To determine the prevalence and outcome of hysterectomy at the Douala General Hospital, Cameroon.
We carried out a descriptive, hospital-based cross-sectional study during the period January 1, 2005 to December 31, 2015. Retrospectively, we studied medical records and theatre registers of women who underwent hysterectomy. Using pre-specified criteria for data collection, we administered a pre-tested questionnaire in which socio-demographic factors, clinical characteristics, indication, type, hospital stay, and complications of hysterectomy were recorded. Data management was with Epi-info and analyzed with STATA version 10 (Stata Corp, Texas, USA).
The prevalence of hysterectomy was 14.54%; mean age 45.76 (SD 7.7) and 18.7% respondents had a previous cesarean delivery. Multiple leiomyomas (58.2%) and heavy vaginal bleeding (60.6%) were the main diagnoses for hysterectomy. Most respondents (79.5%) underwent total abdominal hysterectomy. The mean hospital length of stay was 6.07 (SD 1.92) days and average work experience of gynecologists was 8.6 (SD 1.1) years. Most complications (79.5%) were from total abdominal hysterectomy (p = 0.01).
One in seven women under age 45 with a diagnosis of multiple uterine fibroids and heavy vaginal bleeding undergo hysterectomy at the Douala General Hospital. There is a significant post-operative complication rate.
Prevalence, Hysterectomy, Uterine fibroids, Vaginal bleeding, Complication, Douala General Hospital, Cameroon
CNE: Conseil National d'Ethique; DGH: Douala General Hospital; HGD: Hôpital Général de Douala; NDVH: Non-descent Vaginal Hysterectomy; IUD: Intrauterine Device; SD: Standard Deviation; SPRM: Selective Progesterone Receptor Modulators
Hysterectomy is the surgical ablation of the uterus and is one of the most commonly performed gynecological operations. It was originally used mainly for benign pathology [1]. Vaginal hysterectomy, for its part, has been performed in most countries over the years. In recent times, with advancements in technology, most high-income countries have engaged in laparoscopic hysterectomy for both benign and malignant pathologies [2,3]. Furthermore, the technology trend has led to robotic-assisted hysterectomy [4-6]. The advantages of laparoscopic and robotic-assisted hysterectomy include less post-operative morbidity, short hospital stay and early resumption of work after surgery [6].
The trend in the uptake of hysterectomy has not been the same in most low and middle-income countries due mainly to socio-cultural and economic barriers [7] and to the absence in most of these countries of training programs for laparoscopic hysterectomy [8-10].
In Cameroon, hysterectomy is performed predominantly in referral hospitals based in cities, not only by gynecologists but also equally by general surgeons and general medical practitioners. Even nurses perform it, especially in rural areas. The mainstay of hysterectomy in Cameroon is total abdominal hysterectomy [11]. Most studies on the practice are descriptive or case series studies [11,12].
The aim of this study was to determine the prevalence and outcome of hysterectomy at the Douala General Hospital, Cameroon.
We hypothesize that there is a high prevalence of hysterectomy at the Douala General Hospital Cameroon and that this prevalence will reduce significantly if the known novel methods for treating uterine fibroids become accessible to the gynecologists of the DGH.
The scope of the study is limited to women who underwent a hysterectomy at the Douala General Hospital, Cameroon.
This was a hospital-based cross-sectional study using a pre-specified criteria for data collection conducted at the Department of Obstetrics and Gynecology of the Douala General Hospital (DGH) during the period 1st January 2005 to 31st December 2015. The period of data collection spanned from 1st November to 31st December 2015. The Douala General Hospital is a tertiary care health facility that offers specialised or scientific clinical care, research and teaching to a population of over two million inhabitants of Douala and its environs (Central African sub-region).
For convenience and for purposes of consecutive sampling, we included all medical records of women who underwent hysterectomy during the study period. Patients underwent hysterectomy for the following associated symptoms: Heavy menstrual bleeding, lower abdominal pain, painful heavy bleeding, abdominal mass, dyspareunia, and dysuria. Exclusion criteria for the study were patients who underwent hysterectomy out of the DGH and those with incomplete medical records.
Ethical clearance for study was obtained from the National Ethics Committee (Code: 083/CNE/SE/2014), and authorization to have access to medical records was obtained from the Director of the DGH (Code: HGD/020/BPE/ZM/10/2014).
