Background: The epidemiology of injuries in youth soccer is ambiguous. Most studies are based on the consensus statement of Fuller, et al., where pediatric-specific injuries are not included. As a result, this type of injury is often neglected or categorized inconsistently. A consequence may be adhering an incorrect focus in injury prevention. This study aimed to describe injury incidence, severity and burden by age group in an elite soccer academy.
Methods: We included injury data recorded over four consecutive seasons from 2017/2018 to 2020/2021 from all male youth players (under-8 to under-19) of an elite Dutch soccer academy. The outcome measures were soccer-related time-loss injury incidence (per player-season), severity (days lost) and burden (days lost per player-season).
Results: We identified a total of 1,134 soccer-related time-loss injuries in 979 player-seasons of 406 individual players. The incidence was 1.2 (95% CI 1.10; 1.23) time-loss injuries per player-season, with a median severity of 13 (interquartile range; 6, 27) days lost per injury. The overall injury burden was 15 days lost per player-season (5% unavailability), with a peak in the under-16 age group of 37 days lost per player-season. Incidence peaked in the under-15 with 1.9 injuries per player-season and severity peaked in the under-16 with a median of 20 days lost per injury. Apophysitis of the knee was the most burdensome injury subtype with a peak in the under-14 age group of 11 days lost per player-season.
Conclusion: The overall injury burden results in a 5% players' unavailability for training and/or competition, with a peak in the under-16 of 12% unavailability (37 days lost per player-season), mainly due to an increase in severity. Apophysitis had a proportion in overall incidence of 21% and was the most burdensome injury type (5 days lost per player-season), especially in the knee (3 days lost per player-season).
Soccer, Prevention, Epidemiology, Pediatrics, Injury, Physis
Elite soccer academies are increasingly vital to their clubs for multiple reasons. First, fourteen years ago UEFA implemented the 'Home-grown Players' rule requiring a minimum number of home-grown academy players in their first team [1]. Second, the market of youth players is becoming increasingly lucrative. In the last five years, transfer fees in the under-20 have tripled [2]. It is important to ensure the health and well-being of young players in modern soccer, where higher physical demands are placed on players, not least due to the increasing speed, intensity and quantity of matches [3]. The first step in an injury risk mitigation plan is to describe the injury trends in the academy [4].
Previous epidemiological studies in elite youth soccer reported an injury incidence ranging from 0.4 to 2.2 injuries per player season [5-12]. The most common injuries were muscle [5,8,9,11-21] and/or ligament injuries [6,12,22]. Most studies report a linear distribution across age groups; the injury incidence increased with age. Several other studies found an incidence peak around the age of 15 years [7,11,12]. Growth-related injuries had the highest incidence until the under-13 age group, after which muscle strains predominated. Muscle strain incidence increased with age with the highest incidence in the under-17/under-18 age group [17].
The main limitation is inconsistency in reporting pediatric-specific injuries. Most studies are based on the consensus statement of Fuller, et al., where pediatric-specific injuries are not included. In absence of clear definitions, terms like growth related [7,9,10,20,23], bone [19,22], overuse [5] or osteochondrosis [6] injuries are used. As a result, this type of injury is often neglected or categorized inconsistently. A consequence may be adhering an incorrect focus in injury prevention. In elite youth soccer there is a need for more epidemiological data including these pediatric-specific injuries.
This study aims to describe injury incidence, severity and injury burden in categories based on age group, injury location and injury type, including pediatric-specific injury types in an elite Dutch soccer academy.
This descriptive retrospective cohort study included prospective collected injury data from all male youth players from the under-8 to under-19 teams of an elite soccer academy in The Netherlands. Where players participate in the highest division of their age groups and are trained to become adult first-team elite players. Data from four consecutive seasons (from 2017/2018 to 2020/2021) were included. On average, players have 10 weeks off a year. No matches/training can be missed during this time. Informed consent for the use of injury data for scientific purposes was repeatedly obtained at the start of every season from the player himself and/or both their guardians/parents when the player was beneath 16 years of age.
