To investigate the frequency, management, and consequences of gastrointestinal stromal tumors in thirty patients treated and followed up at a single site.
All gastrointestinal stromal tumor patients admitted to our institution from 2008 to 2018 were retrospectively reviewed. Demographics, clinical findings, and tumor features, pathological, radiological, and immunohistochemical observations, surgical technique, recurrence, and mortality were documented.
Thirty patients were selected for this study, the primary tumor locations were the stomach (46.7%) and small intestine (43.3%). Five (16.7%) gastrointestinal stromal tumors were classified as high risk for relapse, seven (23.3%) as intermediate risk and eighteen (60.0%) as low risk. Imatinib (400 mg/day) treatment was started postoperatively in 12 patients (7 patients with intermediate risk and five patients with high risk). With a median follow-up of 35.5 ± 12.9 months (range 2-54) twenty-four patients (80%) were disease free, while 5 had a local recurrence (16.7%), and a single patient died from hepatic metastasis (3.3%). The disease-free survival rate was 68% at 4 years.
In this study, the mitotic index and tumor size were found to be statistically significant regarding prognosis. A combination of targeted therapy and surgery is recommended for recurrent and metastatic gastrointestinal stromal tumors.
Gastrointestinal stromal tumor, AFIP Miettinen classification, Imitanib, Recurrence, Disease-free survival
GISTs: Gastrointestinal stromal tumors; GI: Gastrointestinal; AJCC: American Joint Committee on Cancer; HPFs: High-power fields; IHC: Immunohistochemistry; CT: Computed tomography; MRI: Magnetic resonance imaging
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumors of the gastrointestinal (GI) tract [1,2]. GISTs are rare, with a frequency of approximately 1:100,000 per year [2,3]. Patients with GISTs typically present between 50 and 80 years of age and the majority of tumors are random [4,5].
According to the American Joint Committee on Cancer (AJCC) Staging Manual, the most predominant areas for GISTs are the stomach (60%), small intestine (30%), rectum (3%), colon (1-2%), esophagus (< 1%), and omentum/mesentery (rare) [6].
Patients suspected of GISTs may have multiple symptoms such as early satiety, fatigue, anemia, intraperitoneal hemorrhage, GI bleeding, or abdominal pain. Some have acute abdominal pain that may require emergency medical attention [2,4,5,7].
GISTs are histologically categorized into 1 of 3 groups: 1) Spindle cell type (70%), 2) Epithelioid cell type (20%), or 3) A combination of both [8]. GISTs are typically positioned on the bowel wall; however, these may form masses that are serosal- or mucosal-based. Most GISTs present singularly as a well-circumscribed nodule [2]. Diagnostic approaches that have been routinely used are computed tomography (CT), MRI, endoscopy, and endoscopic ultrasound [9].
For histochemical detection and diagnoses of GISTs, CD-117 antigen, with a positivity rate of approximately 95%, has been used [10,11]. Other markers for GISTs may be used and include the CD-34 antigen, smooth muscle actin, desmin, and S100 protein [12].
The standard treatment for localized GISTs is surgical resection using an open or laparoscopic surgical technique; however, laparoscopy has been discouraged in patients with large tumors, due to the risk of rupture [4].
Miettinen and colleagues followed up 1,600 patients long-term and determined GIST guidelines for risk stratification. These guidelines were based on the mitotic index, tumor size, and tumor site [13].
In this report, we performed a retrospective analysis of patients, from our center, who was diagnosed with GISTs over the previous ten years. We then analyzed variables that might predict survival and disease recurrence.
Between January 2008 and February 2018, 30 patients diagnosed with GIST in the surgical oncology clinic were retrospectively evaluated from the hospital database based on demographic characteristics, medical history, preoperative evaluation, surgical methods and details, and pathological findings. Inclusion criteria of the study were patients with a confirmed diagnosis of the gastrointestinal stromal tumor. Exclusion criteria were age group 16 and below.
