Objective: To update the current evidence of the effect of acupuncture on recovery Heart Rate (HR), blood lactate and maximum volume of oxygen consumption (VO2 max) following intense exercise through a systematic review of published randomised controlled trials.
Methods: A systematic literature search was performed on electronic databases from inception to 2020. The Cochrane Handbook guidelines for Systematic Reviews of Interventions were used to assess the methodological quality and exclude studies with fatal flaws. The risk of bias was assessed using the Cochrane grading system by two reviewers (SB and BL). Acupuncture intervention was assessed using the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA). This review is reported according to the PRISMA guidelines.
Results: A total of 16 RCTs were included in this review. 8 of the 10 studies that assessed the effect of acupuncture on HR recovery found acupuncture to be significantly more effective than no treatment or sham acupuncture at enhancing recovery HR following exercise. 7 of the 10 studies that assessed the effect of acupuncture on reducing blood lactate found that acupuncture was significantly more effective than no treatment or sham acupuncture at reducing blood lactate following exercise. 4 of the 7 studies that assessed the effect of acupuncture on VO2 max found that there was no significant difference between groups with regards to VO2 max.
Conclusion: Our results indicate that there is strong evidence that acupuncture is significantly more effective than sham and control in enhancing recovery HR and blood lactate following intense exercise. However, there is conflicting evidence with regards to the effect of acupuncture on enhancing VO2 max in athletes. Future studies are required that follow the STRICTA guidelines to help determine the effect of acupuncture on enhancing VO2 max in athletes.
Acupuncture, Heart rate, Blood lactate, VO2 max, Exercise, Recovery
Developing effective methods to help athletes quickly recover from intense exercise or fierce competition and to help them achieve the best psychological and physiological condition is deemed essential, especially prior to international competitions [1]. Cardiovascular fitness represents the efficiency of the heart, lungs and vascular system in delivering oxygen to the working muscles so that prolonged physical work can be maintained. Improvement in cardiovascular fitness is integral to many sports and gives individual athletes and teams a competitive edge over their rivals. Conventionally, cardiovascular fitness is assessed by variables such as resting Heart Rate (HR), HR recovery, resting Blood Pressure (BP), cardiac output, Stroke Volume (SV), maximum volume of oxygen consumption (VO2 max), and endurance capacity [2]. Within the field of sports medicine, acupuncture interventions have been shown to enhance muscle strength [1,3-7], bone repair [8-11], and tendinopathy repair by boosting blood flow and oxygenation to tendons to enhance healing [12,13]. It has also been shown to improve joint proprioception [14]. Although the effects of acupuncture in the management of musculoskeletal injuries have been demonstrated by a number of Randomised Controlled Trials (RCTs), the effects of acupuncture on the physiological response to intense exercise are still unclear.
Our previous review [1] found that there is strong evidence in support of the use of acupuncture with regards to enhancing HR recovery following intense exercise [15-18]. However, there was conflicting evidence to support the use of acupuncture to enhance removal of blood lactate [7,16,19] and to enhance VO2 max [15-17] post-exercise. The majority of the RCTs in our previous review scored low formethodological quality and the quality of the acupuncture interventionwas poor. A systematic review by Urroz, et al., [20] investigating the effect of acupuncture treatment on exercise performance and post-exercise recovery presented with findings similar to our previous study. Therefore, the aim of this review was to update the current evidence with regards to the effect of acupuncture on recovery HR, blood lactate and VO2 max following intense exercise.
This review is reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [21].
A systematic literature search was performed by SB and BL on the following databases from their inception to 2020: MEDLINE, Embase, SPORTDiscus, CINAHL, AMED, ProQuest nursing journal, PubMed, ScienceDirect, the Cochrane Central Register of Controlled Trials, PEDro, Google Scholar, specialized registry of the Cochrane Musculoskeletal group and the Cochrane field of Physical and Related Therapies. The key word search included: acupuncture, auricular acupuncture, laser acupuncture, TENS, electro-acupuncture, acupressure, or acupoint. These were combined with: heart rate, lactate, VO2 max, oxygen consumption, performance, exercise, aerobic, activity, sports, training, endurance, recovery. The bibliographies and references of published studies and reviews were scanned for other possible RCTs. The reviewers (SB and BL) determined the studies to be included based upon the inclusion and exclusion criteria.
