The athlete's heart refers to a heart which has gained physiological adaptation mechanisms due to long term training in various sport activities. Sinus bradycardia, sinus arrhythmia, first degree atrioventricular block and second degree mobitz type I AV blocks are most common electrocardiographic findings in athlete's heart. In our case we observed first degree atrioventricular block with pathological PR interval values second degree mobitz type I (Wenckebach) atrioventricular block and accelerated junctional rhythm at the day time in a 13-year-old athlete playing football, exercising 21 hours a week. The clinical course of our patient indicates that such intense exercise may not always be beneficial to cardiovascular system in children.
Athlete's heart, Accelerated junctional rhythm, Electrocardiography, Atrioventricular block
The athlete's heart refers to a heart which has gained physiological adaptation mechanisms with electrical, functional and morphological remodeling, due to long term training in various sport activities [1]. These adaptive mechanisms may differ from benign changes, requiring no further evaluation, to life threatening arrhythmias on atrial, nodal and ventricular levels [2,3]. Variable degrees of atrioventricular (AV) conduction defects are commonly found in athletes; first degree AV block (35%) and Mobitz Type I (Wenkebach) second degree AV block (10%) are the most common two defects, respectively. These findings were also confirmed in pediatric patients > 14-years-old [4]. These findings are observed during resting and the disappearance of the findings during hyperventilation and exercise implies their physiological origins [5]. In some cases, AV junction can overtake the sinus node and produce rapid signals; therefore, causing a junctional tachycardia due to failure of synchronized atrial contraction [6]. Although the mechanism behind this is unclear, studies suggest that the accelerated junction rhythm is caused by an alteration of calcium metabolism in sarcoplasmic reticulum [7]. In order to differentiate physiological adaptation from changes indicative of underlying cardiac pathology ECG interpretation guidelines have been formed for the athlete's heart (Table 1) [8]. In this case study, we present an asymptomatic patient whose routine check-up showed accelerated junctional rhythm and Mobitz type I second degree AV block while resting in daytime.
Table 1: International Consensus Standards for Electrocardiographic Interpretation in Athletes. (adapted from Sharma, et al. [8]). View Table 1
A 13-years-old boy was admitted to our Pediatric Cardiology outpatient clinic due to sports license examination. He had multiple cardiac check-ups, no significant past cardiovascular history. His multiple previous ECGs were normal except for having physiological mitral regurgitation. His family history was negative for heart disease, sudden cardiac death and premature death. Henoted no cardiac symptoms such as chest pain, dyspnea, palpitation, faintness or syncope. He was an athlete playing football, exercising 21 hours a week. He was 160 cm in height and 48 kg in weight. His pulse rate was 83 bpm and the blood pressure were 112/60 mmHg. Cardiac auscultation showed S1-S2 positive with no murmurs or gallop, and pulmonary auscultation showed normal respiratory sounds and no rales. The first 12-lead resting ECG revealed first degree AV block with 520 ms PR interval (Figure 1). The control ECG from the same day, also had first degree AV block with 480 ms PR interval. Transthoracic echocardiography showed no significant pathology. Laboratory examination revealed no significant pathological change. The patient was hospitalized and NSAID 400 mg was prescribed 4 times daily. Basal ECG of the patient remained first degree AV block during first 3 days of his stay in hospital. Following the third day, mobitz type 1 (Wenckebach) second degree AV block rhythm was observed at his awaken ECG early in the morning (Figure 2). 24 hours ambulatory ECG recording (cardiolineclickholter HRV package system, version 1.4.1 Biomedical Systems, Italy) showed accelerated junctional rhythm at daytime (Figure 3). At the 5th day of stay, rhythm became normal sinus. The patient was discharged after performing treadmill stress test with Bruce protocol. The Treadmill test exceeded 97 percentiles and the ECG was normal sinus rhythm. Blood pressure responses and hearth rate remained normal, no arrhythmia and ST-T changes were observed. The patient's follow up continues without any complications.
 Figure 1: First degree atrioventricular block (PR interval: 520 ms). View Figure 1
Figure 1: First degree atrioventricular block (PR interval: 520 ms). View Figure 1
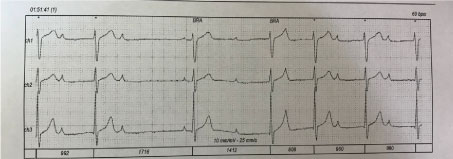 Figure 2: Second degree Mobitz type 1 (Wenckebach) atrioventricular block. View Figure 2
Figure 2: Second degree Mobitz type 1 (Wenckebach) atrioventricular block. View Figure 2
 Figure 3: Accelerated junctional rhythm. View Figure 3
Figure 3: Accelerated junctional rhythm. View Figure 3
Athlete's heart may demonstrate changes in ECG findings, due to adaptive mechanism gained by ≥ 3 hours/week exercise. Most common of these changes are; sinus bradycardia, sinus arrhythmia, first degree AV block and Mobitz type I second degree AV block.
Long PR interval is a physiological change for Athlete's heart but the ECG results of our patient, who had a heavy exercise habit of 21 hours/week, showed first degree AV block with a persistent pathological PR interval of > 400 ms [8] for 3 days with a co-existence of junctional rhythm. Additionally, our patient developed Mobitz type I second degree AV block during his hospitalization. Although in literature, it is indicated that Mobitz type I second degree AV block's incidence is higher at nights, our patient demonstrated this condition only at day time [1].
In study conducted on 2484 athletes, Huttin and colleagues observed first degree AV block (PR > 200 ms) in 8% of the sample, with increased PR interval over 240 ms in 2% and shortened PR interval under 120 ms in 2%. While they found no significant change in AV conduction (ß = -0.0004, 95% CI -1.53 to 1.53; not significant), we observed increased PR duration with AV conduction defect in our patient [9].
Most sports activities and regular exercise are presumed to be good for health. Nevertheless, in accordance with the previous publications, the clinical course of our patient indicates that such intense exercise of 21 hours/week may not always be beneficial to cardiovascular system in children [10].