Background: Obesity is a serious risk for various cardiovascular diseases and is often managed with increased physical activity and exercise. The purpose of this study is to investigate the effects of a minimal dose, High-Intensity Circuit Training (HICT) program on a range of cardiovascular risk factors in obese and overweight individuals.
Methods: The trial was prospectively registered with Cyprus National Bioethics Committee ΕΕΒΚ/ΕΠ/2017/38 29 th October 2017. A total of 30 participants were randomly allocated to HICT-group (n = 15) or to a no exercise control-group (n = 15). Participants in the HICT-group trained for 36-minutes, twice a week (18-minutes per session) for 8 weeks in total. The program consisted of 2 circuits of 6 exercise stations of 1min at 50-60% of Heart Rate Reserve (HRR) which progressed to 70-85% of HRR after the first two weeks, alternating with 1min active rest at 40-50% of HRR which progressed to 50-60% of HRR. Approximately 12 repetitions were performed per station. Body composition, blood markers and physiological variables, cardiorespiratory fitness and isometric strength were measured at baseline and post-intervention.
Findings: Significant and meaningful improvements were demonstrated in cardiorespiratory fitness, several body composition variables, isometric strength of the left (non-dominant) lower limb and several physiological variables. No significant changes were revealed to the biochemical parameters or the strength of the right (dominant) limp.
Conclusion: The results of the study suggest that a low-frequency, circuit training program with high intensity lasting only for 18-minutes twice a week is the minimum required dose in reducing at least some of the cardiovascular risk factors, in obese and overweight population.
Circuit training, Cardiovascular health, Risk factors, Obese, Overweight, High-intensity training
Excessive weight gain and obesity are a global public health problem, associated with an increase of several cardiovascular risk factors [1] and the prevalence of non-communicable diseases such as metabolic diseases [2], certain types of cancer [3], depression [4,5], sleep disturbances [5,6] and all-cause mortality [7,8]. Strategies to decrease the cardiovascular risk factors, to reduce the incidence of these diseases and improve their physical, social and psychological consequences that affect the quality of life is a perpetual goal of health providers [9,10].
American College of Sports Medicine (ACSM), suggestsa combination of Moderate Intensity, Aerobic, Continuous Exercise (MICT) and resistance training whenever possible, for the management of obesity [11]. Despite the physical activity recommendations (at least 150 min of moderate intensity exercise or 75 min of vigorous intensity exercise per week) [12], lack of adequate physical activity remains a worldwide problem [13]. It was reported in the 2016 Lancet Series of physical activity that the prevalence of inactivity was 23.3% and that women and older individuals have higher levels of inactivity [13,14]. Exercise training involving aerobic and resistance exercise, have been used to increase energy expenditure and demonstrated a positive impact in body composition of normal-weight and obese individuals [9,15,16]. However, lack of time and motivation, financial reasons, fatigue and family responsibilities are often cited as barriers to participation in these exercise programs [10,17].
Training programs for weight control, vary on exercise modalities, intensity, duration and frequency. The vast majority of the studies for the management of obesity used MICT [18]. The last few years High Intensity Interval Training (HIIT) has received extensive attention as a an effective and time-saving exercise modality for overall health [19,20]. A large number of studies compared HIIT to MICT and demonstrated that HIIT has similar effects in health parameters such as body composition, physiological parameters, cardiorespiratory fitness [20-24].
Traditional HIIT protocols used in obese and overweight individuals, utilise unimodal, aerobic exercise regimens on cycle-ergometers or treadmills [20,25-27] and are often criticised as inadequate to improve Lean Body Mass (LBM) [28] and to advance functional performance [29]. In contrast, resistance training is known to induce muscle hypertrophy and increase muscle strength [28] and is included in the exercise recommendations (moderate to vigorous strength training ≥ 2 days/week in addition to aerobic exercise) of public health [12]. Therefore, combining strengthening and aerobic exercises in a high intensity program, seems ideal for weight control as it includes beneficial adaptations from both types of exercises [12] and reduces the time needed for meaningful results, which is an important barrier to participation for some people [17].
One example of successful combination of aerobic and resistance exercise is Circuit Training (CT) which includes multi-joint resistance exercises and calisthenics in a high intensity program [30]. During CT, participant moves from one exercise station to the next, with limited rest, which results in a short duration of each session [31]. Moreover, this program can be adjusted to any baseline level of fitness and includes functional movements and body weight exercises [27]. Furthermore, it does not need any expensive equipment, it can be performed everywhere and can be progressed as the fitness improves. New and inexpensive technologies such as Heart Rate (HR) monitors which are easily accessible could help monitor the intensity of exercise, the HR, the fitness level, the aerobic or anaerobic stress of the exercise as well as the quality of sleep, the activity level and the daily energy expenditure [32]. Overall CT can overcome several of the berries to participation in exercise such as financial constraints, lack of specialised equipment or space, time constrictions and therefore increase the adherence in the regimen.