To be included in this review, a study had to meet the following criteria: RCTs that had used acupuncture to enhance recovery HR, VO2 max and the reduction of blood lactate following intense exercise. No language restrictions were imposed, and translations were sought where necessary. Only published RCTs, in English or translated into English, were included.
The guidelines of the Cochrane Handbook for Systematic Reviews of Interventions [22] were used to assess the methodological quality and to exclude studies with fatal flaws. The risk of bias was assessed using the Cochrane grading system in the Rev Man 5.4 software by two reviewers (SB and BL) to evaluate: (a) Sequence generation, (b) Allocation concealment, (c) Blinding of participants and therapists, (d) Blinding of outcome assessor, (e) Incomplete outcome data, and (f) Selective outcome reporting. After evaluation of each domain, the studies were classified as low, unclear, or high risk of bias. Acupuncture intervention was assessed using the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) [23].
Figure 1 shows the PRISMA flow diagram outlining the selection of the included studies. A total of 9067studies were located; 9042 were excluded because they were duplicates, compared the effect of acupuncture on heart rate variability in unhealthy populations, did not involve acupuncture, were systematic reviews or single case studies, were in German or Chinese and could not be obtained in English, or they did not include a control group. Thirtyfull text studies were identified in whichone did not include exercise, and13 were not an RCT or were a protocol or unpublished studyand were therefore removed. Sixteen RCTs were finally included in the systematic review.
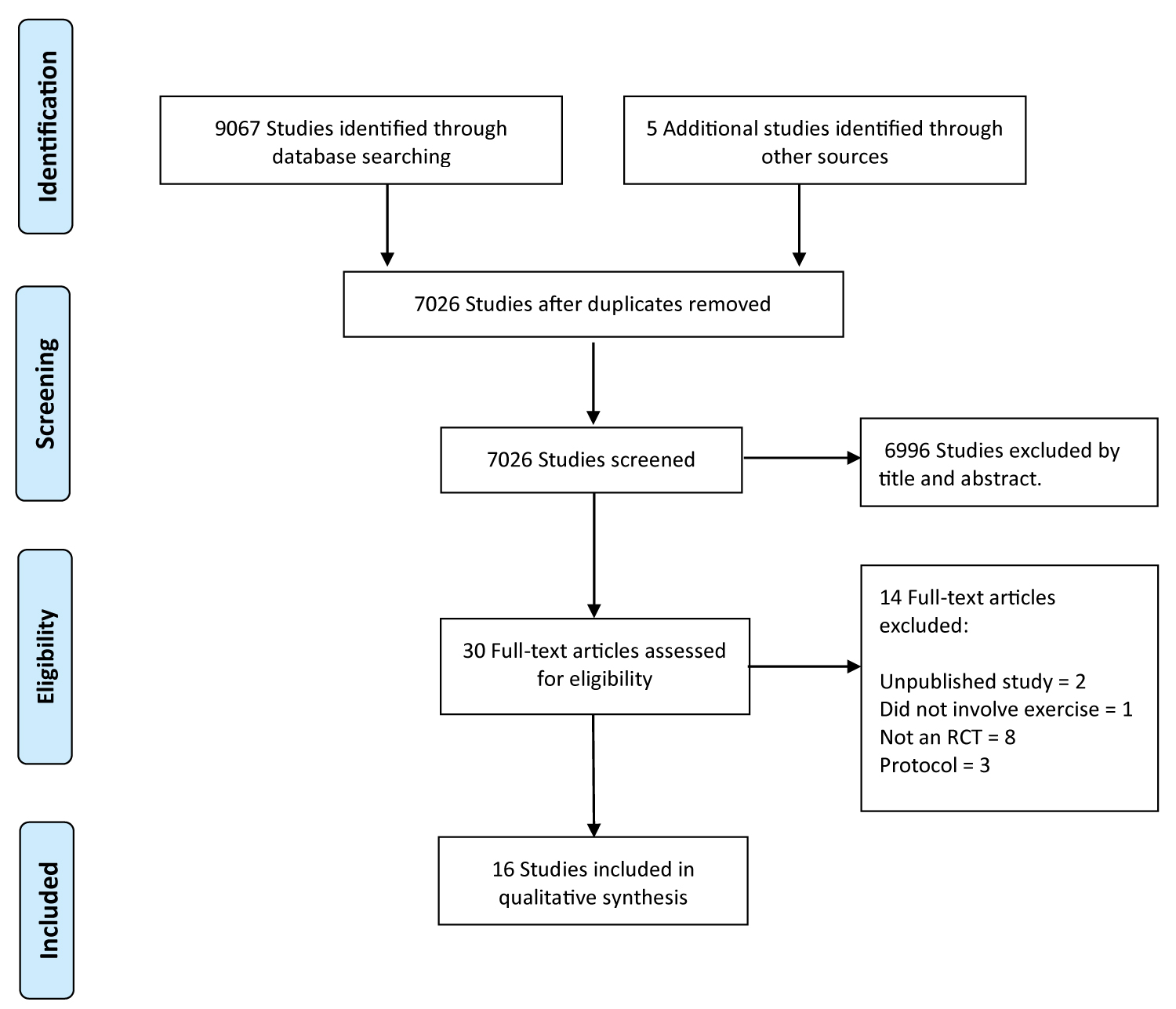 Figure 1: Flow diagram of study selection. View Figure 1
Figure 1: Flow diagram of study selection. View Figure 1
The characteristics of each study are presented in Table 1. The studies reviewed were published between 1992 and 2018 and included 409 participants aged between 16 and 60-years-old (mean age 24.5 yrs). The sample size was generally small and ranged from 10 to 60 participants in each study. Ten (62.5%) studies [7,18,19,24-30] had fewer