Cukurova Univesity Clinical Ethical Board approved the study.
Tumors were categorized based on the aforementioned approach proposed by Miettinen, et al. [8] (Table 1). The results were analyzed using multiple imaging methods of the upper or lower GI tract used to determine the initial diagnosis. Ultrasound computed tomography, and MRI images were assessed for identifying tumor margins, echogenicity, density or signal intensity, contrast enhancement, calcification level, necrosis, and ulceration.
Table 1: Risk of aggressive behavior (AFIP-Miettinen8). View Table 1
Mitoses were determined in 50 consecutive high-power fields (HPFs) from cellularly and mitotically active areas. Immunohistochemistry (IHC) was performed with the following antibodies: CD-117, CD-34, α-smooth muscle actin, desmin, and S100 protein.
Surgical resection was performed in all cases. Resections are classified as incomplete when the tumor is unresectable during discovery or when there is gross residual disease after resection. Complete resection is considered as excision of all gross diseases, independent of microscopic borders. According to the Union for International Cancer Control (UICC), R0 was defined as a complete resection, R1 as microscopic evidence of residual tumor at surgical resection margins, and R2 as macroscopic residual tumor at the surgical resection margin. Local recurrence was defined as the reappearance of the tumor at the initial site of the primary tumor. The follow-up period was defined as the time dating from the date of surgery to the last day of follow-up. Follow-up was conducted through telephone or clinic interviews every 3 months after surgery. Status for survival was as follows: alive, free of disease; alive with disease, and death from the disease.
SPSS 23.0 package was used for statistical analysis of the data. Categorical measurements are summarized as the number and percentage, and continuous measurements are summarized as the mean and standard deviation (median and minimum-maximum). Chi-square test or Fisher test was used to compare categorical variables. The estimated relapse time was calculated by Kaplan-Meier analysis. For all tests, the p-value was accepted as significant when below 0.05.
A total of thirty patients were histologically diagnosed with GISTs and were enrolled in the study. We could not operate because of comorbidity in 1 patient with suspected GIST, and we started preoperative imatinib treatment and then operated when surgical morbidity decreased. One patient with suspected GIST was diagnosed as well-differentiated liposarcoma according to the pathology report after surgical excision and was excluded from the study. The patients had a mean age of 63 years (range of 44-87), with sixteen men and 14 women comprising the investigation. Stomach GISTs accounted for 14 tumors (46.7%), small bowel GISTs for 13 (43.3%), esophagus for two (6.7%), and rectum for one tumor (3.3%).
Symptoms were associated with the location of the disease. Seven patients with abdominal pain, four patients presented with gastrointestinal bleeding, four patients with toxic shock due to hemorrhage and four patients with intestinal obstruction. Four patients were admitted to the intensive care unit due to toxic shock resulting from severe GI bleeding. After the vital signs of the patients recovered, endoscopy revealed that a stromal tumor was found in one patient at the ligament of treitz, in another patient in the duodenum and in the other two patients in the stomach. The patients underwent surgery later. In the patient with the intestinal obstruction, a tumor of approximately 20 cm was detected in the ileum. After correction of the vital signs, a segmental small intestine resection was performed (Figure 1a and Figure 1b).
