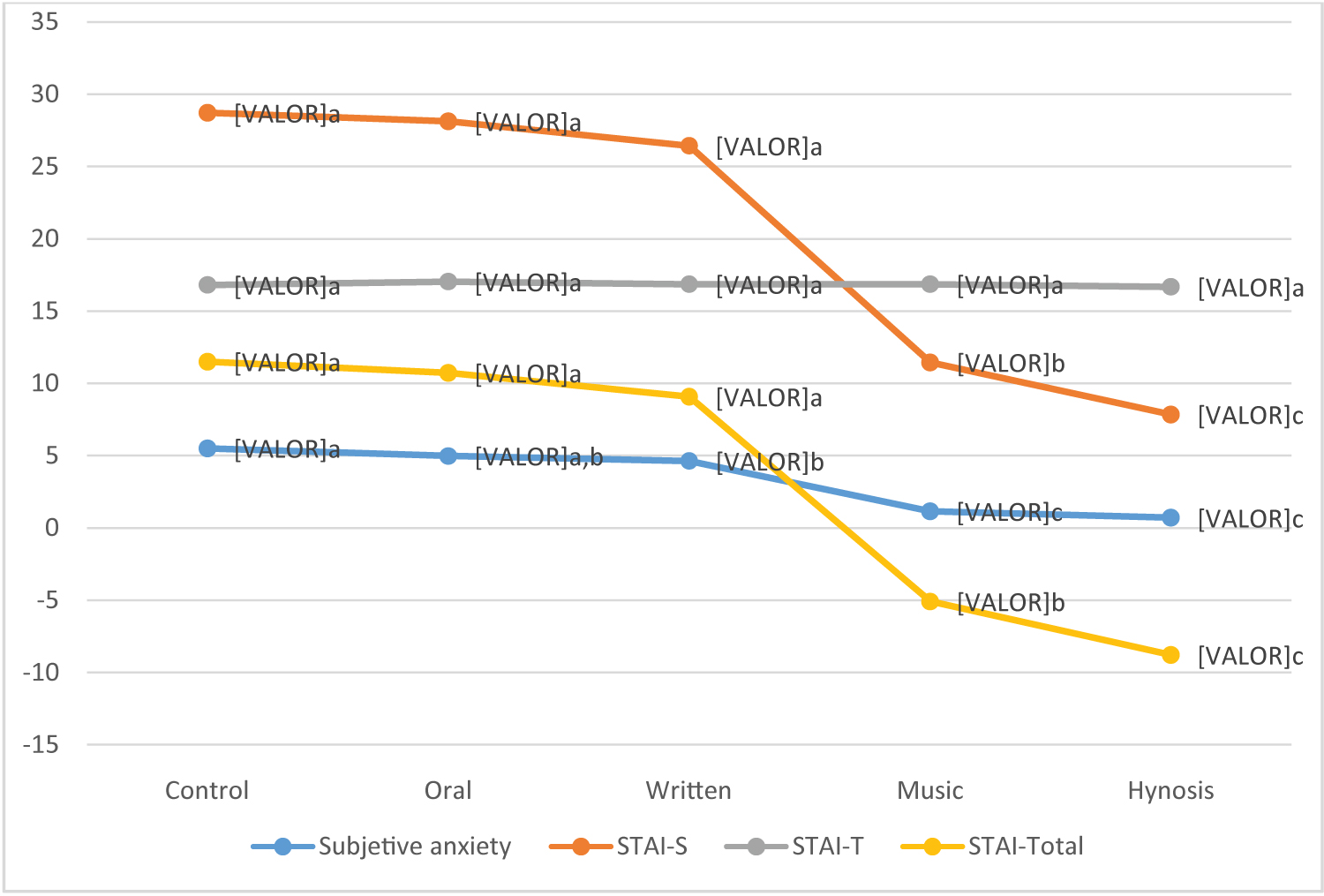 Figure 1: Significant differences between interventions in anxiety measures.
Figure 1: Significant differences between interventions in anxiety measures.
Y-axis -Medial marginal estimada
View Figure 1
With respect to the effectiveness of interventions on the post-intervention STAI state anxiety score, controlling for the effect of the pre-intervention STAI state anxiety, we found significant differences between the intervention groups and control (F, 223.272; p = 0.001; η2 partial = 0.80). The hypnotic induction group (7.85) and music group (11.46) presented lower mean scores on the post-intervention STAI state anxiety, showing statistically significant differences between them, as well as, with the control group (28.71), oral group (28.11) and written group (26.43).
The post-intervention STAI trait anxiety score yielded no significant differences between groups. This suggests that almost all the variabilities in the post-intervention STAI trait anxiety scores were explained by the level of the preintervention score. This confirms the stability of this variable, which coincides with our prior expectations based on trait anxiety being a personality characteristic.