than 30 participants. Thirteen (81.25%) studies [7,16,18-20,24-29,31,32], only applied one treatment session while three (18.75%) studies [15,17,30] applied several treatments over 4-5 weeks. Nine (56.25%) studies [16,18,19,24-26,28,31,32] applied treatment before exercise intervention, three (18.75%) studies [7,20,29] applied treatment after exercise and one study [27] did not mention when acupuncture was applied. There were at least 45 female and 296 male participants reported to take part in the trials. One study did not report on gender [32] and another study [15] did not indicate the ratio of female to male participants. Seven (43.75%) studies [16,19,25,29-32] used elite athletes and nine (56.25%) studies [7,15,17,18,20,24,26-28] used active healthy subjects. One study [25] used auricular acupuncture and compared with control, four studies [7,18,26,28] compared the effects of Acu-TENS with placebo Acu-TENS, one study [27] evaluated the effect of acupressure compared to exercise recovery. Seven studies [15-17,20,24,29,32] investigated the effect of acupuncture compare with control andshamand one study [31] used magnetic studs in the ear.
Table 1: Characteristics of studies. View Table 1
Figure 2 presents the percentage of the risk of bias across all the included RCTs. The risk of bias across all RCTs is summarised in Figure 3. Generally, there was poor reporting with regards to method of randomisation and allocation of participants to treatment groups. Nine studies (56.25%) were rated as unclear (?) for sequence generation and 4 studies (25%) rated as low risk of bias (+). The majority of studies gave an unclear description or did not discuss the method of allocation (9 studies, 56%) and concealment (10 studies, 62.5%). There was a high risk of bias (-) with regards to blinding of participants and personnel (6 studies, 37%) and blinding of outcome assessors (8 studies, 50%); otherwise the studies were unclear in their explanation of blinding of participants and personnel (6 studies, 37%) and blinding of outcome assessors (7 studies, 43%). The majority of studies rated low for incomplete outcome data (14 studies, 87.5%), selective reporting (13 studies, 81.25%) and other bias (11 studies, 68.75%).
