Thoracic ganglioneuromas are exceedingly rare. They arise from neural crest cells. These tumors are mostly asymptomatic, but massive tumors can present symptoms related to locoregional compression like dyspnea or scoliosis. We report a case of thoracic paravertebral giant ganglioneuroma in a 12-year-old child presenting as a large intrathoracic mass in the posterior mediastinum with intimate contact with the dorsal spine. That masse causes skeletal deformity and scoliosis. Scoliosis secondary to ganglioneuroma is rare and there is no report on its incidence. The diagnosis was made on a CT-guided tarnsparietal biopsy. Our intent is to highlighting the difficulties that may occur during the diagnosis of such patients, especially in view of the unusual clinical signs and the large size of the tumor. As well as the management of paravertebral ganglioneuroma associated with scoliosis, especially in the preoperative phase.
Thoracic ganglioneuromas are rare nerve tumors and there are very few cases reported in the literature [1]. They belong to the group of neurogenic tumors arising from sympathetic ganglion cells [2]. Only a few cases of ganglioneuroma with scoliosis have been reported in the literature. In this report. The authors report a case of thoracic paravertebral giant ganglioneuroma in a 12-year-old girl who presented with scoliosis. it's one of the largest ganglioneuroma have been reported in children, there's only one observation in an 8 year old that describes a tumor larger than ours [3]. Through our observation, we propose to review its clinical peculiarities, its radiological aspects and the significant diagnostic challenge given the rarity of this entity. The study and analysis of the case improved the knowledge of this tumor.
A 12-year-old child without a medical history significant, had been presented witha progressive shortness of breath without other respiratory or extra respiratory associated signs. The child had no loss of weight, and his appetite was good. The clinical examination objectified the presence of a scoliosis attitude and a condensation syndrome of the right hemithorax, there were no abnormalities on nervous system examination.
A chest X -ray revealed a large round opacity occupying approximately two-thirds of the right hemithorax, which were well limited. The inner limit of this opacity was drowned in the mediastinum (Figure 1). Computed tomography of the chest depicted a large mass occupying the right posterior mediastinumwith