Injuries were diagnosed by the sports physician or physiotherapist and reported in an electronic medical reporting system (Smartabase Athlete from Fusion Sports Pty Ltd) as part of their normal clinical routine. If indicated additional imaging (e.g., ultrasound, X-ray, CT-scan or MRI) was performed. The classification was based on the consensus statement of Fuller, et al. [24], which was extended to include the pediatric-specific physeal injury, apophysitis, as preferred by the club. The injury report included the date, location and type of injury. The injury definition used in this study closely followed the recommendations of Fuller, et al. [24].
Injury: A physical complaint sustained by a player that results from a soccer match or training.
Time-loss injury: An injury that results in a player being unable to take full part in future soccer training or match play.
Medical attention injury: An injury without time-loss.
The medical staff determined the diagnoses and classified them into injury location and type. The injury location was subdivided into head, neck, sternum/upper back, abdomen, low back/pelvis, shoulder/clavicle, upper arm, elbow, forearm, wrist, hand, hip/groin, thigh, knee, lower leg/Achilles tendon, ankle and foot/toe. In addition to the consensus statement by Fuller, et al. [24], buttock was added as an injury location.
Injury type was subdivided into concussion, fracture, other bone injury, dislocation/subluxation, sprain, meniscus or cartilage injury, strain, tendon injury, overuse not specified, hematoma/contusion/bruise, abrasion, laceration, nerve injury and other injuries. In addition to the consensus statement by Fuller, et al. [24], synovitis/effusion and apophysitis were added as injury type.
Injury subtypes were formed by linking location and type. For instance; knee, ligament injury or ankle, ligament injury.
The injuries were cross-checked individually by the coordinating researcher for consistent classification based on the diagnosis and injury report described by the medical staff in the database. In case of incorrect classification, the classification was revised and classified according Fuller, et al. [24]. When an injured player left the academy, the sports medicine physician estimated the expected time-loss as described by Fuller, et al. [24].
The data was transferred from Smartabase Athlete Management to IBM SPSS Data Editorusing Microsoft PowerBI.
Injury incidence is the number of time-loss injuries per player season. Severity is measured in days lost, divided into minimal (0-3 days), mild (4-7 days), moderate (8-28 days) and severe (> 28 days) [24]. Day of which the injury occurred is defined as day 0, and time-loss was counted until clearance for team training and match availability. Clearance was given by the sport physician and/or physiotherapist as part of normal clinical routine. Injury burden [25] is expressed in days lost per player season.
For incidence, we assumed a Poisson distribution [22]. The Poisson-based meantime-loss incidence was determined per season and translated into overall incidence and 95% confidence interval. For the selection of descriptive statistics for severity, data was checked for normal distribution using a ShapiroWilk test in IBM SPSS Data editor. In the case of normally distributed data, the mean and 95% confidence interval were presented. If the data was not normally distributed, the median and interquartile ranges were presented. Injury incidence and severity were combined to calculate the injury burden per categorical variable.
The cohort totaled 979 player seasons in 406 individual players. The number of player seasons per age group is described in Supplemental Table S1.
A total of 1134 time-loss injuries were found out of a total of 1300 injuries. 166 injuries (13%) were medical attention injuries, causal injury subtypes can be found in Online Supplemental Table S2. The 1134 time-loss injuries (87%) had a total of 31067 days of time-loss. 73% (296 out of 406) of individual players suffered one or multiple soccer-related injuries during this period.
The overall time-loss injury incidence was 1.2 (95% CI, 1.1-1.2) per player season with a median time-loss of 13 (95% CI, 12-14) days lost, resulting in an injury burden of 15 days lost per player season. A complete overview of all data of the injury incidence, severity and burden per age group and injury subtypes can be found in the Online Supplemental Table S2.
The injury burden in the academy is distributed across the age groups as shown in Figure 1. The under-16 has the largest time-loss injury burden with 37 days per player season and the under-8 has the smallest burden with 3 days per player season.