Only a few studies have looked at the effects of CT. Three of these studies examined only middle age participants. Ballesta-García, et al. [33] reported that 1-hour of HICT (14–18 Borg scale) twice a week for 18-weeks, is more effective than MICT in improving upper limb strength and reducing Body Mass Index (BMI) in middle-aged and older women. The same study reported significant improvements in maximum oxygen uptake, Systolic Blood Pressure (SBP) and Diastolic Blood Pressure (DBP) after the program, compared to the no-exercise group [33].Two studies by the same group using the same HICT protocol (3times for 50 minutes/week for 12 weeks) showed significant improvement in DBP and blood lipid profile compared to low intensity CT and endurance training [30] and that HICT can augment the improvements of endurance training in body composition, blood lactate and strength [34].
Only three studies looked at the effect of HICT in overweight or obese individuals and two of them included only women while the third included only men. Sperlich, et al. compared HICT alone or in combination with high volume low intensity training in overweight women and concluded that both regimens were effective in improving body composition, fitness, physical performance and several other variables [35]. Interestingly, they found that while HICT improves peak oxygen uptake it causes a higher perception of pain and that the combined protocol is better at improving the perception of general health [35]. Another study in obese women which lasted for 40-weeks, used CT for 3 times per week with 10-12 exercises (65% of HRR) [36]. These exercises were performed with work and recovery intervals (20-40 sec) and participants completed as many repetitions as possible at each station. Following the completion of the study, the participants had on average a 6% reduction in BW and a 5.5% in BF with a 3.4% increase in LBM and an increase in strength and endurance by almost one third [36]. Miller, et al, demonstrated significant improvements in biochemical, physical and body composition characteristics of sedentary obese males with only 6 hours of HICT in four weeks (30min x3/week) [31].
All these studies examining the efficacy of HICT used a long duration of exercise for several weeks with the exception of Miller, et al. which used shorter sessions (30 minutes) for only four weeks. The minimal dose (duration/frequency) of HICT which is able to offer meaningful improvements in obese and overweight men and women is yet to be determined.
The purpose of this study was to examine the effect of an 8-week, multi-modal HICT program that includes short sessions of resistance and aerobic exercises in obese and overweight individuals. The hypothesis of the study was that an 8-week HICT program will be able to induce changes in body composition, lipid profile, strength of lower limbs, physiological and cardiorespiratory parameters of obese and overweight individuals with only two short duration session per week.
A total of 30 individuals between the age of 18 and 55 years were recruited from Nicosia district of Cyprus via flyers and advertisements at the local noticeboards. Eligible participants were screened by the following criteria: (a) BMI ≥ 25 kg/m2, (b) no history or presence of endocrine, pulmonary and cardiovascular disease, (c) no history of musculoskeletal condition that would contraindicate the participation to exercise. Participants were excluded if: (a) they had a record of regular physical activity over the past 6-months, (b) had any symptom related to cardiovascular and pulmonary diseases, (c) had a "yes" answer in any question of the Physical Activity Readiness Questionnaire (PAR-Q). All participants provided informed written consent prior to participation, and the study was approved by the Cyprus Bioethics Committee (ΕΕΒΚ/ΕΠ/2017/38). Potential participants were assessed based on inclusion and exclusion criteria during initial contact and screened again by a cardiologist before conducting the initial assessment. All measurements (except biochemical analysis) were performed (from June 2017 to January 2018) at the physiotherapy laboratory of University of Nicosia. Participants demographic characteristics are provided in Table 1.
Table 1: Baseline characteristics of the two groups. View Table 1
Participants were randomly assigned to one of two groups: (1) HICT (n = 15) or (2) Control-group (n = 15), using established randomization software (Sealed Envelope.com, Clerkenwell Workshops), after the initial assessment by one of the assessors. This was a randomised, clinical trial with HICT as the intervention group and Control-group as the comparator group. Participants assigned to HICT-group participated twice a week in a supervised, progressive exercise program for 8-weeks, whereas those in control-group continued their usual routine. All participants were asked to continue their normal diet and physical activity routine. It was not possible to blind participants, as they usually are aware whether they are training or not [37]. However, the assessors who perform the biochemical analysis and the 6-minute walking test were blind.