regular and well-limited borders and measuring 18.7 × 10.4 × 8.7 cm (Figure 2). The lesion was hypodense (20UH), homogenous with vascular trabeculae and was not enhanced after injection of contrast agent (24UH). This mass had intimate contact with the dorsal spine with a scoliosis attitude and minimal endo-canal extension at the height of D7, without detectable bone lysis. The tumor had intimate contact with the aorta, esophagus, bronchial tree, pulmonary veins and left atrium that itharmoniously pushed forward and to the left (Figure 3). Furthermore, there were no signs of locoregional invasion.
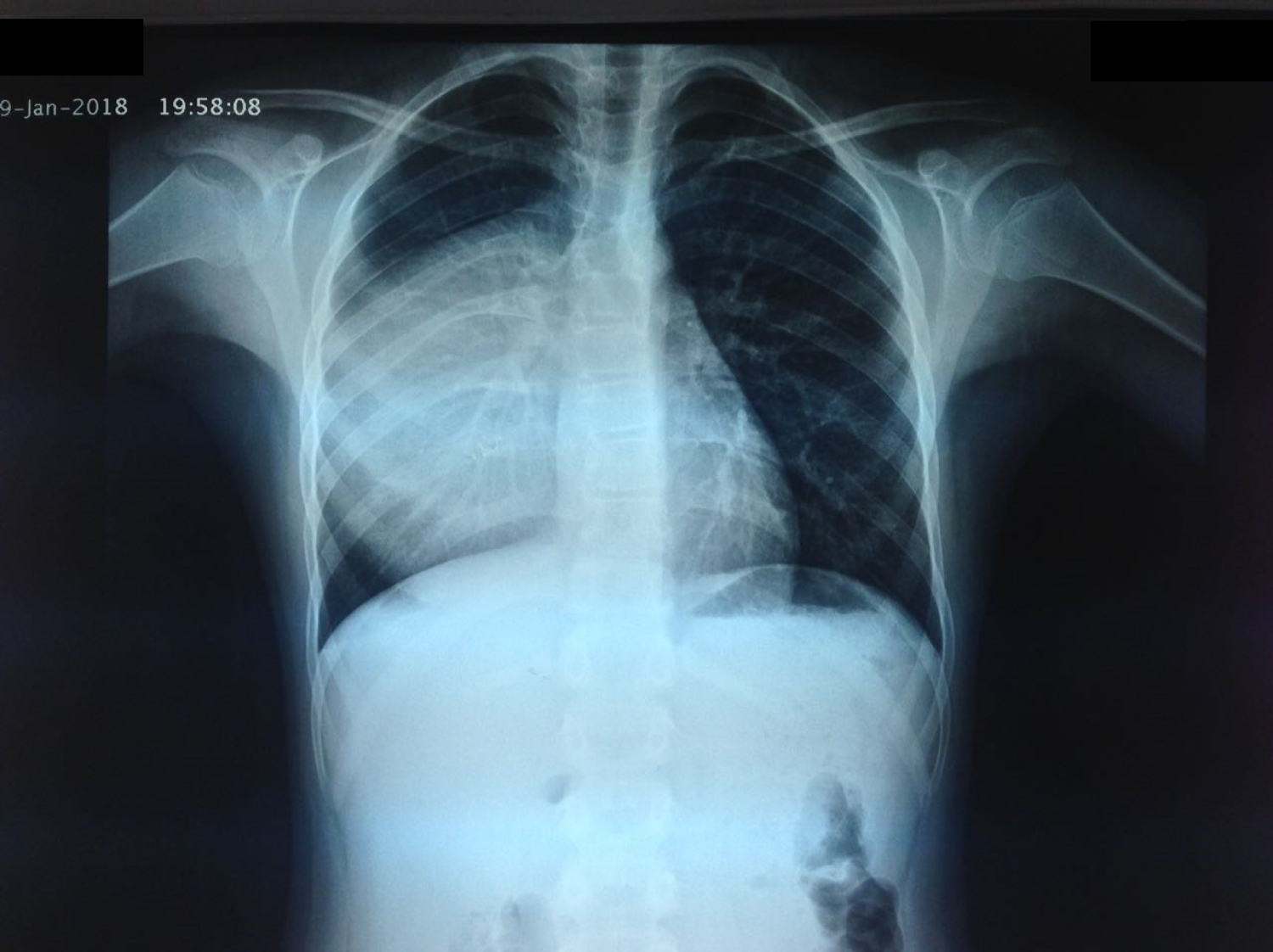 Figure 1: A chest X-ray revealed a large round opacity occupying approximately two-thirds of the right hemithorax, well limited.
View Figure 1
Figure 1: A chest X-ray revealed a large round opacity occupying approximately two-thirds of the right hemithorax, well limited.
View Figure 1
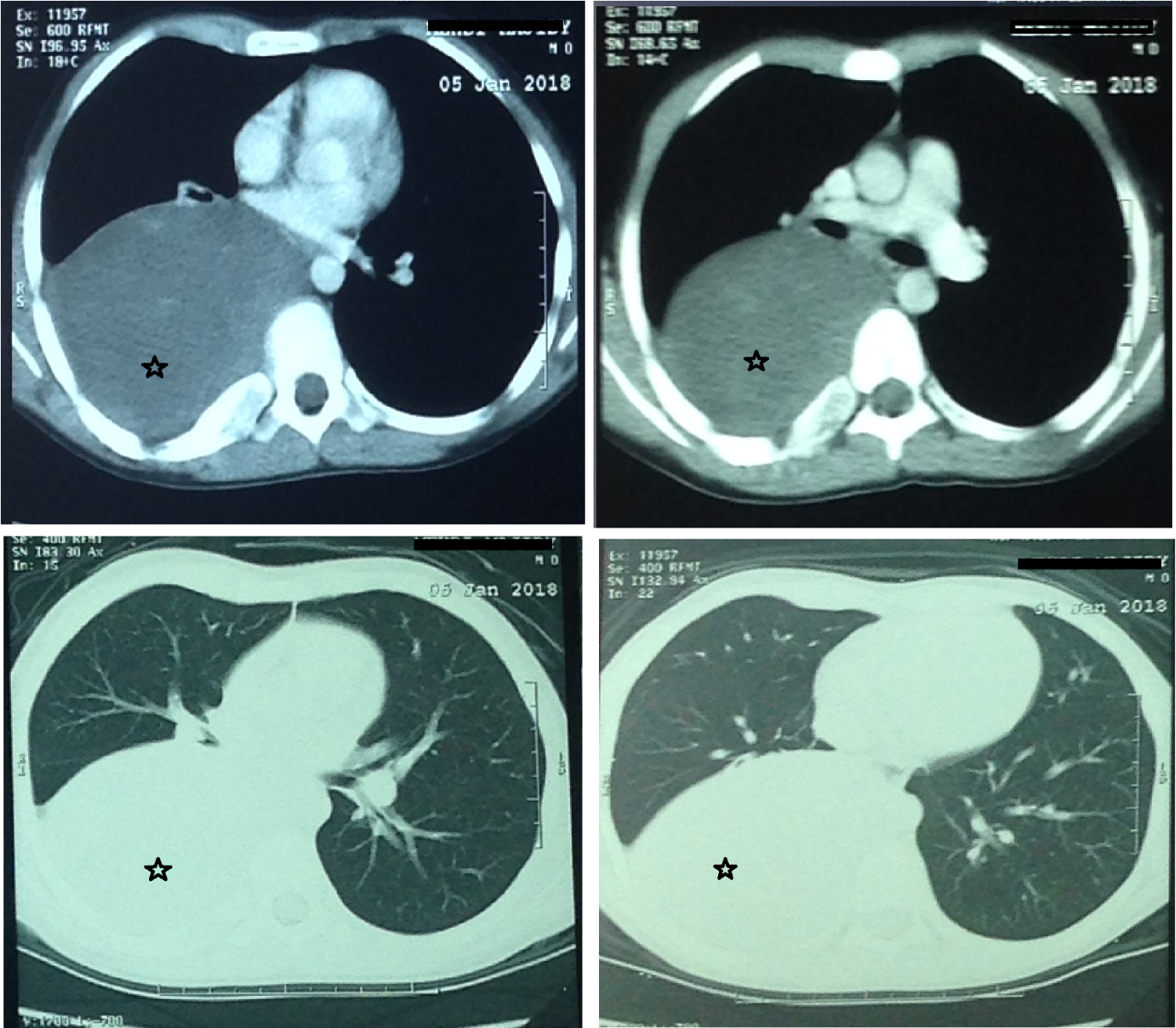 Figure 2: Mass occupying the right posterior mediastinum with regular and well-limited borders, measuring 18.7 x 10.4 x 8.7 cm (stars).
View Figure 2
Figure 2: Mass occupying the right posterior mediastinum with regular and well-limited borders, measuring 18.7 x 10.4 x 8.7 cm (stars).
