The interruption of the cardiac conduction system that occurs in the ventricles, anatomically after the electrical impulse leaves the atrioventricular node, generates bundle branch block. With a particular electrocardiographic morphology, specific measurable and revealing of its topography, it may be related to underlying cardiac pathology, although it also exists in hearts without pathology. Compared to adults, there are more frequent patterns of presentation in the paediatric age, such as right bundle branch block, especially incomplete right bundle branch block. Recognition of this electrocardiographic disorder is important, as it may be a marker of underlying cardiac pathology.
Depolarization of myocardial cells leading to cardiac contraction occurs in an orderly and sequential manner via the cardiac excitoconductive apparatus. The impulse starts in the sinus node, expanding to the atrioventricular (AV) node, where it spreads the activity to the ventricles via the bundle of His through its two main ventricular branches, the left and the right, continuing through the Purkinje fibers. The impulse is transmitted simultaneously to the left and right ventricular myocardium (Figure 1).
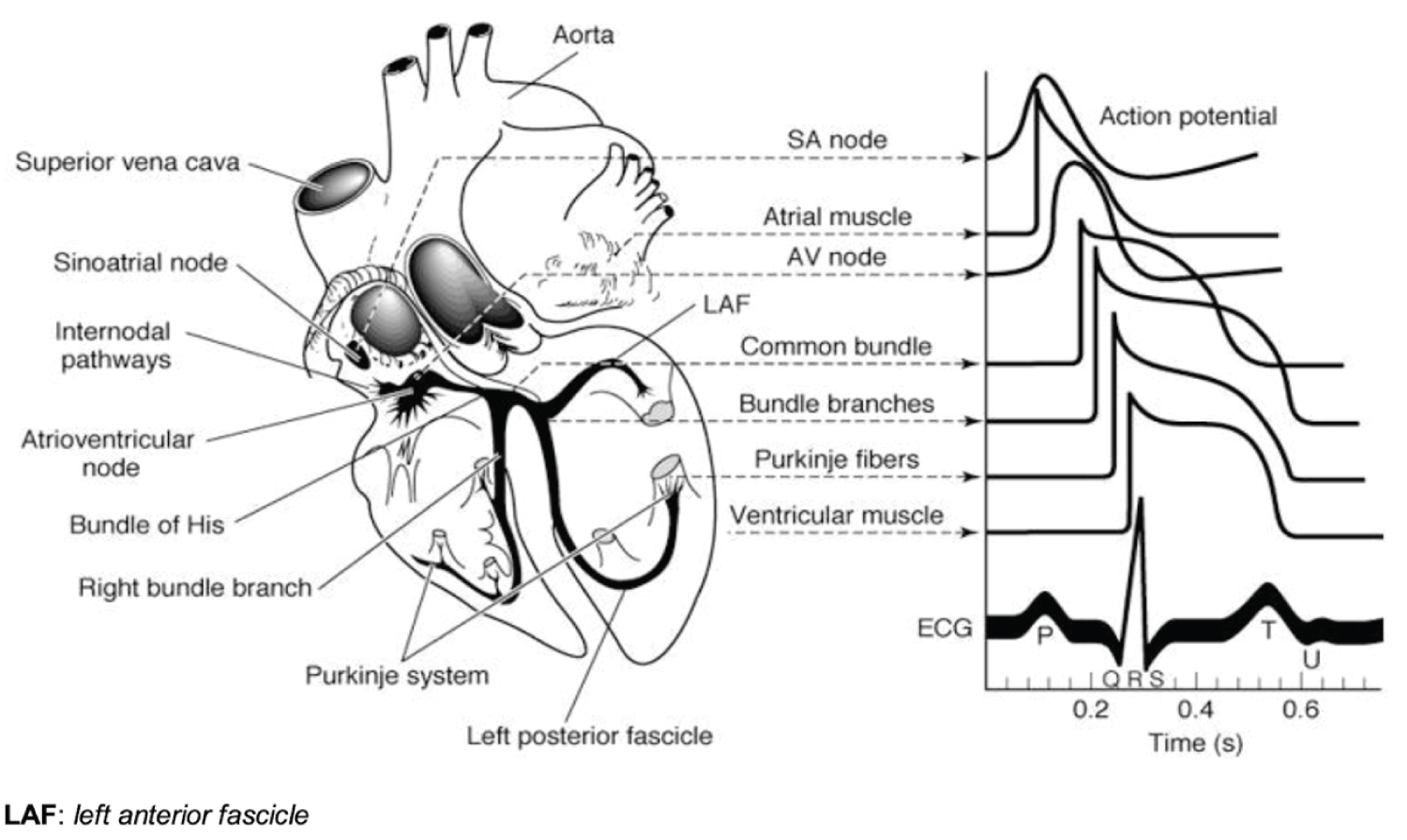 Figure 1: Cardiac excito-conductive system.