All procedures were performed in accordance with the ethical standards of the Declaration of Helsinki [13].
At first, there was a pre-specified criterion for data collection and a final year medical student trained for the purpose did the data collection. Information abstracted from the files include socio-demographic and socioeconomic status, and clinical information (obstetric and surgical), mainly age, diagnosis, type of abdominal incision (midline or low transverse), type of hysterectomy (total, subtotal or radical) [14], and route (abdominal, vaginal) or laparoscopic [2]. We also recorded any associated procedures, intraoperative complications, blood loss and febrile morbidity. For this study, blood loss ≥ 500 ml was considered as a complication and a temperature ≥ 38 ℃ was considered as post-operative fever. Furthermore, we recorded information regarding the presenting complaint, hospital length of stay, day two hemoglobin levels and management of post-operative complications.
The data collected was coded and double-entered into a pre-designed template in Epi data, then exported to and analysed using STATA version 10 (Stata Corps, Texas USA).
The analysis focused on the prevalence and outcomes of hysterectomy. In computing the socio-demographic and obstetric characteristics of study participants, measures of central tendencies (mean, standard deviation and interquartile ranges) were used while frequencies and percentages were used to compute continuous variables and then summarized in tables.
A bivariate analysis was done to assess the measure of association between predictor variables and outcome variables with Chi squared test and differences between groups were determined by the Fisher exact test. A P-value of less than or equal to 0.05 was considered statistically significant.
During the study period, 3012 obstetric and gynecologic surgeries were performed at the Department of Obstetrics and Gynecology, of which 438 (14.54%) were hysterectomies. Among the 438 cases, only 410 (93.6%) were suitable for analysis (15 cases had no post operative notes and 13 cases had poorly filled or incomplete medical records).
The average age of study participants was 45.76 (SD 7.7). Majority, 63.4% (260/410) participants were in the age group 40-50. About 43.9% (180/410) respondents had given birth three to four times while 5.8% (24/410) were nulliparous. Besides, 34% (140/410) respondents had previous surgery and the most prevalent surgery was cesarean delivery in 18.7% (77/410). A greater number 60.67% (249/410) of respondents' presenting complaint was heavy vaginal bleeding and 58.2% (239/410) underwent hysterectomy because of symptomatic uterine leiomyoma (Table 1).
Table 1: Socio-demographic and clinical characteristics of study population. View Table 1
Furthermore, abdominal, vaginal and laparoscopic hysterectomy was reported in 79.5%, 14.6% and 5.9% (24/410), respectively (Figure 1). Besides, 95.9% (393/410) respondents underwent total hysterectomy while 3.9% (16/410) underwent radical hysterectomy. Low transverse incision was the most frequently used in 65.6% and the mean hospital length of stay was 6.07 (SD 1.92) days, 6.34 (SD 2.0) for abdominal and 5.02 (SD 1.09) for vaginal hysterectomy. The average working experience of gynecologists was 8.6 (SD 1.1) years (Table 2 and Table 3).
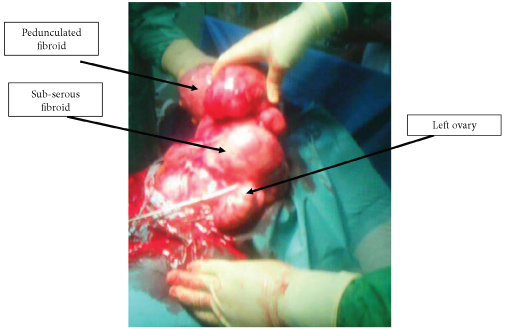 Figure 1: Total abdominal hysterectomy of a huge uterus with multiple uterine fibroids. View Figure 1
Figure 1: Total abdominal hysterectomy of a huge uterus with multiple uterine fibroids. View Figure 1
Table 2: Characteristics of Hysterectomies. View Table 2
Table 3: Indication and surgical route. View Table 3
The global intraoperative complication rate was 3.17% and complications were more common during abdominal hysterectomy, 2.7% mainly bleeding and bladder injury though this was not statistically significant (p = 0.25). Moreover, 11.95% (49/410) respondents had post-operative complications especially after abdominal hysterectomy in 11.2% (46/410). The most frequently occurring complication was fever in 6.1% (25/410), followed by anemia 3.7% (15/410). One patient (0.24%) had pulmonary emboli after laparoscopic hysterectomy. This was statistically significant (p = 0.01) (Table 4).