View Figure 2
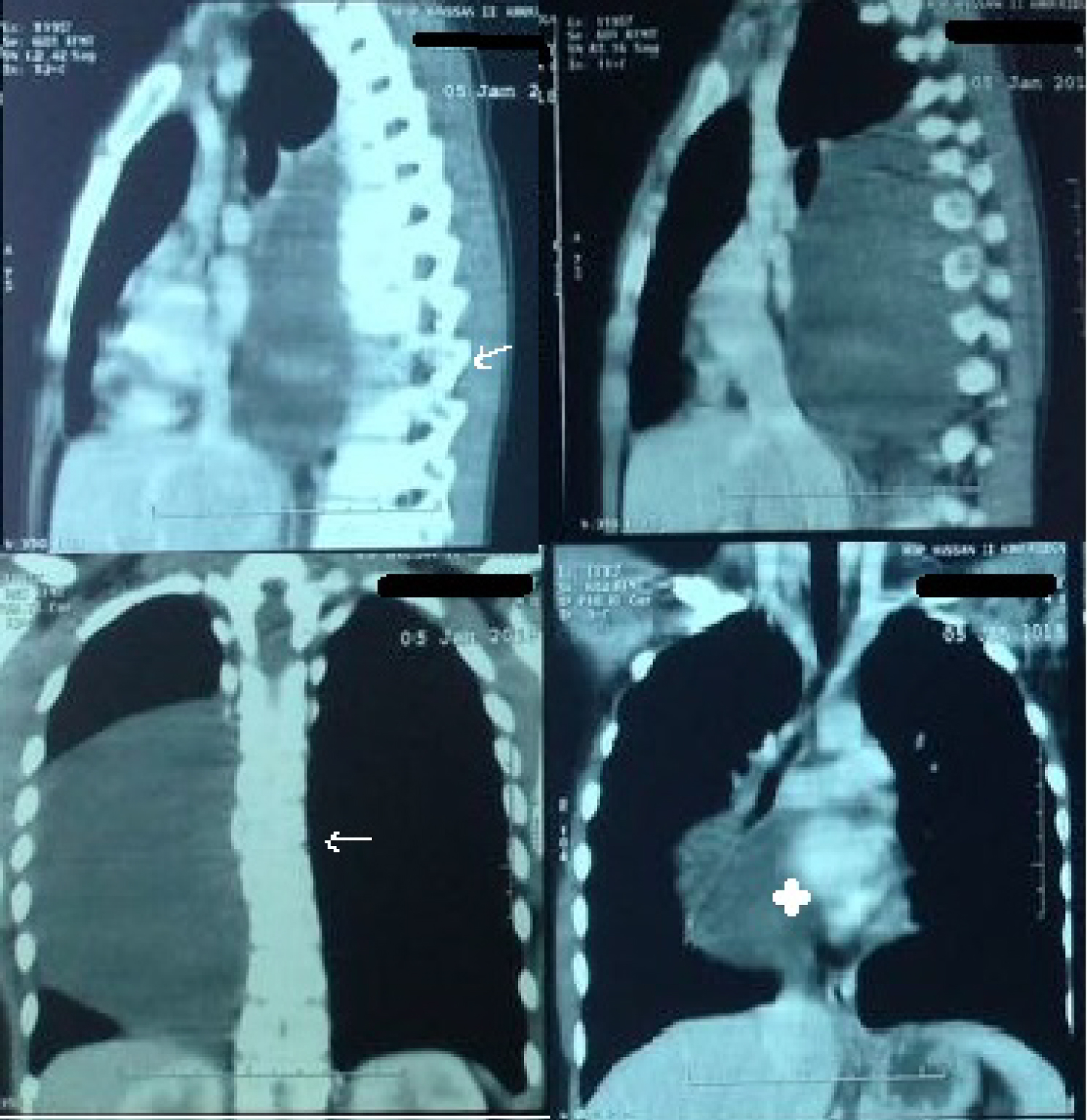 Figure 3: Chest CT scan shows that the mass has an intimate contact with the dorsal spine with scoliotic attitude (arrow), intimate contact with the the mediastinal components and left atrium that it harmoniously was pushed forward and to the left (star).
View Figure 3
Figure 3: Chest CT scan shows that the mass has an intimate contact with the dorsal spine with scoliotic attitude (arrow), intimate contact with the the mediastinal components and left atrium that it harmoniously was pushed forward and to the left (star).
View Figure 3
The radiological findings were compatible with a benign posterior mediastinal mass. The differential diagnosis included ganglioneuroma, Schwannoma, neurofibroma, paraganglioma and neuroblastoma.
A CT-guided transthoracic biopsy was performed under local anesthesia. Histological study of the specimens showed benign tumor proliferation consisting of wavy cells with tapered bumps and with an elongated nucleus without cyto-nuclear atypia or mitosis. That proliferation was organized in bundles with clear nerve differentiation and included mature ganglion cells in places (Figure 4). The morphological aspect was compatible with a ganglioneuromas.