View Figure 1
Figure 1: Cardiac excito-conductive system.
View Figure 1
When an interruption in that transmission occurs, branch locks are caused. They are classified topographically, according to the location of the interruption of the electrical impulse, being called right bundle branch block (RBBB) or left bundle branch block (LBBB) with electrocardiographic peculiarities that make them recognizable.
The left main branch is in turn divided into two, the left anterior fascicle and the right posterior fascicle. Conduction disorders that involve only the anterior or posterior branch of the left ventricle are known as hemiblocks or fascicular blocks.
A possible medial or septal tract in the left conduction system that could have implications has been studied. The origin of the fibers of this fascicle is variable: In most cases they come from the posterior branch, less frequently from the anterior branch and in very few cases they are independent. In addition to being extremely difficult to identify the alteration of the medial fascicle on the electrocardiogram (ECG), it has no clinical significance [1].
The pathophysiological changes of bundle branch blocks are due to the fact that the electrical stimulus first depolarizes the healthy branch and then, through the myocardium with slower conduction, the ventricle with the affected branch, causing a delay in depolarization. The electrocardiographic translation of this event is a vector of cardiac depolarization oriented towards the problem ventricle [2,3]. Identifiable changes in the ECG can be interpreted in both depolarization and repolarization waves in cases of complete blocks [4]. Mainly we would perceive the widening of the QRS proportional to the severity of the block, anomalous T wave and deviation of the QRS axis. All ECG parameters are quantifiable and, in the case of pediatrics, they are standardized according to age.
The right branch is shorter than the left and innervates a small myocardial mass, so its interruption in isolation is more prevalent [5].
It is often found in subjects without evidence of structural heart disease. Less frequently it is found in the context of ischemia or cardiomyopathy. In general, it is considered a benign finding and a favorable prognosis [6].
Complete right bundle branch block (CRBBB): Its prevalence increases with age, unlike incomplete right bundle branch block (IRBBB). Full grade presentation is not common in children with a structurally normal hearts [7].
A CRBBB can be found in relation to the following pathologies:
• Congenital causes: Atrial septal defect, arrhythmogenic right ventricular cardiomyopathy, Brugada syndrome, Ebstein's anomaly or coarctation of the aorta in infants.
• Acquired causes: Ischemic heart disease, degenerative conduction system disease.
• Due to right ventricular overload: Right ventricular hypertrophy, chronic pulmonary disease, pulmonary thromboembolism, pulmonary hypertension.
• Iatrogenic etiology: After catheterization or cardiac surgery (ventricular septal repair or tetralogy of Fallot).
• Treatment with antiarrhythmics, tricyclic antidepressants, diphenhydramine, chloroquine, digoxin.
• Other causes such as aberrant conduction or asthma phenomenon, electrolyte disturbances such as hyperkalemia, poisoning (arsenic).
The defining electrocardiographic findings of complete RBBB are summarized in Table 1 and Figure 2 [4].