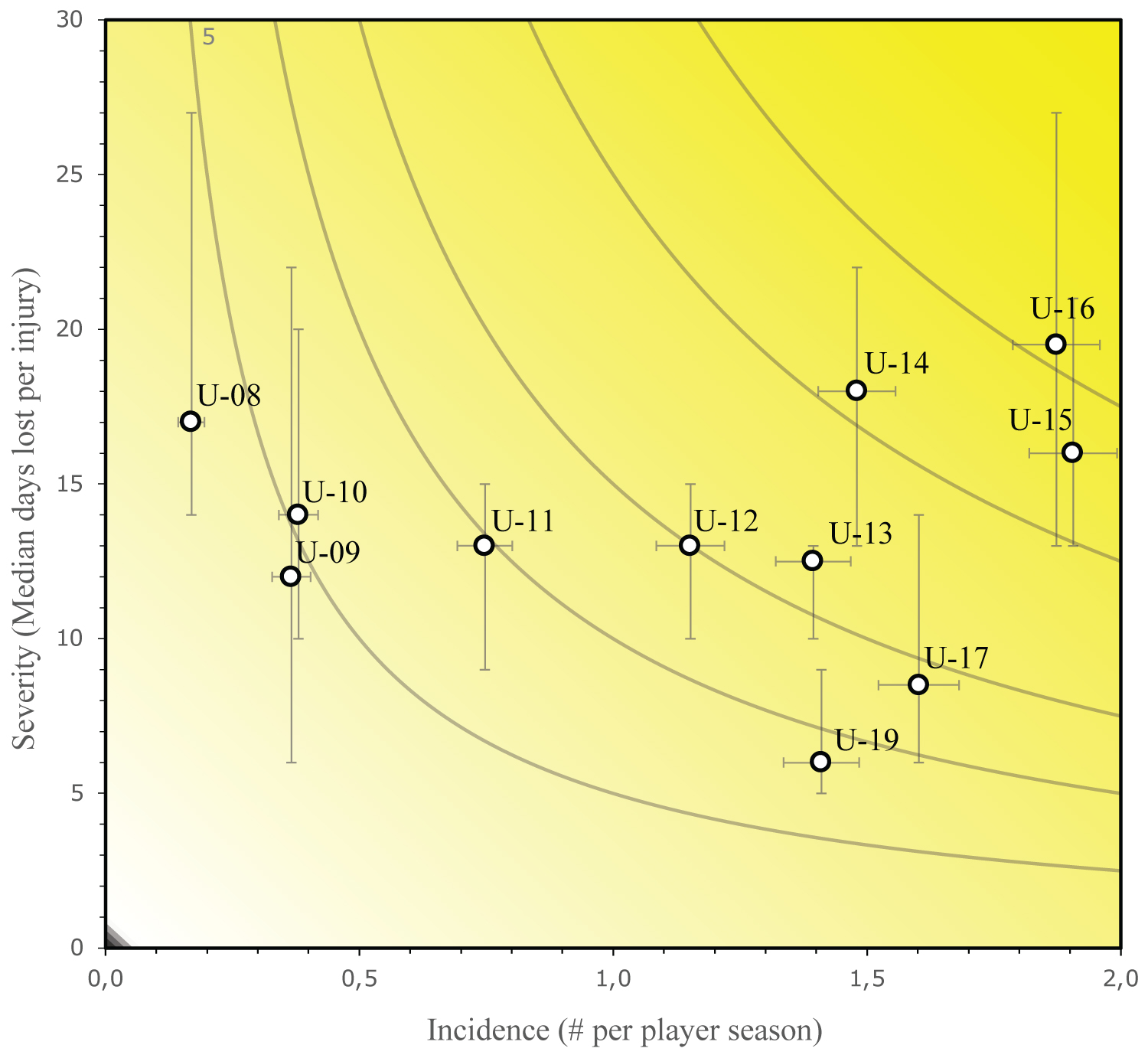 Figure 1: Risk matrix illustrating the injury burden per age group. By plotting the incidence (# per player season against the severity (median days lost per injury). The horizontal and vertical error bars represent the 95% CI ranges. U stands for "Under". The grey curved lines represent the same value of injury burden in days lost per player-season.