Results for the post-intervention total STAI score reveal statistically significant effects for both the covariate (pre-interventiontotal STAI) and the intervention groups (F, 120.913; p = 0.001; η2 partial = 0.69). On assessing the means of the post-intervention total STAI scores corrected for the effect of the covariate, we found statistically significant differences between the control group (11.50), oral information group (10.72) and written information group (9.07) with music group (-5.09) and hypnotic induction group (-8.79), as well as significant differences between the latter two, presenting lower levels than the other groups.
In relation to physical data, the post-intervention heart rate, we did find statistically significant differences controlling for the effect of the pre-intervention heart rate (Table 3). This model explains 79% of the variance of the post-intervention heart rate. On assessing the means of the post-intervention heart rate scores corrected for the effect of the covariate, we found statistically significant differences between the control group (73.15), oral information group (74.69) and written information group (73.50) with the music group (69.17) and hypnotic induction group (68.51).
Table 3: Results of the ANCOVA on the post-intervention heart rate score. View Table 3
Finally, for the post-intervention systolic blood pressure variable, we found statistically significant effects of the covariate (pre-intervention systolic blood pressure) with experimental groups (F, 187.834; p = 0.000; η2 partial = 0.78). The corrected means of post-intervention systolic blood pressure show statistically significant differences between the control group (132.93), oral group (132.79), written group (134.18) with music group (128,55) and hynosis group (128.31). Similar results were found in post-intervention diastolic blood pressure (F, 126.007; p = 0.000; η2 partial = 0.70). Controlling for the effect of the covariate (diastolic blood pressure) statistically significant differences were found between the control group (75.41), oral information (74.72) and written information (77.02) with music (70.20) and hypnosis groups (69.49) in the corrected means of the level of post-intervention in diastolic blood preassure.
This paper has measured the level of anxiety (subjective and objective) and has comparatived study of the effectiveness of different interventions for the reduction of anxiety in a sample of cancer patients that go to the Nuclear Medicine Service for the accomplishment of an 18F-FDG-PET-TAC.
In relation to the data collected for the socio-demographic presents higher numbers of people who do not work because of retirement and sick leave since they are cancer patients (331).
With respect to the presence of cancer, our work indicate that the primary location of the tumor for which the patients were to undergo a PET/TC study was the lymphatic system, followed by the breast, gynecological system, andlung. These data are similar to those of other studies (NCCN guidelines; SEOM). Besides, this high number of lymphomas is due to the fact that PET-CT is the most useful diagnostic tool in this pathology and it is so frequent among young people. Chemotherapy is the most frequently administered treatment, according to international guides and protocols [21].
The participants exhibited no dyspnea, digestive problems, muscle stiffness, or dizziness either before or after undergoing the PET/CT. It is also worth noting the lack of artifacts generated during the test [8-11,20] as a result of patient movement or muscle tension, with the subsequent accumulation of brown fat, in our experimental group.
The most common reason for implementing the PET/CT studies was to monitor treatment, followed by initial staging and detection of recurrence. For most of the participants, however, this was their first experience of a PET/CT test, and for alarge number, no antihypertensive treatment took previously. Indeed, in our study, nobody needed anxiolytic treatment during the procedure; this finding is important since many studies report the need to administer anxiolytics [16-18]. We find that most participants have no psychopathological history of anxiety or depression.
Focusing on the aim of the present work, total STAI score indicated the appearance of subjective and objective preintervention anxiety such as previous studies [1,3,5-7]. However, post-interventions, both the level of subjective anxiety and the standardized indicators, decrease. This finding highlights the effectiveness of an interventions of the type administered in the current study in reducing both subjective and objective anxiety. For that, is needed to perform some interventions to improve or reduce these high anxiety levels [9,23]. Studies previous have tried different type of interventions [4,5,9,11-13,16,18,19,21,24-26].
As regards the effectiveness of the intervention conducted in the present study, as expected, statistically significant differences were found between some experimental groups (music and hypnosis) and the control group in all the post-intervention anxiety measures (level of subjective anxiety, STAI state anxiety, and STAI total anxiety). Further more, the experimental groups of music and hypnosis were effective in reducing post-intervention HR and BP (sistolic and dyastolic). In contrast, the post-intervention STAI trait anxiety score showed no significant differences between groups. Trait anxiety reflects a relatively stable emotional state and measures a person's general tendency to perceive day-to-day situations as threatening, as well as the person's baseline feelings and personality structure [30]. Besides, we results show how trait anxiety and state anxiety are theoretically independent constructs.
Specifically, oral information intervention did not show significant differences among any variable. It is an interesting result because the patient in PET-TAC should be informed. The patient should receive clear, complete and personalized information so as to make him feel welcomed, and doubts and concerns should be answered in order to generate a climate of trust in which patientes understand everything related to the problem and can express hisemotional state. A patient who has been well informed about pathology and treatment is better suited to the different situations and his anxiety or other emotional responses are thus reduced; he better understands the explanations received and is more satisfied with the relationship with the professional [4,32-35]. It is necessary to ensure good and individual information regarding their pathology and the consequences it will have for them, the treatment they will have to undergo. This information will promote maximum possible well-being and reduction suffering [1]. Future researchs are neccesary to know the elements in the comunication in the relaionship doctor-patient with the proposal to be more effective.