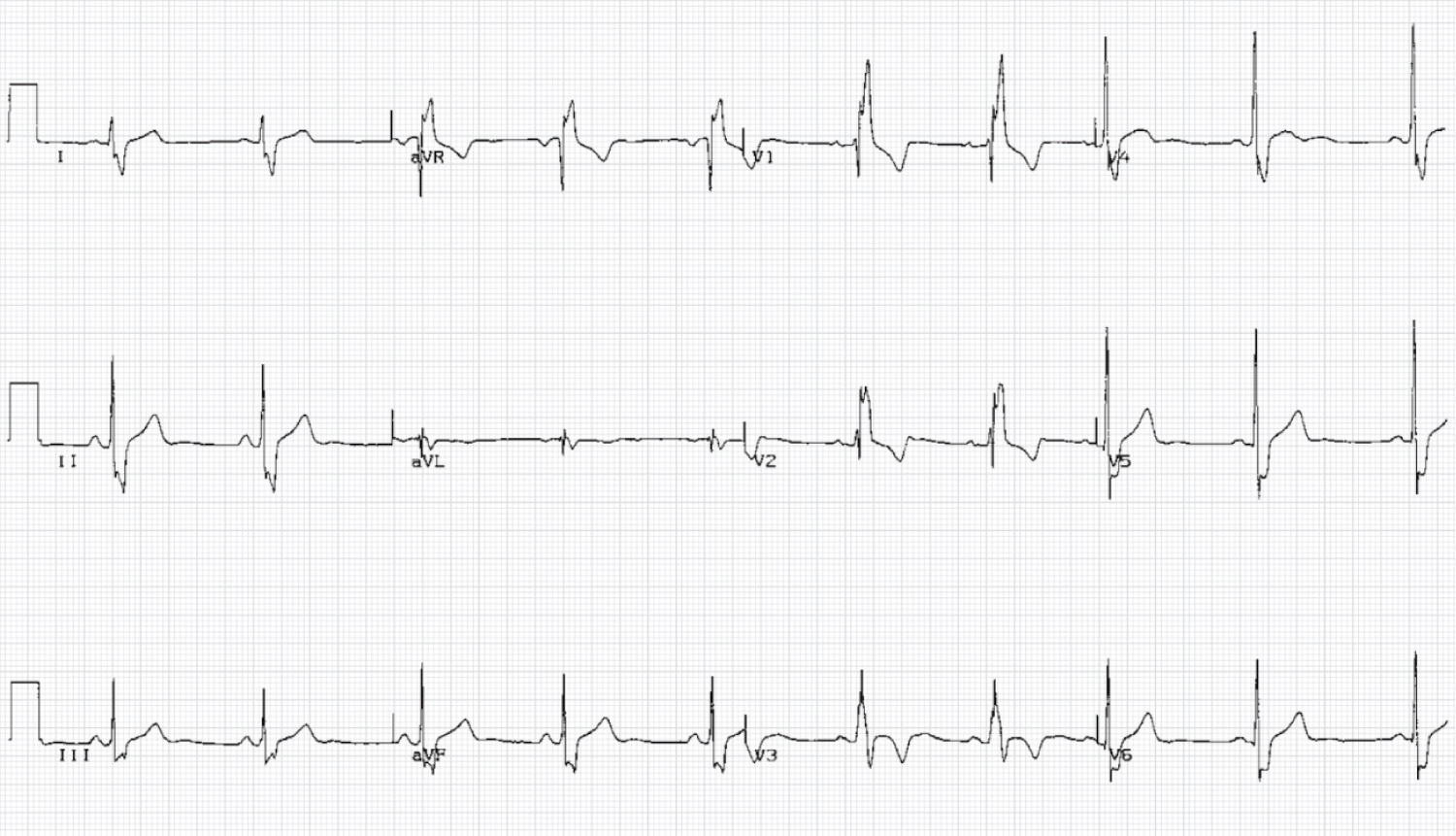 Figure 2: ECG with complete right bundle branch block.
View Figure 2
Figure 2: ECG with complete right bundle branch block.
View Figure 2
Table 1: Diagnostic criteria for complete right bundle branch block. View Table 1
The prognosis and treatment of RBBB is largely tied to the severity of the underlying heart disease and the possible presence of other conduction disturbances. Long-term health expectations are generally excellent in patients without apparent heart disease, while those who present it as comorbidity have worse results [8].
Incomplete right bundle branch block (IRBBB): It is very prevalent in pediatrics but its pathological significance has not been demonstrated in a previously healthy child. Nuclearly defined in the ECG as rsr', rsR', rSR' or RsR` pattern in V1 above all (also less V2). This right conduction delay presents a slightly longer than normal QRS duration but not enough to meet criteria for complete block.