Table 4: Complications of hysterectomy and comparison between surgical routes. View Table 4
We carried out a study to determine the prevalence and outcome of hysterectomy at the Douala General Hospital, Cameroon.
Hysterectomy has been reported as one of the most practiced gynecological operations [1], but few studies have reported the prevalence of hysterectomy in Cameroon. Other African studies have reported a much lower incidence than our findings; 9.3% by Kouam, et al., 2005, 5.1% by Ahmed, et al., 2015, 9.29% by Awoleke, et al., 2012, 9.4% by Okunade, et al., 2017 [11,15-17]. The reason for this low prevalence of hysterectomy in African studies stems from the fact that women and their spouses will not readily consent to hysterectomy because of socio-cultural and financial barriers [7]. One study in a referral hospital in rural Cameroon reported that nearly one-fifth of patients presenting to a surgical clinic with a treatable condition did not ultimately receive needed surgery. Women in Cameroon believe that removing the uterus makes them incomplete [18]. That not withstanding, a Danish study reported a lifetime prevalence of 10.4% and a crude rate of hysterectomy of 3.4 per 1000 years with the 40-year-old having the highest rate 7.8 per 1000 year [19]. A woman without education had a 2.2 relative risk of having a hysterectomy compared with the educated woman [19].
The average age of 45.76 ± 7.7 reported in our study was higher than the 43.23 ± 8.23 years reported by Kouam, et al. in Yaoundé [11]. However, others have reported an average age for hysterectomy of 49.9 ± 12.6 years [17,20] although that for abdominal hysterectomy was 45.3 ± 7.4 [20].
This may have an impact on the reproductive health of the population since the menopausal age in Cameroon is around the fifties. Therefore there is need to look for alternative methods to manage these patients because majority of these women by the time of surgery had one to two children. The recent introduction of selective progesterone receptor modulators (SPRMs) such as ulipristal acetate (UPA) and aromatase inhibitors has added more possibilities to the medical options of treatment. Uterine artery embolization (UAE) has now been well recognized as a uterine-sparing (fertility-preserving) method of treating fibroids. More recently, the introduction of ultrasound waves (MRgFUS) or radiofrequency (VizAblate™ and Acessa™) for uterine fibroid ablation has added to the options of minimal access treatment [21,22]. However, most of these treatment modalities for uterine fibroids are not yet accessible to the Cameroon population. Firstly, they are too costly for the average Cameroonian and secondly, most hospitals do not have the technical and financial know-how to offer these services to their clients.
The main diagnosis for hysterectomies was multiple uterine fibroids accompanied with heavy and prolonged menstrual flow. This is consistent with other studies that report that uterine fibroids are the most common indication for hysterectomy in the USA [21]. A study carried out in the USA with randomly selected women between the ages of 35 and 49 years (who were screened by self-report, medical record, and sonography) showed that the incidence of uterine fibroids by age 35 was 60% among African-American women, increasing to > 80% by age 50, whereas Caucasian women showed an incidence of 40% by age 35, and almost 70% by age 50 [21]. This corroborates studies that report that uterine fibroids are more frequently found among the black race [23].
Total abdominal hysterectomy has been the main type of hysterectomy performed in our Department. The reason for this trend has been because patients come to the hospital relatively late and in acute conditions of anemic or hemodynamic instability. Such patients will not be suitable for laparoscopic or vaginal surgery. In addition, a good number of gynecologists in our Department have not acquired training to perform both laparoscopic and vaginal hysterectomy. It is noteworthy that with the advent of the new technologies for treating uterine fibroids, there is competition amongst physicians in high-income countries to adapt to the new surgical instruments and improve on their surgical skills. In the same light, the administrative staff of hospitals in most high-income countries serves as drivers to foster or boost this trend by providing appropriate medical equipment to gynecologists. This has not been the case in the Douala General Hospital and other hospitals in low-income countries. There is lack of an appropriate maintenance policy that safeguards the constant functioning of medical equipment at the Douala General Hospital. It is not unusual to temporarily suspend laparoscopic surgery for some time because of lack of an essential instrument like the bipolar forceps. Other pitfalls are the lack of continuous medical training/refresher courses that could help upgrade medical practitioners, and the lack of collaboration among gynecologists that impedes transfer of knowledge. Besides, gynecologists in our Department have been trained in different residency programs from different countries and their skills/competences in performing hysterectomies differ considerably. This is not consistent with other studies that have reported homogeneity in training and practice in their hospitals leading to a high technicality index in performing hysterectomies. The study carried out in Quebec, Canada, showed that the proportion of hysterectomies done by laparoscopy increased over the years while vaginal hysterectomies remained stable. Therefore, the number of abdominal hysterectomies was declining and the technicality index was increasing in Quebec. This was attributed to an increased use of medical alternatives and the presence of gynecologists better trained in advanced laparoscopic surgery [24,25].