The assessment was conducted at week 0 prior to the intervention and at week 8 within 2 days after the completion of the program. The assessment sessions were conducted in the morning, between 8:00-9:00 am. Participants were required to abstain from food, alcohol and caffeine consumption after midnight of the night prior to the assessment and any strenuous exercise the day before the assessment. On both occasions, anthropometric, body composition, physiological parameters, biochemical markers, cardiorespiratory fitness and strength measurements were performed within 2 days. A follow-up assessment after 2-months was also conducted, at a similar time of the day which included only the cardiorespiratory fitness testing as described below.
The assessments were carried out with the same minimum clothing, without socks and shoes. Height was measured using a portable standing stadiometer (Seca, Hamburg, Germany). Body composition including body mass in kilos (BM-Kg), Lean Body Mass in kilos (LBM-Kg), percent Lean Body Mass (LBM%), body fat in kilos (BF-Kg), percent Body Fat (%BF) and BMI was obtained with an electronic scale, calibrated prior to each day of testing (Omron BF511, Kyoto, Japan). Waist Circumference (WC) was measured in the horizontal plane midway between the lowest rib and the top of the iliac crest and hip circumference was assessed at the level of the symphysis with a measuring tape. Waist-to-Hip Ratio (WHR) was calculated based on the WHR= waist circumference / hip circumference equation [38].
A 12-hour fasted venous blood sample was obtained from the antecubital vein in sitting position by a trained biochemist. Samples were collected in an EDTA tube and blood was centrifuged for 10 min at 1000×g to separate plasma. Plasma Total Cholesterol (TC), triglycerides, High-Density Lipoprotein Cholesterol (HDL), Low-Density Lipoprotein Cholesterol (LDL) concentrations and fasting glucose levels were analysed by Lx20 (Beckman Coulter LX20, Fullerton, CA, USA).
Resting Heart Rate (RHR) and Blood Pressure (BP) were assessed in a sitting position after participants maintained a quiet position for at least 10-minutes. An automatic BP monitor (Omron M3, Kyoto, Japan) was used to assess SBP and DBP. BP assessment was performed 3 times with 1-minute interval and the average was used in the analysis. RHR was recorder via a pulse meter watch (Polar V800, Finland), while participants were in a seated resting position for 10-minutes.
Exercise intensity was set as a percentage of maximum HR. Maximum HR (HRmax) was predicted from the 208- (0.7 x age) equation [39]. The intensity of the exercise was then set using the formula (Exercise HR = [(HRmax/peak − HRrest) × % intensity desired] + HRrest) [38].
The following equations: (a) RPP = HR Χ SBP and (b) MAP = [(DBP Χ 2) + SBP]/3 were used to calculate Rate Pressure Product (RPP) and resting mean arterial pressure (MAP) [40-42].
Cardiorespiratory fitness was assessed by the 6-Minute Walking Test (6MWT) pre-intervention (week 0), post-intervention (week 8) and at the follow-up (2 months). The walking test was performed on a flat 30-metre-long indoor walking track, marked with visible cones and following the standards established by the American Thoracic Society Pulmonary Function Standards Committee [43]. The total distance covered over 6-minutes was recorded and used to calculate the VO2peak based on ACSM formula VO2peak = (0.02*distance[m]) - (0.191*age[yr]) - (0.07* weight [kg]) + (0.09*height [cm]) + (0.26*rate pressure product [*10 -3]) + 2.45 [38].
MicroFET 2 handheld dynamometer (Hoggan Health Industries Inc. West Draper, UT, USA) was used to quantify isometric strength of the hamstrings and quadriceps of both lower extremities. Three trials were performed on each muscle group, in order to take the average. Patients were seated upright in the physiotherapy bed (height was raised so that the participants feet were not in contact with the floor), with hips and knees fixed at 90° of flexion with a goniometer and both hands on the side. Moreover, a strap was placed around femoral bones just distal to the hip joint and another strap was used to stabilize the dynamometer above the ankle [44]. The protocol consisted of three maximum isometric contractions which would need to be sustained for 3 seconds. Verbal encouragement was given to the participants to produce a maximum effort. Then the assessor applied the "break technique", which overpowers patient’s maximum effort and therefore produces an eccentric muscle force.
OMNI-RES scale (0 = extremely easy to 10 = extremely hard) was used during training sessions as another way to monitor exercise (internal) load [45]. During familiarization session, participants were trained how to use the scale. At the end of each of the two cycles of the exercise session, participants rated their overall perception of how hard the exercise felt.