It can be seen in up to 10% of children and is a cause for concern for some pediatricians. It is especially frequent in infants since the QRS vector is normally straighter and more anterior at these ages, due to the persistence of right ventricular predominance of perinatal origin, being a variant of normality. In older children and adults this pattern is unusual.
The diagnostic utility of an isolated IRBBB on ECG in healthy children is limited by its lack of diagnostic specificity, and does not require further evaluation [9].
Within the organicity, and as a frequent fact, it can be observed in children with atrial septal defects without this data defining this underlying pathology, so that in isolation it should not lead us to this diagnostic hypothesis [10,11].
It can also be a dynamic electrocardiographic finding in Brugada Syndrome, being its differential diagnosis important [12].
Table 2 shows the BIRD [4] electrocardiographic criteria. In Figure 3 we can see a plot.
 Figure 3: ECG with incomplete right bundle branch block.
View Figure 3
Figure 3: ECG with incomplete right bundle branch block.
View Figure 3
Table 2: Diagnostic criteria for incomplete right bundle branch block. View Table 2
As a special consideration, in children who practice competitive sports we can see a RBBB of variable degree in relation to the physiological and structural modifications that take place in the right ventricle. This finding in the absence of clinical symptoms or abnormalities in repolarization should not be interpreted as an underlying cardiac pathology, nor would it be associated with future cardiovascular events. Therefore, it does not require further evaluation [13,14].
It occurs with the interruption of the electrical impulse through the left branch of the bundle of His. It can happen completely or partially affecting some of its fascicles, left anterior or posterolateral. Except for the anterior left hemiblock, which is seen more frequently in pediatrics, and can settle in healthy hearts, the other two presentations are infrequent and generally suggestive of organicity, due to intrinsic degeneration of the conduction system or a disease of the myocardium of the left ventricle [15].
Complete left bundle branch block (CLBBB): The interruption of the impulse from the AV node to the left branch of the bundle of His can occur before the subdivision or in both of its fascicles, therefore, the depolarization of the entire left ventricle is affected.