View Figure 1
Figure 1: Risk matrix illustrating the injury burden per age group. By plotting the incidence (# per player season against the severity (median days lost per injury). The horizontal and vertical error bars represent the 95% CI ranges. U stands for "Under". The grey curved lines represent the same value of injury burden in days lost per player-season.
View Figure 1
Injury incidence by location and type: The distribution of injuries based on location and type is shown in Table 1. 79% of the injuries affect the lower extremities. The knee, hip/groin and foot/toe were the most common injury locations. Muscle injury/strain and apophysitis were the most common injury types.
Table 1: Distribution of injuries based on injury location and type. View Table 1
Severity by location and type: 16% (176 out of 1134) of the time-loss injuries were minimal, 17% (190 out of 1134) were mild, 44% (504 out of 1134) were moderate and 31% (264 out of 1134) of the injuries were severe injuries, with more than 28 days lost. A knee injury accounted for 39% of severe injuries. Apophysitis accounted for 29% of severe injuries.
Injury burden by location and type: The risk matrixes show the time-loss injury burden per injury location (Supplemental Figure S1) and injury type (Supplemental Figure S2). The injury location with the largest injury burden was the knee with 6 days lost per player season. The injury type with the largest injury burden was an apophysitis with 5 days lost per player season.
The 10 most burdensome injury subtypes, injury type per injury location, of the entire academy are illustrated in Figure 2. An apophysitis of the knee has the largest burden with 3 days lost per player season.
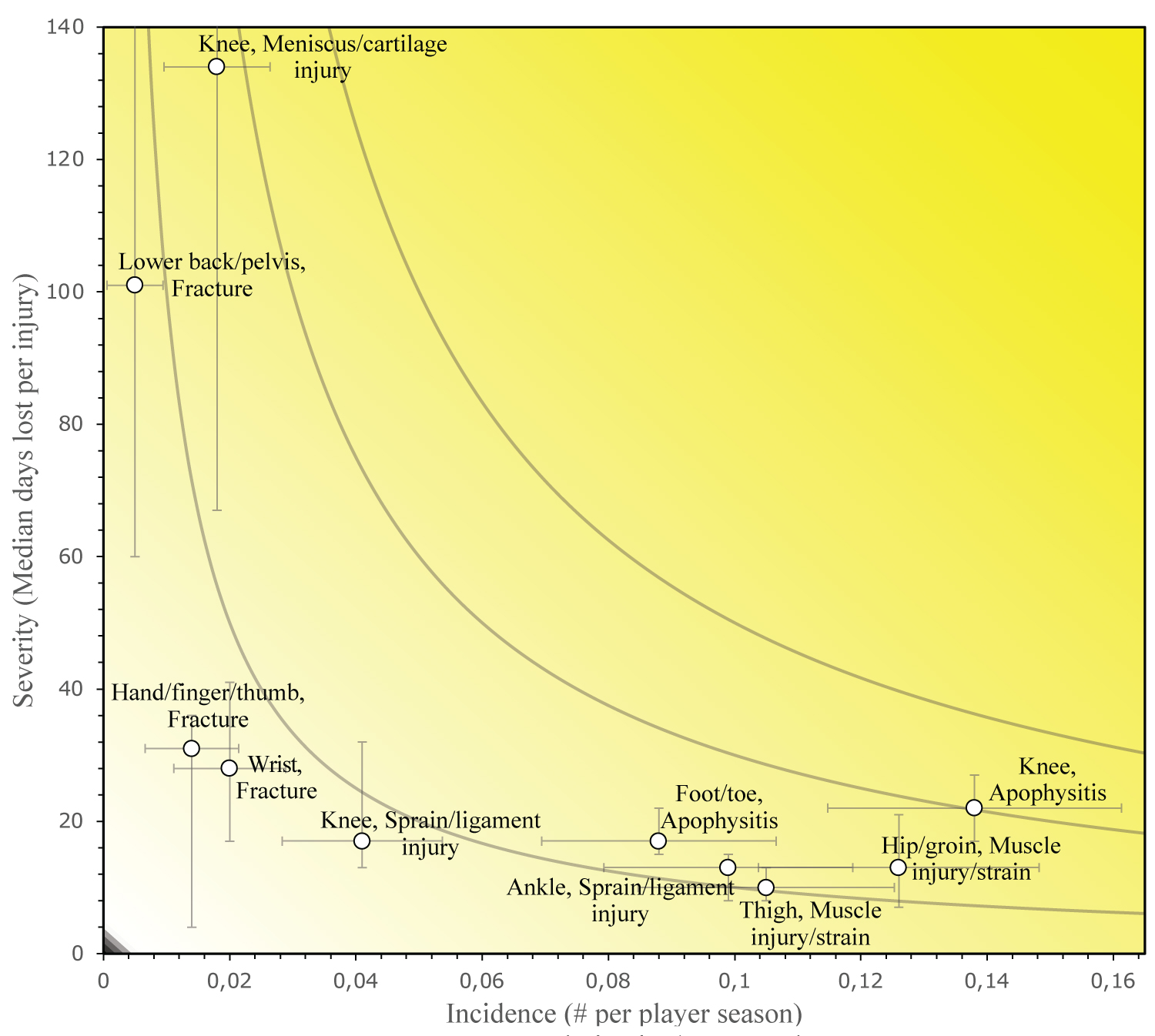 Figure 2: Risk matrix showing the injury burden per injury subtypes. By plotting the incidence (# per player season against the severity (median days lost per injury). The horizontal and vertical error bars represent the 95% CI ranges. The upper bound of lower back/pelvis fracture and knee meniscus/cartilage injury are respectively 301 and 219. The grey curved lines represent the same value of injury burden in days lost per player-season.
View Figure 2
Figure 2: Risk matrix showing the injury burden per injury subtypes. By plotting the incidence (# per player season against the severity (median days lost per injury). The horizontal and vertical error bars represent the 95% CI ranges. The upper bound of lower back/pelvis fracture and knee meniscus/cartilage injury are respectively 301 and 219. The grey curved lines represent the same value of injury burden in days lost per player-season.
View Figure 2
Table 2 shows the injury data of the three most burdensome injury subtypes per age group.
Table 2: Top 3 injury subtypes per age group based on injury burden. View Table 2