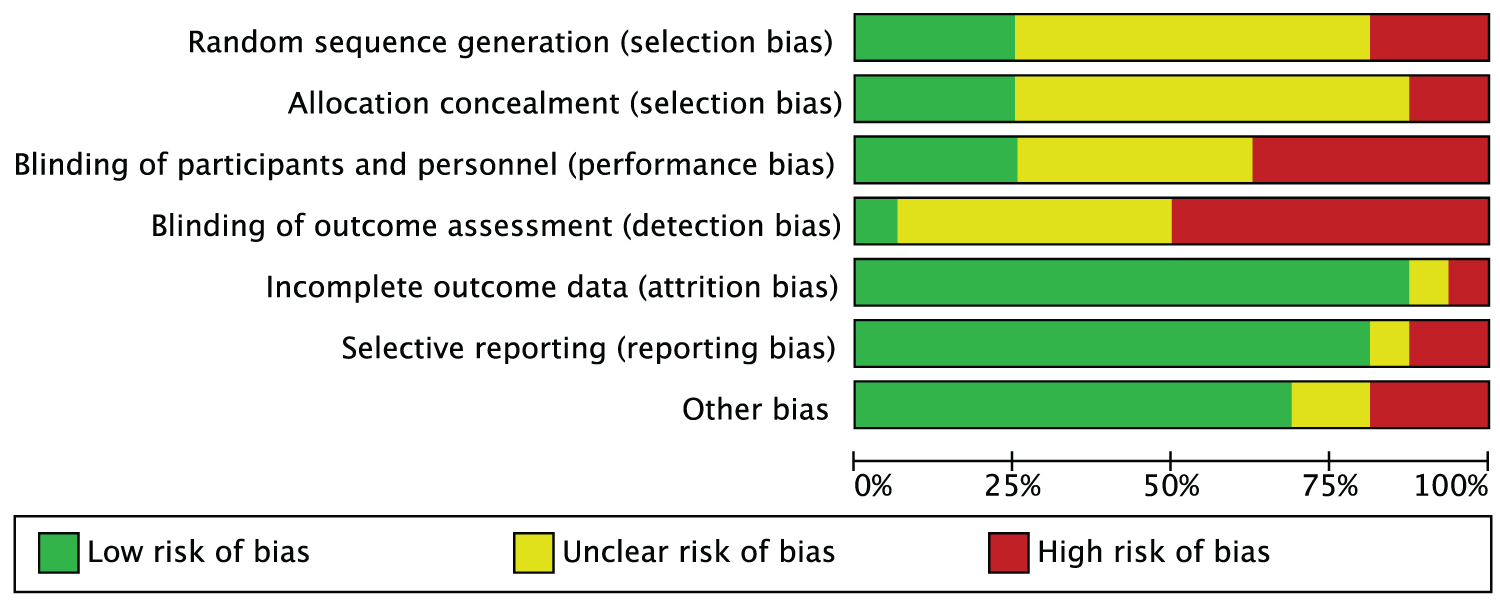 Figure 2: Graph to show percentages of risk of bias across all studies. View Figure 2
Figure 2: Graph to show percentages of risk of bias across all studies. View Figure 2
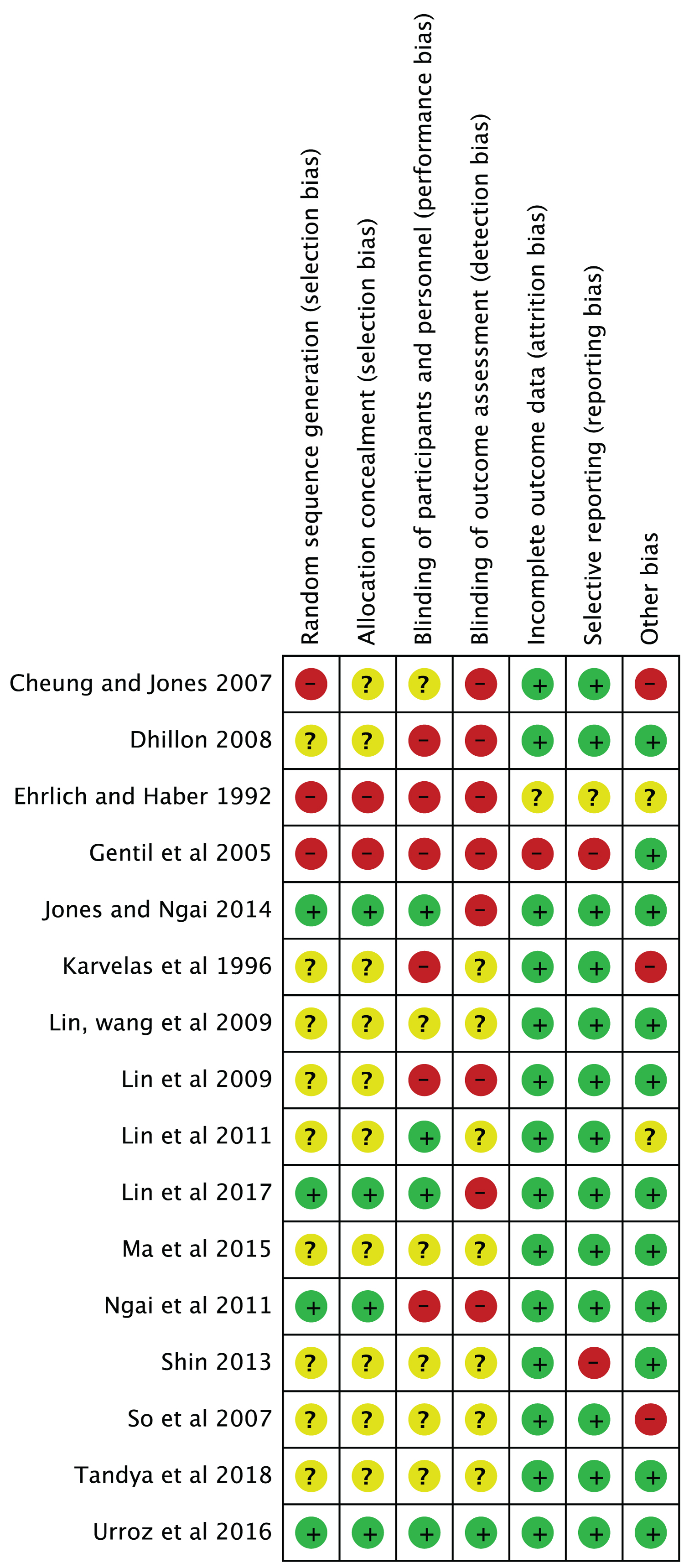 Figure 3: Risk of bias summary. View Figure 3
Figure 3: Risk of bias summary. View Figure 3
None of the RCTs assessed in this review used the STRICTA checklist as a guide. However, most of the recommendations on the checklist were fulfilled by the majority of the RCTs. When assessing the effects of acupuncture on specified conditions it is important to select the most appropriate acupuncture points that have been shown to be most relevant to the condition or organ function under investigation in order to acquire optimal results. The experience, knowledge and training of the acupuncturist who is applying the treatment can have a profound impact on the precise location of the acupuncture points, choice of points, and treatment outcome [1]. What was most consistent in the majority of RCTs in this review was a lack of reporting on the qualification and experience of the practitioner administering acupuncture and other components of the acupuncture treatment. The method of needle stimulation was inadequately discussed, and, in some studies, it was not mentioned [15-17,27,29].
Delayed effect of acupuncture: The time from the treatment to the assessment of the effects of acupuncture varied considerably between studies, which would have an impact on the treatment outcome. Both human and animal studies have shown that the effects of acupuncture have a delayed onset, with a gradual peak, and a gradual return to baseline [33-35]. Price and colleagues [33] found that following electro-acupuncture, there is a delayed onset of between 1 and 24 hours to maximum effect. Our earlier review [1] found that acupuncture