Similar results were found in written information group. This intervention did not find any significant differences among any variable. Various techniques by which to improve the care and education of patients undergoing interventional techniques or complex diagnostic procedures have been developed, such as the development of informative leaflets or graphic medicine with illustrated stories, comics and cartoons. However, in PET/CT there have been few studies which have analized this goal, for this reason, it is difficulty to conclude about the effectivenees of written information.
In our study, we provided an informative leaflet in the form of a triptych made ex profeso in which it is explained in a simple way in which PET- process to which the patient is going to submit, allowing the opportunity for the patient to clarify the doubts that have arisen once read all the information. Maybe, our leaflet had methodological problems or had no atracttive, etc. In the future, other studies should study which elements must contain the written documents delivered to patients in the PET/CT service to ensure that they are effective. Even in the future, is necessary to know the impact of written information presented in other formats, such as cartoons, comics or graphic stories, must be expanded and evaluated.
As regards, listening to music intervention, we found positive results with a significant differences in anxiety levels (subjetive and objetive) and psysical data (HR and BP). Some studies have showed the effectiveness of music in different medical procedures [36-40] even in PET/CT study [5,11,14]. These studies found low anxiety levels and HR in patients after PET/CT scan and they suggest how listen to medidative music can distract patients' attention or avoid feeling uncomfortable before PET/CT scans. In conclusión, Relaxing meditative music can be used as a relaxation and anxiolytic mechanism as an integral multimodal part in patients during the uptake phase before PET-CT studies. Besides, reducing anxiety has the potential to decrease the risk of false positives and improve image quality and image in the absence of artifacts.
Listening to music is safe, inexpensive, easy to implement, relieves anxiety, and helps maximize efforts to promote comfort and relaxation for PET-CT patients. Therefore, it is encouraged to include initiatives such as the one presented in this paper.
Finally, the hypnotic induction intervention was effective with significant differences in anxiety levels (subjetive and objetive) and psysical data (HR and BP). Hypnosis has been used in other medical invasive procedures and cancer patients to reduce anxiety and pain [24-26,36,41-45]. In PET/CT scan this technique has not been used and can be new, however, our data showed how a hypnotic induction intervention has been effective in all studied variables. This intervention, contained background music and sounds of nature over which an off-voice made descriptions in order to guide the patient and induce a state of deep relaxation and medidative with the fomentation of self-observation and the acceptance. These elements or other can be responsable of effectivite of this hypnosis intervention, for that we need more studies similar to this, to know the relation among the elements. Thus, it would be interesting to investigate these components and the role actually played by awareness and the nonjudgmental attitude towards thoughts in the therapeutic effectof hynotic induction intervention. But, we can conclude how a hynosis intervention reduce anxiety and psysical data. Beides, hynosis induction intervention, does not give rise to the appearance of artifacts that could hinder the analysis of the images.
Therefore, in light of the results, hypnotic induction such as the one presented here, by means of an audio recording, is postulated as an effective, useful and easy-to-apply tool to manage and reduce anxiety in patients who undergo it. An 18F-FDG PET-CT study. It seems clear there lies ahead a fascinating quest to clarify the specific elements needed in hyposis-based intervention to ensure its effectiveness in clinical populations.
Following the results obtained in this study, we can conclude that patients who are submitted to a PET/CT study have high subjective anxiety and measured by STAI standardized questionnaire. None of the music and hypnotic induction interventions presented artifacts which allow an adequate evaluation of PET/CT. Oral information and written information did not show significant differences in any of the variables. In contrast, music and hypnotic induction interventions obtained significant differences in the variables of anxiety measured objectively and subjectively, the BP and the HR. Finally, the conclusion of music and hypnotic induction interventions would be a great advance in the quality of care of our patients and in our own and would show an act of courage from the services of Nuclear Medicine to want to change things betting on innovation with present interesting and important proposal. It is recommended to use hypnosis and music interventions to reduce physical and emotional discomfort during the PET/CT procedure and to improve the quality of life of patients in nuclear medicine service.
In relation to our study limitations, the first limitation involves the sample size and the geographical location of the population, which might be considered unrepresentative when attempting to generalize the findings. The second limitation referes the ad hoc questionnaire and its possible lack ofvalidity and reliability. Finally, the limited existence of research and evidence on the use of hypnosis, music or written information in nuclear medicine opens the door to important new projects since there are currently no programs of this type in the national health systems. These type of interventions would be a valuable improvement of great use in the treatment of patients with cancer undergoing 18FFDG-PET/CT diagnostic tests.
No conflict of interest.