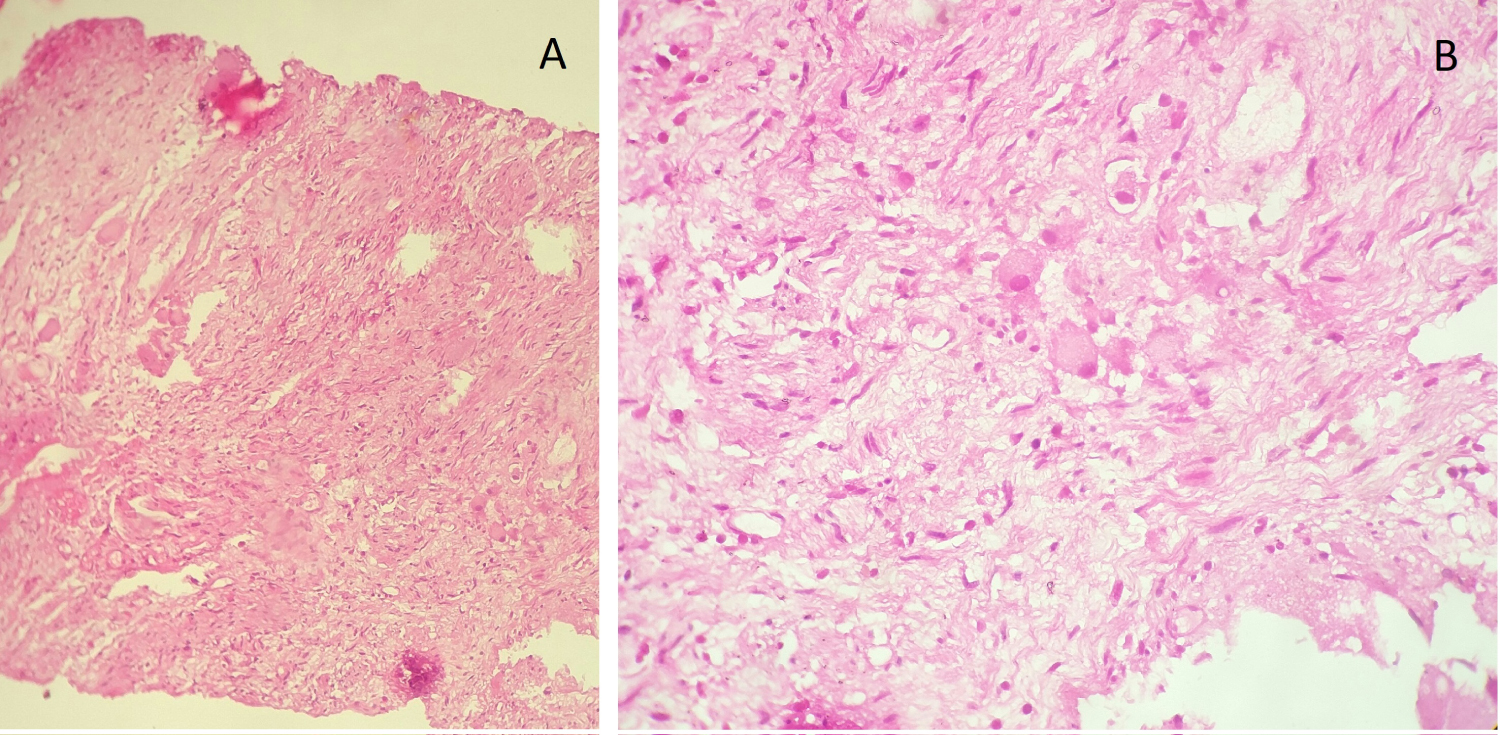 Figure 4: Histologicalanalysis : ganglion cells with an abundant eosinophilic cytoplasm which is well limited. These cells are surrounded by Schwann cells which have a spindle-shaped appearance and are distributed in a disorderly manner. A) High magnification (20×) microscopic; B) High magnification (40×) microscopic.
View Figure 4
Figure 4: Histologicalanalysis : ganglion cells with an abundant eosinophilic cytoplasm which is well limited. These cells are surrounded by Schwann cells which have a spindle-shaped appearance and are distributed in a disorderly manner. A) High magnification (20×) microscopic; B) High magnification (40×) microscopic.
View Figure 4
A multidisciplinary discussion including pediatric surgeon, neurosurgeon and the orthopedic surgeon was necessary to discuss the surgical approach in this patient. Due to the size of the ganglioneuroma in this case, the proximity of the mass to the spine and mediastinal structures, a thoracotomy was the safest approach as it allowed for timely intervention in event of an operative complications. The scoliosis was minimal and early in onset and had not required orthopedic intervention.
The patient successfully underwent tumor resection via right posterolateral thoracotomy, an exploration has found a posterior mediastina tumor at the expense of the thoracic sympathetic chain. The tumor was firm,well encapsulated and was not invading any of the adjacent structures. The mass was in proximity to the spine, but there was no intramedullary invasion, so there was no need for neurosurgical intervention. The surgical section slice was whitish in appearance with a fibrous capsule. The tumor was removed in its entirety. Postoperative course was unremarkable, the patient was discharged on the 7th Day. The 24-month follow-up period had not revealed any recurrence or metastasis.