Participants were instructed to avoid food, caffeine or alcohol at least 5-hours prior to the exercise session. Participants trained 2 times per week on non-consecutive days. The training program lasted 8-weeks in total and was under the supervision of a physiotherapist. The training session always commenced with a general warm-up of 3-mins (toe taps, heel taps, marching on the spot, step jacks, split squat jacks, skier jacks) and finished with a 3-min cool-down (toe taps, heel taps, quadriceps stretching, hamstrings stretching, triceps stretching, pectoralis stretching) at 40-50% of HRR. During the main part of the program participants completed 2 circuits, with 6 stations per circuit and 10-12 repetitions per station. A total of 4 cardiovascular (CV) stations and 2 Active Recovery (AR) stations were performed, each lasting for 1-minute. One AR station was performed after 2 CV stations. Participants trained during CV stations at 50-60% HRR for the first 2-weeks and at 70-85% HRR for the rest of the program. AR stations were performed at 40-50% HRR for the first 2-weeks and at 50-60% of HRR for the following weeks. The intensity of the exercise was monitored through the Polar V800, which recorded the HR throughout the whole exercise session. The training protocol included the following exercise stations: (1) squat jumps, (2) medicine ball squat overhead throw, (3) wall push-ups or standing bicep curl, (4) two-handed dumbbell high step-up, (5) running, (6) dumbbell walking lunges. If the participant failed to reach at least 12 repetitions on a given set, the weight was reduced in the following set, whereas when > 12 repetitions were reached the weight was increased in the following set (following the OMNI-RES scale 8 ("hard, somewhat difficult"). Total exercising time commitment for each session was 12-minutes (without the warm up and cool down).
Statistical analysis was performed using SPSS software v.25(SPSS Inc., Chicago, IL). Normal distribution of the data was assessed using the Shapiro-Wilk test. Baseline characteristics between the two groups were compared using independent samples t-test. A 2 × 2 repeated measures ANOVA was performed to assess the effect of time (pre vs. post) and group (HICT vs Control) for all variables. Only VO2peak was analysed using a 2x3 repeated measures ANOVA as it was assessed at three time points (pre, post and 2 months follow up). For non-normally distributed variables the corresponding non parametric tests were used. Statistical significance level was set at p < 0.05. Effect sizes for main effects and interaction were calculated by partial eta-squared (η2p) with the magnitude of effect sizes determined as: small η2p ≤ 0.01, medium η2p ≥ 0.06, and large η2p ≥ 0.14 [46]. Data are presented as mean ± SD for normally-distributed data and median (interquartile range) for non-normally distributed data. Power analysis using G*power (3.1.9) revealed a sample size of 14 individuals per group was necessary to observe a moderate group by time interaction effect (Cohens d = 0.57) in VO2peak with a level of significance at 0.05 and power of 0.8.