The mean hospital length of stay for laparoscopic hysterectomy in our study was comparable with that of vaginal hysterectomy. The reason for this was because at the time of this analysis we were less experienced with the practice of laparoscopic hysterectomy; we therefore preferred to observe the patients longer than usual in hospital. However, women who underwent abdominal hysterectomy had the longest hospital length of stay. This was consistent with other studies that reported that non-descent vaginal hysterectomy (NDVH) should be the procedure of choice unless contra-indicated. Not only is it the least time consuming and also has the least intra-operative and post-operative complication rate, it is equally cost-effective and cosmetically appealing [26]. Radical hysterectomy for cervical cancer was recorded in only 3.9% cases. The reason for this low value is because patients come to hospital with advanced stage diseases that are suitable for radiation or adjuvant chemotherapy. This has been reported in other studies [27].
There was a non-statistically significant association of intra-operative surgical complications of hysterectomy that was ascribed to total abdominal hysterectomy compared to the other surgical routes. Besides, intra-operative complications are usually associated with the skills and experience of the gynecologists, especially in patients who have had a previous surgical operation. In this study most of the complications were from younger and less experienced gynecologists and residents. Secondly, about 18.7% of cases had a prior cesarean delivery. This is consistent with other studies that reported that women with at least one previous cesarean delivery face an increased risk of complications when undergoing a hysterectomy later [28,29].
Post-operative complications are usually related to the surgical technique and the duration of surgery. The climatic conditions in Douala, hot and humid, with a lot of circulating particles, can also be associated with an increased risk of post-operative infection. Furthermore, Cameroon is a hyper-endemic region for Plasmodium falciparum [30]. Therefore patients may develop malaria after surgery because of the transient postoperative cellular and humoral immunosuppression that has been reported after different degrees of operative stress [31]. This may explain the statistically significant rates of post-operative complications. That not withstanding, we recorded one case of pulmonary embolism after laparoscopic hysterectomy. We managed the case with enoxaparin (Lovenox™), a low molecular weight heparin. Others have previously reported two cases of pulmonary embolism after laparoscopic cholecystectomy. Therefore, in spite of the low incidence of postoperative thromboembolic disease following minimally invasive procedures, the risk of pulmonary embolism must not be underestimated and its symptoms must not be under-diagnosed [32]. We have since then suggested a specific prophylactic scheme for patients undergoing laparoscopic hysterectomy at the Douala General Hospital, Cameroon.
This was a retrospective study where some medical records were incomplete and not suitable for study. Some theatre records did not have post-operative notes. There could also be recall bias in the study. Besides, this was a hospital-based study; therefore the results may not reflect the general trend of hysterectomy in Cameroon.
This study is among the few on hysterectomy in sub-Saharan Africa. It also highlights the difficulties (socio-cultural and economic) encountered by gynecologists to make patients consent to surgery in the African context. In conclusion, almost one in seven women under age 45 with a diagnosis of multiple uterine fibroids and heavy vaginal bleeding undergo hysterectomy at the Douala General Hospital. The post-operative complication rate was high.
We thank the staff of the Department of Obstetrics and Gynecology, Douala General Hospital, for assisting us during the management of the patients and throughout this study. TOE conceptualized and wrote the manuscript. TOE, FMK, JEN and MNJA were in the surgical team. ENE and FMK collected and analyzed the data. REM supervised the study. All the authors read and approved the final version of the manuscript.
Ethical clearance for study was obtained from the National Ethics Committee (Code: 083/CNE/SE/2014) and authorization to have access to medical records was obtained from the Director of the DGH (Code: HGD/020/BPE/ZM/10/2014).
Written informed consent for publication of any accompanying images was obtained from the patient. A copy of the written consent is available for review by the editor-in-chief of this journal. Furthermore, the datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no competing interests and did not receive any form of funding in carrying out this study.