was significantly more effective than sham acupuncture and the control group when assessed up to 72 hours after treatment and not as effective when assessed immediately following treatment. Furthermore, it was found that acupuncture was most effective when several sessions over a number of weeks were employed [1]. The majority of studies in this review used a single treatment session with a crossover design. It is suggested that crossover design studies comparing real versus sham acupuncture raises doubt as to whether participants can maintain blindness to acupuncture treatment once they have been exposed to both real and sham acupuncture interventions [1]. Therefore, it may be more beneficial to use parallel rather than crossover designs to assess the effects of acupuncture in future trials [36]. Furthermore, carry-over treatment effects which persist long after treatment ceases have been documented in crossover trials of acupuncture [37].
A meta-analysis was not possible due to the incomparability of the study characteristics such as outcome measures, treatment intervention, patient population and the methodological rigour.
Ten studies [14-17,19,23-25,29] evaluated the effect of acupuncture on recovery HR. Eight studies [14-17,19,24,29] found acupuncture to be significantly more effective thanno treatment or sham acupuncture at enhancing recovery HR following exercise. Recovery HR was reported to be 4 to 10 minutes quicker in the acupuncture group compared to the control and sham acupuncture group following exercise [18,28]. Two studies [23,25] found that there was no significant difference between treatment intervention in recovery HR post-exercise. The overall findings indicate that there is strong evidence that acupuncture is significantly more effective than no treatment or sham acupuncture in enhancing recovery heart rate following exercise.