Participants baseline characteristics are presented in Table 1 (See Figure 1 CONSORT). Significant differences between the two groups at baseline were found only for gender, LDL, TC and the strength of the right quadriceps muscle. All the other variables were similar between groups at baseline.
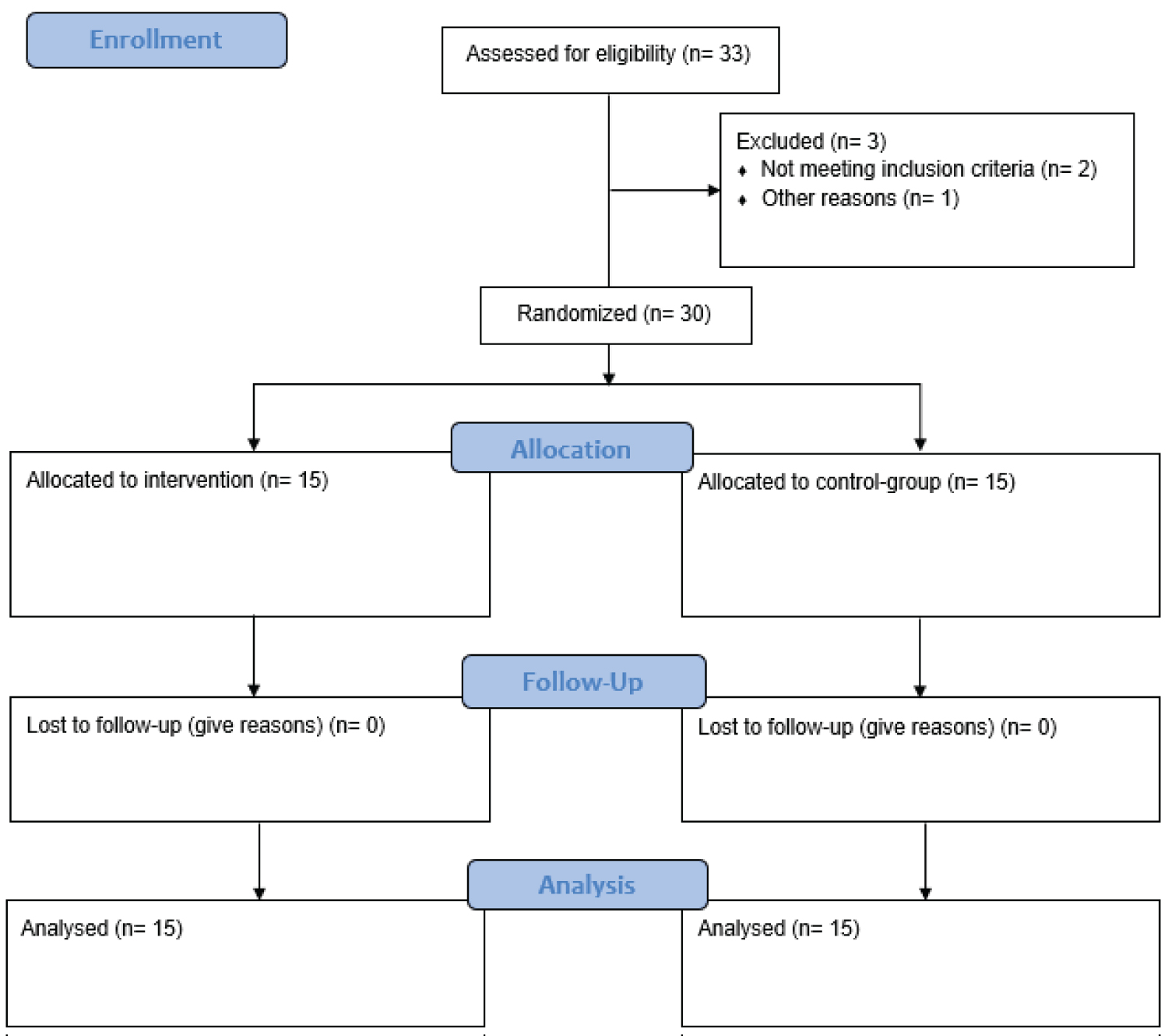 Figure 1: CONSORT flow diagram.
View Figure 1
Figure 1: CONSORT flow diagram.
View Figure 1
The drop-out rate during training and the loss to follow up was 0%. The training adherence for the participants who completed the exercise protocol was 100%. Only one participant reported feeling unwell, immediately after the first session, due to a major drop in BP. Participant recovered completely within 5 minutes with some rest and fluid replenishment with an energy drink. Nevertheless, no major cardiovascular or musculoskeletal adverse events were reported during or immediately after the training sessions.
There was a significant group x time interaction in BW (p = 0.001, η2p = 0.62), BMI (p = 0.001, η2p = 0.56), BF% (p = 0.001, η2p = 0.48), BF(Kg) (p = 0.001, η2p = 0.40), WC (p = 0.001, η2p = 0.39) and hip circumference (p = 0.006, η2p = 0.24). The mean % difference (Post-Pre value/Pre Value x100%) in BW was 0.3% (± 0.70) for the control-group and -3.6% (± 1.96) for the HICT-group. Moreover, the % differences were 0.2% (± 1.41) and -3.5% (± 1.91) for the BMI, 3.1% (± 4.18) and -4.5% (± 3.88) for the BF%, 3.7% (± 6.61) and -7.9% (± 4.81) for the BF(Kg) for the control-group and the HICT-group respectively. The % difference in WHR was 0.61% (± 0.29) and -3.4% (± 13.80), in hip circumference was 0.4% (± 0.90) and -1.3% (± 19.95), in WC was 0.4% (± 1.01) and -2.7% (± 2.67) for the control-group and for the HICT-group respectively (Table 2).
Table 2: Outcome variables at baseline and after 8-weeks. View Table 2
None of the biochemical markers demonstrated any statistically significant group x time interaction (η2p from 0.003 to 0.075) (Table 2) however the percentage differences favoured the HICT group. The % difference in LDL was -4% (± 14.79) and 4.4% (± 24.29), in HDL was -0.3% (± 8.83) and 13.8% (± 56.68) for the HICT-group and for the control-group respectively. In addition, the % difference in TC was -3.2% (± 8.46) and -0.7% (± 23.03), in glucose was -1.1% (± 6.44) and 4.5% (± 8.68), in triglycerides was 2.6% (± 44.53) and 17.5% (± 44.70) for the HICT-group and for the control-group respectively.
SBP demonstrated a significant group x time interaction (p = 0.002, η2p = 0.29), similar to DBP (p = 0.001, η2p = 0.39) (Table 2). The % difference in SBP was 3.1% (± 5.93) and -2.9% (± 4.11) and in DBP was 5.5% (± 8.67) and -4.6 (± 3.89) for the control-group and the HICT-group. Moreover, significant group x time interactions were found in MAP (p = 0.001, η2p = 0.41) and HR (p = 0.001, η2p = 0.43) but not in RPP (p = 0.63, η2p = 0.008) (Table 2). The % differences for the HR were 3% (± 4.65) and -4.9% (± 4.40), for the RPP were 6.9% (± 10.86) and -7.2% (± 5.97), for MAP were 4.7% (± 7.19) and -4.8% (± 4.17) for the control-group and HICT-group respectively.