In this epidemiological injury study including 979 player seasons in age groups from under-8 to under-19, we found a time-loss injury burden of 15 days lost per player season. The distribution of injury burden across age groups showed a peak at the under-16 (injury burden 37 days lost per player season) with 12% unavailability for training and/or competition due to a soccer-related time-loss injury assuming a season lasts 300 days. Apophysitis had a proportion in overall incidence of 21% and was the most burdensome injury type (5 days lost per player season), especially in the knee (3 days lost per player season). The reported overall injury burden results in a 5% players' unavailability for training and/or competition.
The injury incidence of 1.2 injuries per player season is in the range of previously reported 0.4 to 2.2 injuries per player season [5-12]. The systematic review by Jones [5] reported that the moderate injuries (8 to 28 days) were the most prevalent, which is in line with our findings. The burden of 15.1 days lost per player season indicates that an elite youth player misses about 5% of the development time due to a soccer-related injury assuming a season lasts 300 days. This is in line with the study of Price, et al. [9], who found an unavailability of 6%.
For injury types, we found a high overall incidence of muscle strains and apophysitis. For muscle strains, this relative incidence is comparable with existing literature [5,8,9,11-21]. The injury type apophysitis has the greatest impact (5 days lost per player season) on players' availability due to a high severity. Comparison to existing literature was constrained due to several factors. Apophysitis was not always included as a specific injury in previous studies [8,11,13,14,16]. Some studies used other terms like growth related [7,9,10,23], bone [19,22], overuse [5], osteochondrosis [6], "other" [12] injury, knee strain [21] or Osgood Schlatter and Sever's disease [15,20]. A combination of the latter was made in order to compare our results with existing literature. The proportion of apophysitis incidence in overall incidence of 21% in our cohort exceeds the range of 3% to 17% found in existing literature. These are merely comparisons in proportion of incidence; due to differences in degree of exposure between studies, is a comparison of absolute injury incidence not possible. The wide range might reflect the lack of consensus across youth epidemiological studies on the definition of pediatric-specific injuries. Pediatric epidemiology studies are mainly based on the consensus of Fuller, et al. [24], where pediatric-specific injuries are not included. As a result, this type of injury is neglected or labelled differently in existing literature.