Seven studies assessed the effect of acupuncture on VO2 max. Three studies [16,25,31] found that acupuncture was significantly moreeffective than no treatment and shamacupuncture in enhancing VO2 max. Four studies [15,17,24,28] found that there was no significant difference between groups with regards to VO2 max.
A total of 10 studies [7,16,17,19,20,25,27-29,32] investigated the effect of acupuncture on blood lactate levels. Seven studies [7,16,25,27-29,32] found that acupuncture was significantly more effective than no treatment or sham acupuncture at reducing blood lactate following exercise. Three studies [17,19,20] found no significant difference between groups. The overall findings indicate that there is strong evidence that acupuncture is significantly more effective than no treatment or sham acupuncture in enhancing lactate removal following exercise.
This review assessed the effect of acupuncture on reducing HR, blood lactate and VO2 max following exercise in healthy individuals. The study by Dhillon [19] looked for an increase in blood lactate during intense exercise unlike the other studies that were looking for a decrease in blood lactate following exercise. The findings from Dhillon [19] showed that the acupuncture intervention group presented with a higher (but not significant) lactate level, significantly higher Reported Perceive Exertion (RPE) and were able to work harder and longer. Although the acupuncture group completed the 20 km cycle one minute quicker than the sham and control group, statistically there was no significant (p < 0.66) difference in cycling time for the acupuncture (36.19 min), sham (37.03 min) and control (37.48 min) groups. In the real world, in a 20 km cycling race the ability of the acupuncture group to complete a race one minute quicker than their competitors would be more than a significant difference. The findings of Dhillon [19] aresimilar to Ngai, et al. [26] who reported that there was no significant difference between groups in RPE, but the acupuncture group was able to work harder and longer (1 minute) at near maximal intensity. Furthermore, Ma, et al. [29] announced that following acupuncture, the levels of distinguished metabolites, 2-hydroxybutyrate, 3-hydroxyisovalerate, lactate, pyruvate, citrate, dimethylglycine, choline, glycine, hippurate, and hypoxanthine were recovered at an accelerated speed in the acupuncture group in comparison with the control group. These findings indicate that acupuncture reduces fatigue and aids recovery following exercise by back regulating the disrupted energy metabolism, choline metabolism, and attenuating Reactive Oxygen Species (ROS) stress within the muscles. These findings are important for athletes who are competing at an elite level and are involved in multiple events over several days [1]. The quicker the removal of lactic acid, metabolitesand reduction of ROS stress following intense exercise, the better prepared the individual athlete will be for their next round of competition, allowing the muscles to work to their maximum for longer before they start to fatigue.
The mechanism by which acupuncture is suggested to achieve its effect on the cardiorespiratory system is partly through its effect on the Autonomic Nervous System (ANS). The activity of the Vagus Nerve (VN) is associated with health and wellbeing and constitutes the main part of the parasympathetic branch of the ANS. The VN comprises afferent and efferent fibres that control, among other things, respiration and HR [1]. Several reports from human studies support an increase in vagal activity and/or a decrease in sympathovagal balance during acupuncture on PC-6 [38-40]. A systematic review [41] evaluated the effect of acupuncture on HR variability and found a significant effect of ST-36 and PC-6 on low and high frequency ratio of HR variability compared to sham/control in healthy subjects. The most common acupuncture points used in this review were ST-36 (9 = 56.25%) and PC-6 (7 = 43%).
There were a number of limitations within this study. It was difficult to make comparisons with all the studies within this review due to the differences with regards to when treatment was applied (before, during or after exercise), treatment duration, when assessment was conducted (during exercise, immediately after, or intervals following exercise), number of treatment sessions, different outcome measure tools and diverse choice of acupuncture points between studies. Some studies did not present all of the qualitative data (mean and standard deviation). The lack of consistency in the reporting makes it difficult to draw an exact conclusion on treatment dose.
Our results indicate that there is strong evidence that acupuncture is significantly more effective than sham and control in enhancing recovery HR, and blood lactate following intense exercise. However, there is conflicting evidence with regards to the effect of acupuncture on enhancing VO2 max in athletes. Further studies are required that follow the STRICTA guidelines to help determine the effect of acupuncture on enhancing VO2 max in athletes.
S.B developed the research question and search strategy. Both S.B and B.L collected and managed the data. Writing of the original draft was by S.B. All authors have read and agreed to the article before submission.
The authors declare that they have no conflict of interest and the author has no financial interest related to the material of this manuscript.
No funding was received.