A significant group x time interaction was found for the VO2peak (p = 0.001, η2p = 0.31). From baseline to 8-weeks post-intervention, HICT-group demonstrated an improvement of 16.7% (± 11.74), in contrast to 2.3% (± 5.09) improvement in control-group. During the detraining period (follow-up), VO2peak decreased by 4.3% (± 4.05) in HICT-group and by 6.6% (± 10.62) in control-group. Despite this decrease, HICT-group had 11.6% (± 10.62) VO2peak increase from baseline to 2-months follow-up, whereas control-group had a decrease of -4.3% (± 12.45) (Figure 2).
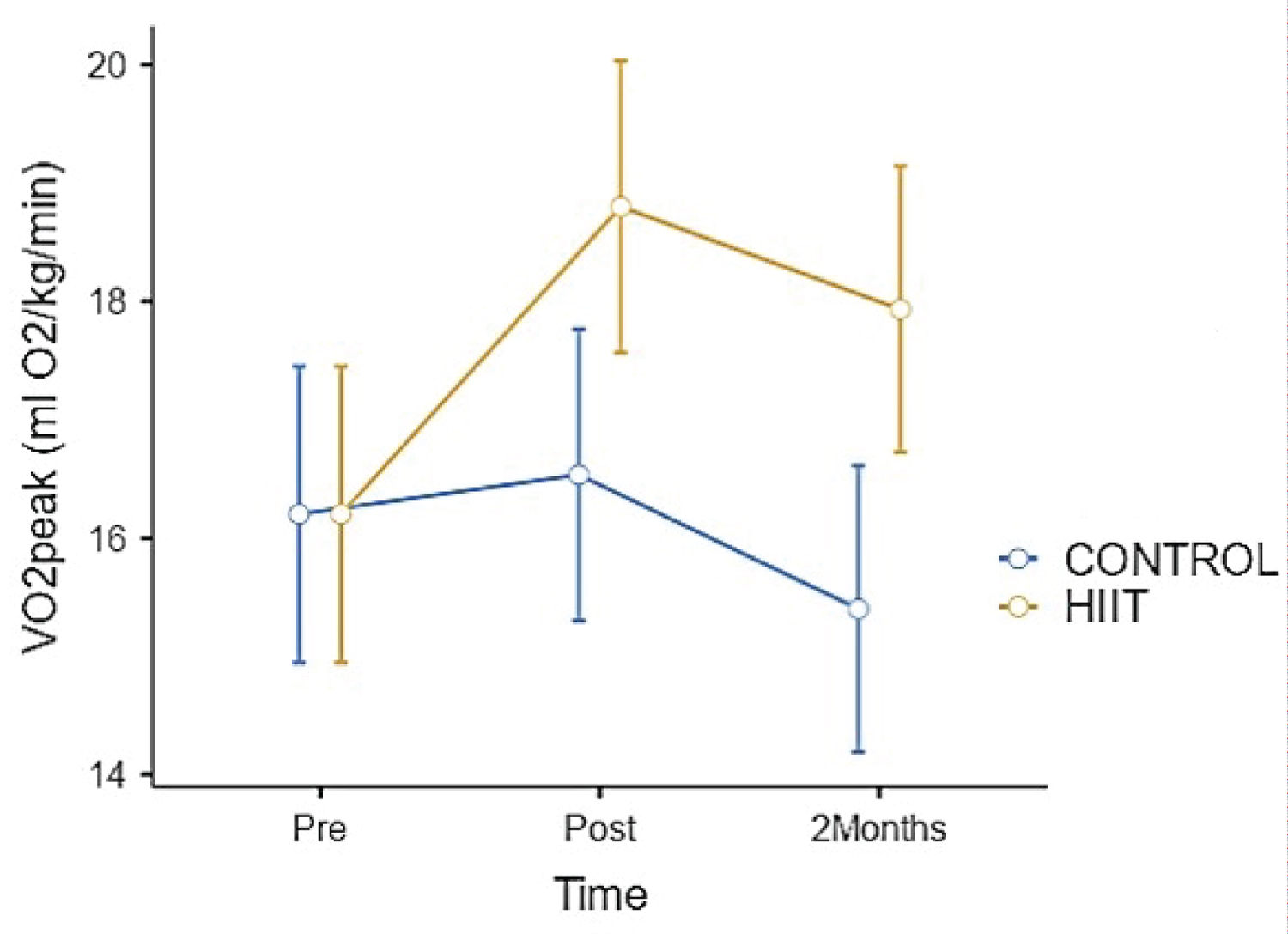 Figure 2: Changes in VO2peak at the three time points for both groups. Significant between group differences were found immediately post intervention (p = 0.013) and at two months (p = 0.005).