It has a strong association with underlying cardiovascular disease, sometimes it presents as the first manifestation of an unknown disease. Therefore, given its finding on the ECG, even in asymptomatic patients, a complete cardiological evaluation is indicated [16].
The main associated left bundle branch block heart diseases are:
- Left ventricular hypertrophy secondary to high blood pressure or aortic stenosis.
- Ischemic heart disease.
- Valvular disease: Aortic stenosis, mitral stenosis, aortic regurgitation.
- Dilated and hypertrophic cardiomyopathy.
- Degenerative disease of the conduction system (older patients).
- May appear with elevated heart rates due to aberrant conduction.
In Table 3 and in Figure 4 we list the electrocardiographic findings that define a LBBB along with a characteristic tracing, respectively [4].
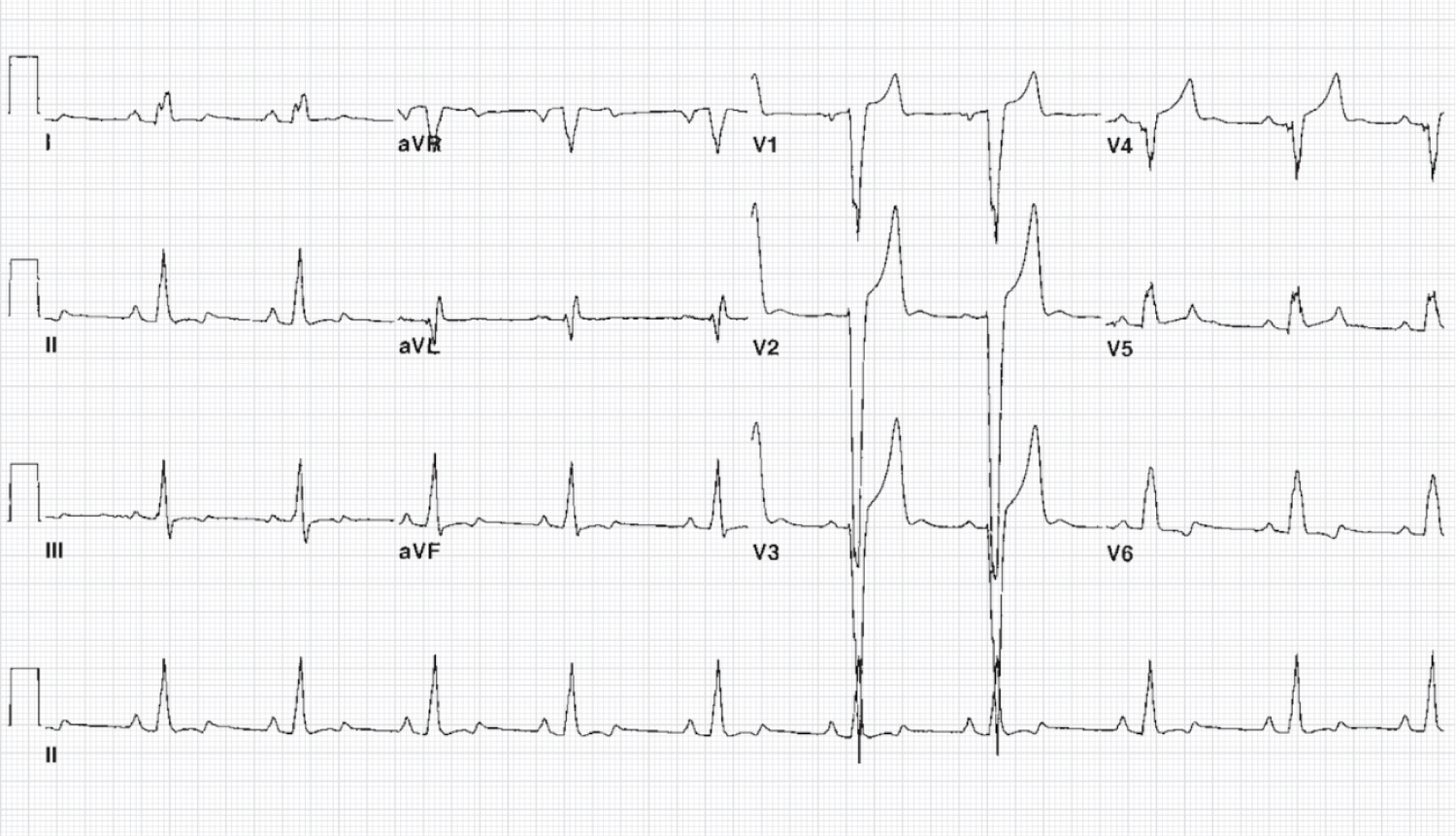 Figure 4: ECG with complete left bundle branch block.
View Figure 4
Figure 4: ECG with complete left bundle branch block.
View Figure 4
Table 3: Diagnostic criteria for complete left bundle branch block. View Table 3
Patients with isolated LBBB do not require specific treatment except for the underlying pathology, if any.
In sports context, contrary to RBBB, a LBBB in an athlete besides being more unusual does not seem to be related to normal physiology. LBBB is most likely representative of structural cardiac disease, it is considered a marker of future cardiovascular morbidity and mortality, so it should be specifically evaluated [16].
Left anterior fascicle block: Isolated left anterior hemiblock may be a common finding in patients with underlying congenital heart disease such as the spectrum of endocardial pad abnormality or triscuspid atresia. Although finding it in subjects without evidence of underlying pathology is the most frequent. After RBBB, it is the second most frequent electrocardiographic entity in pediatric age [8,17]. After a first specialized evaluation, in asymptomatic patients with this electrocardiographic finding, no follow-up is required, since it can be considered a variant of normality.
In Table 4 we can find the criteria that define the blockade of the left anterior fascicle in the ECG, in Figure 5 a characteristic tracing is shown [4].