The injury incidence increases gradually with age with a peak at the under-16 age group after which it decreases. This distribution was demonstrated in some previous studies [7,11,12,16]. In contrast, studies in which there was a linear relationship predominated [5,6,8-10,13-15,17-23]. The median severity of injuries showed a peak around the under-15 age group. This pattern was also found in an injury audit of six Premier League academies [10]. The distribution of injury burden across age groups was parabolic with a peak at the under-16 (injury burden 37 days lost per player season). Skeletal maturity [7], rapid growth [26,27] and adolescent awkwardness [28] are often suggested as contributing factors for the higher injury burden in these age groups, but quality evidence to support this hypothesis is still lacking.
Injury types varied by age group, with apophysitis being the most burdensome. We observed a common pattern [23,29] where the affected site was distal(foot/toe) in the younger groups and became more proximal (knee, pelvis) with increasing age. A notable difference is that Gudelis, et al. [29] reported the majority of apophysitis (70%) in the pelvic region against 9% in our recent study. A variation in definition of injury type or a genuine difference in the incidence of pelvic apophysitis may be the cause of this difference.
One of the strengths of these studies is the cohort size and cohort period. This provides empirical value and validity of the conclusions. Injury report and classification was uniform and based on the consensus statement by Fuller, et al. [24]. We have included the injury burden as an outcome measure, which is clinically relevant as it reflects the extent of the problem [25].
A limitation is a risk of inconsistent classification of diagnosis because of the retrospective design. The club's standardized structured prospective surveillance program was set up according to Fuller, et al. [24], but we cannot exclude inconsistencies in classification during reporting. Through data cleaning we attempted to counter this. This process was not documented at the time, and cannot be described in detail. A difference from other epidemiological injury studies is the measure of exposure. While "per 1000 hours of exposure" was commonly used [24,30-32], we reported the incidence and injury risks "per player season" due to the lack of individual exposure data in the cohort. Future studies will include recordings of individual exposure and training load. Another limitation is that the female squads were not included in this cohort because of a difference in cohort period. The female youth academy started in the 2020-2021 season and will be included in future studies.
Pediatric-specific injury types were often absent or were included and classified inconsistently in previous studies. This argues for a classification that includes paediatric-specific injury types like apophysitis for the surveillance of youth sports injuries to give a complete overview.
The future offers opportunities to investigate etiology and risk factors of youth sports injuries. This will help to determine the focus of future preventive studies and interventions.
This data suggests that injury prevention programmes and injury prevention studies in youth soccer should focus more on apophyseal injuries, as this type of injury causes the highest injury burden in this cohort.
We found a time-loss injury burden of 15.1 days lost per player season. The distribution of injury burden across age groups showed a peak at the under-16 (injury burden 37.5 days lost per player season) with 12%, mainly due to an increase in injury severity. Apophysitis had a proportion in overall incidence of 21% and was the most burdensome injury type (4.9 days lost per player season), especially in the knee (3.0 days lost per player season).
The authors would like to thank all medical, performance and science staff that contributed to the data collection.
There was no external or internal financial support for this study.
The authors report there are no competing interests to declare.
Medical Research Involving Human Subjects Act (WMO) does not apply to this study and an official approval of this study by an ethics committee is not required, according to the Medical Ethics Review Committee of the Academic Medical Centre Amsterdam.
Informed consent for the use of injury data for scientific purposes was obtained from the player itself and/or their guardians/parents when the player was beneath 16 years of age.
GR, HT, BB collected injury data prospectively. VdB and LJ processed injury data for analysis. DH and GR conducted data cleaning. DH designed analytical tools and analyzed data. The first draft of the manuscript was written by DH and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.