View Figure 2
Figure 2: Changes in VO2peak at the three time points for both groups. Significant between group differences were found immediately post intervention (p = 0.013) and at two months (p = 0.005).
View Figure 2
Pair wise comparisons demonstrated significant between group differences immediately after the intervention (p = 0.013) and at 2-months (p = 0.005). In addition, in the HICT-group significant differences were found from pre-intervention to post-intervention (p = 0.001), from pre-intervention to 2-months follow-up (p = 0.015) but not from post intervention to 2 months follow up (p = 0.196). In line with VO2peak results, OMNI scale showed that the HICT-group had significantly lower feeling of exertion (p = 0.003) at the end of the program. The average % improvement of exertion was -13.4% (± 10.62) (Table 2).
Significant group x time interactions were found only at the left lower limb, which was the non-dominant limb (left hamstrings p = 0.002, η2p = 0.30 and left quadriceps p = 0.001, η2p = 0.31) (Table 2). On the other hand, no significant differences were found on the right lower limb (hamstrings p = 0.20, η2p = 0.06 and quadriceps p = 0.6, η2p = 0.01).
Significant differences in body composition, physiological variables and fitness were found with a minimal intervention of 2 exercises sessions per week. The duration of the main body of the session was only 12-minutes with an additional 6 minutes for warm up and cool down. This brings the total duration of each exercise session to the 18-minutes. This means that a commitment of 36-minutes per week is able to reduce the most common cardiovascular risk factors and increase the fitness of obese and overweight individuals. Lack of exercise is associated with a higher risk of chronic diseases, while being physically active is linked to a 25% reduction in deaths from chronic diseases [47]. The important finding of this study is that an 8-week multimodal CT program with high intensity is able to induce favourable health benefits in obese and overweight but apparently healthy individuals, despite being 39-minutes less than the current, intense, physical activity recommendations by WHO.
Unlike most HIIT studies, the protocol of the current study was functional HICT, which is low cost and does not require expensive equipment or specifically designed space. Despite the short duration 8-(weeks) and frequency of the study (2 weekly sessions) significant results with large effect sizes (η2p between 0.24 and 0.62) were found in all body composition variables including BW, BMI, BF%, BF-kg and body circumference. Similar beneficial results in body composition have been reported by other studies. However, these studies utilised higher frequencies (3 sessions per week) and longer durations (9-12 weeks) with twice as much exercise time (50-60 minutes per session) [30,35,48]. To our knowledge this is the first study to show meaningful improvements with a short duration, low frequency HICT program.
WC is one of the key screening variables used to identify those with metabolic syndrome [49]. In this study, an average reduction of ~3% in WC and ~1% in hip circumference was found. The results of WHR are in accordance with another study which used a progressive CT protocol for 8-weeks (4 circuits x 8 exercise stations at 65-85% of 1 repetition maximum, lasting 60-mins) [50]. Other studies reported circumference changes of 2.4 cm and 1.4 cm following 2-weeks of sprint interval training or HIIT but used a more strenuous exercise protocol [51] or a longer training session (60-mins) [51,52]. However, the small reductions in circumference from this 8-weeks, low-cost HICT program were found despite no changes in diet and everyday physical activity.
No meaningful changes were found in any of the biochemical variables. Obesity has a direct link with increased levels of triglycerides, as they are the main fat storage [53], and this was shown to increase the risk of cardiovascular diseases [54]. Participants in the exercise group demonstrated a 9 mg/ dL reduction in triglycerides but this was not statistically significance. It has been reported that when participants have lower baseline levels of triglycerides, there is only a small reduction post-exercise, whereas when triglycerides levels at baseline are high, the reduction is significant [55]. Taking into consideration the normal baseline triglycerides levels of the participants in this study, it was no surprise the effect of the program was not significant. Most previous studies except one [56] found significant changes in lipid profile [30,50,57] therefore the training variables used in the current study were not able to induce this particular adaptation. If this lipid profile is the most important adaptation required, we recommend to increase the duration of the program by at least 4 weeks and/or the duration of the session to 50 minutes while keeping the intensity high.