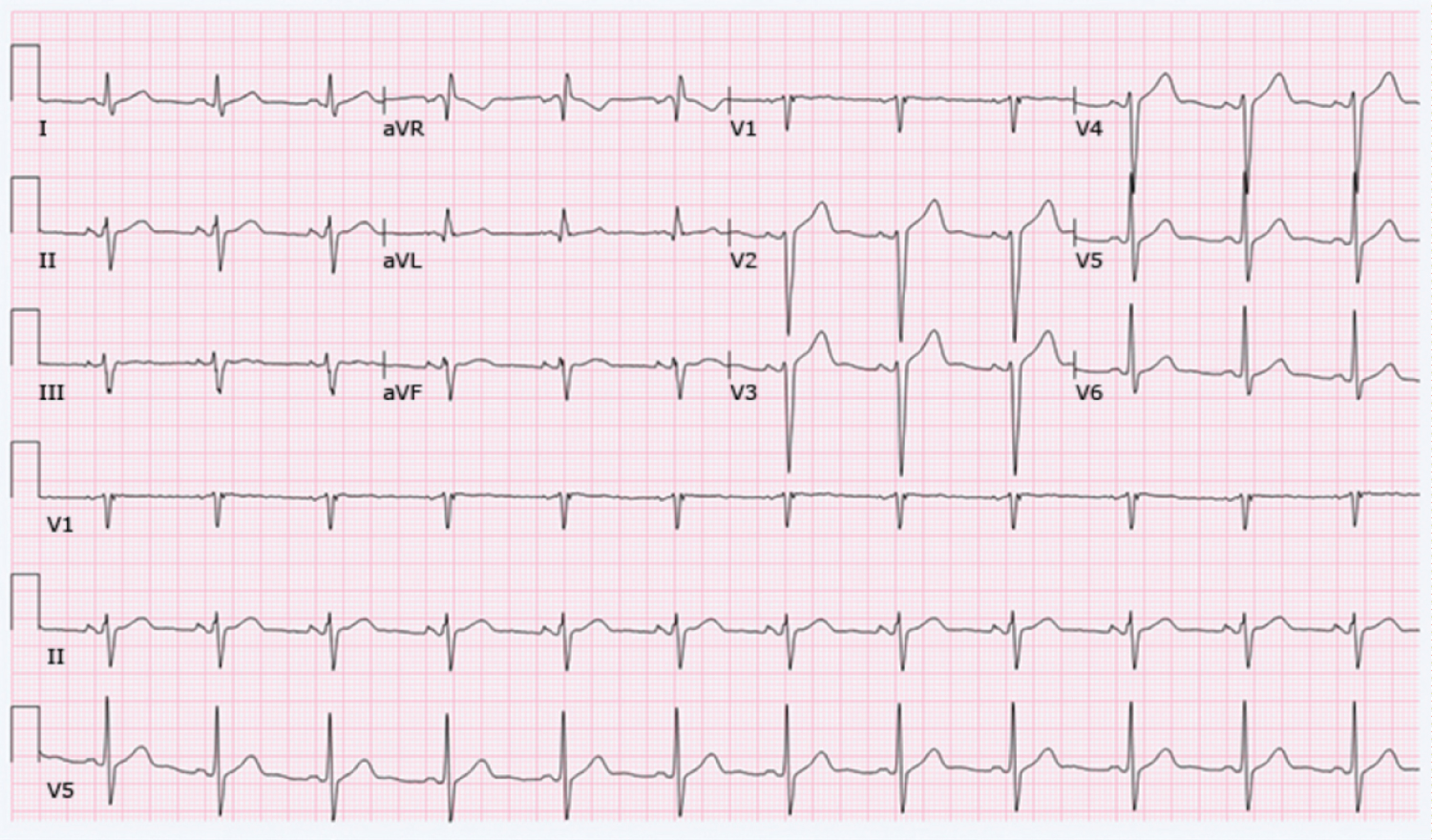 Figure 5: ECG with left anterior fascicle hemiblock.
View Figure 5
Figure 5: ECG with left anterior fascicle hemiblock.
View Figure 5
Table 4: Diagnostic criteria for left anterior bundle block. View Table 4
Block of the right posterior fascicle: Compared to the previous case, isolated left posterior hemiblock is organic and very rare in children. Its prognostic importance is unknown [17,18].
The typical ECG findings are attached below (Table 5 and Figure 6) [4].