The ganglioneuroma is a rare benign nerve tumor of neuro-ectodermal origin [1]. It belongs to the group of neurogenic tumors developed at the detriment of ganglionchains sympathetic, a group that also includes ganglioneuroblastoma and neuroblastoma [1,2]. The incidence of ganglioneuromais not well documented, but it is estimated to characterize 0.1 to 0.5 % of total central nervous system (CNS) tumors [4]. The ganglioneuromas usually occur in the posterior mediastinum or are more commonly retroperitoneal. About 40% of these tumors occur in the posterior mediastinum [5].
The ganglioneuroma may remain asymptomatic for a number of years, to be discovered incidentally on a chest X-ray [2,6]. Most of cases in the literature were asymptomatic (Table 1). However, theses lesions are capable to grow to a significant size and become symptomatic and displace or compress the neighboring organs. Review of systems may identify symptoms of mass effect including pain, dysphagia, dyspnea, stridor, cough, or Horner's syndrome [19]. In our observation, the tumor attained a large size, which was causes local mass effect on the mediastinal structures and the spine, resulting shortness of breath and spinal deformation.
Table 1: Literature review for the thoracic ganglioneuroma. View Table 1
On review of current literature, this is the second largest ganglioneuroma reported in paediatric patients. Guan, et al. reported a case with a tumor of 21 × 15 × 18 cm in an 8-year-old child [3]. The largest tumor was reported by Lambdin, et al. but it was in an adult patient (24 × 10 × 10) [20] (Table 1).
Paravertebral ganglioneuroma and scoliosis is rarer and has only been sporadically reported. There are 13 different articles dealing with ganglioneuroma and scoliosis [7-17]. There are three types of paravertebral ganglioneuroma and scoliosis: 1) The tumor grows e expansively, leading to damages in the side and front vertebrae and eventually to scoliosis; 2) Scoliosis is mechanically stimulated, induced the tumor; 3) paravertebral ganglioneuroma and scoliosis occur simultaneously [19].
In our observation, the deformity was not very obvious, and so the patient and his parents neglected the scoliosis. the diagnosis allowed resection of the tumor and preservation of the spine. the child avoided a serious orthopedic operation which can be a source of post-operative complications.
The radiological diagnosis of this tumor is complicated by the variability of its aspects [6]. Before injection, the tumor is homogeneous, hypodense, with regular and well limited borders. After injection, the contrast agent uptake is low to moderate and the mass is being heterogeneous or staying homogeneous [2]. In magnetic resonance imaging (MRI), the ganglioneuroma appears as a homogeneous hyposignal on T1-weighted MRI, and is hyper or isosignal on T2-weighted MRI (based on the quantity of stroma in the lesion) [2,6].
The thoracic ganglioneuroma represents a diagnostic challenge and creates a problem of differential diagnosis with other intra-thoracic tumors. Notably neurogenic tumors including other neuroblastic tumors (ganglioneuroblastoma and neuroblastoma) and nerve sheath tumors (mainly neurofibroma) [21].
Transthoracic needle biopsy has a sensitivity of 90% for intrathoracic pathology [22], and provides valuable information which helps in making decision in many cases of intrathoracic pathology as for was the case in our observation.
Microscopically, these tumors contain large ganglion cells and show areas with smaller lymphocyte-like cells within a matrix of fibrous stroma and Schwann cells. The distinction from a malignant tumor is based on the absence of necrosis or the presence of immature ganglion cells [23].
The treatment is surgical, consisting of tumor resection [1,2]. A thorough preoperative assessment is mandatory to help plan surgery accordingly. These tumors have traditionally been approached by thoracotomy but the thoracoscopic approach has gained acceptance since Landreneau's description in 1992 [24]. Cardillo, et al. concluded that video-assisted surgery (VATS) was associated with low morbidity and mortality and a shorter postoperative stay [25]. The possibility of applying VATS depends on tumor size and intramedullary extension.
We chose to perform a thoracotomy, since thoracic surgery implies an increased risk of vascular or nerve damage, and also to better manage a possible spread of the tumor in the spine.
Thoracic ganglioneuromas have the potential to cause compressive symptoms if they grow up to a significant size, and they should be included in the differential diagnosis of intrathoracicmasses.
The feature of our observation is the presence of symptomatic clinical signs, the large size of the mass causing spinal deformity. A careful preoperative examination is crucial for patients diagnosed with paravertebral ganglioneuroma and scoliosis.
None.
This research received no specific grant from any funding agency in the public, commercial or non-profit sectors.
Obtained.
I declare that the authors have attributed to the manuscript.