VO2peak is a well-recognized indicator of cardiorespiratory fitness [58,59] and its reduction is associated with health issues and premature death [60]. A ~17% increase in VO2peak was found following 8 weeks of HICT for only 36 minutes per week. During the 2 months detraining period there was still a 12% improvement compared to baseline in the exercise group. These results are consistent with previous reports by Ballesta-García et al. [33] and Ludin et al. [56] which used HICT for 18-weeks and 12-weeks in older, obese women and obese female students respectively [33, 56] and better than those reported by Sperlich et al. [35] following 3 weekly HICT sessions for 9-weeks [35]. Considering the minimal dose of the current program we suggest HICT is a time efficient mode of training to improve cardiorespiratory fitness and it has the potential to increase adherence.
Participating in physical activity has been recommended as an effective non-pharmacological approach to improve BP [61]. This study demonstrated that 8-weeks of a HICT program decrease BP. Mean SBP for exercise group changed from 120.0 to 116.3 mm Hg and DBP from 82.5 to 78.5 mm Hg following the exercise protocol, which based on American Heart Association [62], represents a mean change from "elevated blood pressure" category down to "normal blood pressure" category. Similar results have been reported by other studies [30] reinforcing the notion that a short duration, high intensity program can lower BP. Ludin, et al. [56] reported no significant reduction in SBP and DBP of obese females [56] but perhaps the work to rest ratio (1:1) was not adequate to maintain the intensity high enough to induce this adaptation. Several physiological explanations have been reported, such as improved vascular function and diameter post-exercise, which can explain this improvement in BP [63]. BP can also decrease due to the reduction of sympathetic nervous system activity with exercise, normalisation of arteriolar morphology and reduction of peripheral resistance to blood flow [64]. Previous studies reported that HIIT or even moderate intensity continuous training demonstrated beneficial improvements in vascular diameter, thus improved SBP [65,66] however, this mechanism is merely hypothetical as vascular diameter was not measured in this study.
A lower resting-HR in the study can be explained by central and peripheral changes resulting from exercise. Central changes such as an increase of venous return and systolic volume, an improvement in myocardial contractility as well as peripheral ones such as an improvement in oxygen extraction or O2 use, can explain the HR reduction [67]. The results of the current study are in line with Miller, et al. [31] and Ballesta-Garcia et al. [33], who also found a reduction of resting HR from 84bpm to 71bpm and from 100bpm to 80bpm, respectively [31,33].
RPP directly indicates the energy demand of the heart, which is related to myocardial blood flow [68]. No significant changes were demonstrated in RPP post exercise. It was reported by Halliwill et al. [69] that after an acute bout of moderate exercise, baroreflex control of HR and blood vessels is clearly regulated [69]. Thus, sympathetic drive to the heart increases, while there is a reduction in sympathetic drive to blood vessels. Therefore, exercise intensity can affect the baroreflex control of HR, but not the baroreflex control of blood vessels.
Muscular strength is negatively and independently associated with all-cause mortality, even after controlling for cardiorespiratory fitness or BMI [70,71]. Participants in this study showed an improvement only in the isometric strength of the left lower limb. A study by also reported strength improvements only in one limb in overweight females following 12 weeks of CT with hydraulic resistance machines (3x40 minutes per week). Strength increases can be the result of muscle size growth or due to neural adaptations [62]. Since LBM did not change in the experiment group, the observed increase in strength was due to neural mechanisms. In addition, since most subjects were right side dominant (83.33%), the unilateral effect suggests that the dose of the program was enough to produce strength adaptations only in the non-dominant and therefore the more unaccustomed to intense physical activity limb.
This study has several limitations which might affect the generalisability of the results. There was no record of the daily physical activity and the food intake of the participants during the 8 weeks of the intervention so the effect of these factors is difficult to be ascertained. The small number of participants in each group probably requires confirmation by larger studies, nevertheless the results are promising. In addition, participants were obese and overweight but apparently healthy, without any comorbidities and it is difficult to generalize the results in the whole obese and overweight population. Finally, groups were not balanced in terms of gender, which might have affected the results.
Overweight and obese individuals demonstrated significant improvements in several health markers, with only 36-minutes of HICT per week for 8-weeks in total. It seems that a low cost, functional CT program can be used by health care professionals in order to manage obesity and reduce some of the risks for cardiovascular diseases. CT due to the short duration of the exercise session, the low-tech equipment needed to perform the exercises and the ability to monitor the results with readily available equipment is an ideal prevention strategy in small physiotherapy clinics or at home. However, further research can optimise these results perhaps by manipulating further the exercise parameters or by combining exercise with a diet plan.
The authors wish to thank the participants for their participation in this study.
The authors received no financial support for this study.
The datasets used and analysed during the study are available from the corresponding author on reasonable request.
Approval to conduct this study was obtained from Cyprus National Bioethics Committee (ΕΕΒΚ/ΕΠ/2017/38). Verbal and written consent were obtained for all participants before any measurements.
Not applicable.
The authors declare no competing interests.