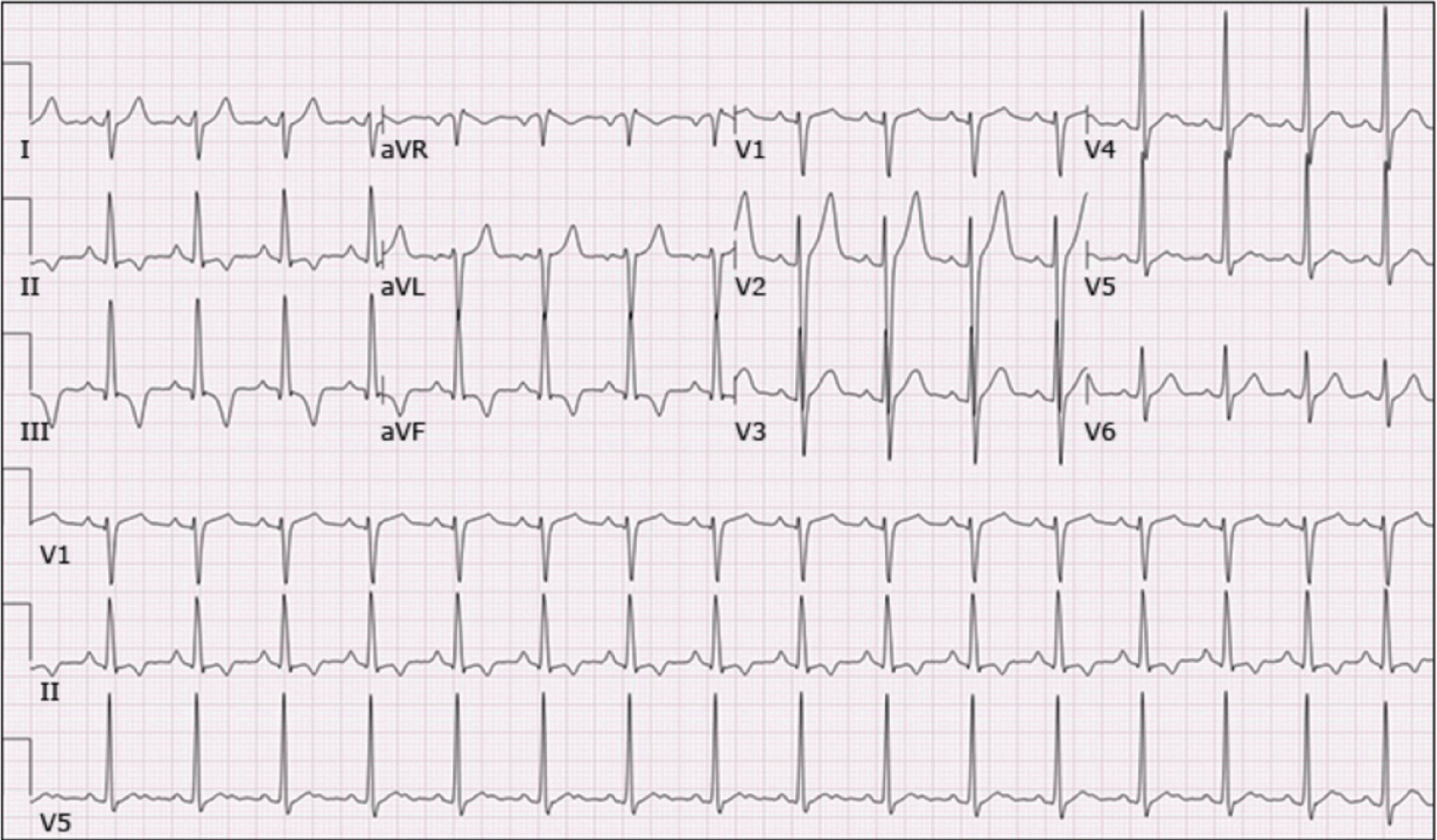 Figure 6: ECG with hemiblock of the right posterior fascicle.
View Figure 6
Figure 6: ECG with hemiblock of the right posterior fascicle.
View Figure 6
Table 5: Diagnostic criteria for right posterior fascicle block. View Table 5
In summary, we can conclude that bundle branch blocks are due to a delay in the conduction of electrical impulses through the intraventricular conduction system. They have typical electrocardiographic characteristics that make them recognizable. With relatively frequent forms in its presentation in pediatric age, such as incomplete right bundle branch block, and except the complete form, in addition to left anterior hemiblock, which may not be associated with cardiac pathology, the presence of this being more frequent in less common cases which requires an additional specialized assessment.
The authors have nothing to disclose.
These authors contributed equally to this paper.