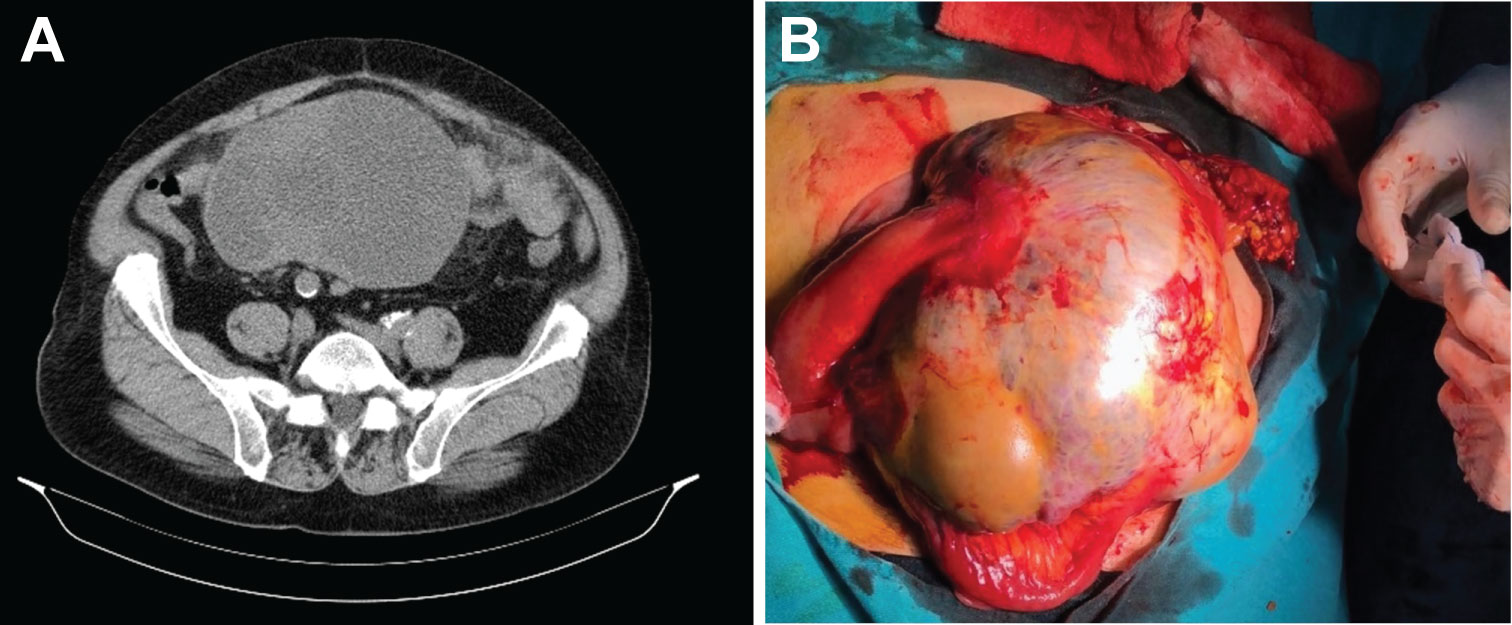 Figure 1: CT imaging a) and appearance during operation b) of a GIST located in small intestine (ileum).
View Figure 1
Figure 1: CT imaging a) and appearance during operation b) of a GIST located in small intestine (ileum).
View Figure 1
Four subjects were anemic, and one patient complained of stool issues caused by rectal GIST. The clinical data are given in Table 2.
Table 2: Clinical and pathological findings. View Table 2
Tumors ranged from 3 to 20 cm with an average size of 7 cm. For the mitotic rate, five mitoses per 50 HPF were found in 21 tumors (70.0%), and between six and ten mitoses per 50 HPF were found in six tumors (20.0%). Interestingly, more than ten mitoses per 50 HPF were found in three tumors (10%). According to the AFIP-Miettinen (8), 18 tumors were low risk, seven were intermediate risk, and five were high risk. All specimens were stained, and CD117, CD34, SMA, S-100 and desmin expression were 100%, 73.3%, 23.3%, 3.3%, and 3.3%, respectively (Table 2).
There was a significant association of recurrence with mitotic rate and tumor size. There was no significant association with tumor localization or recurrence. However, 5 patients with small bowel tumors experienced recurrence while 1 patient with a gastric tumor developed a recurrence. In the risk classification according to AFIP, recurrence rate increases proportionally to risk classification (Table 3).
Table 3: Relationship between tumor characteristics and mitotic rate and recurrence. View Table 3
The primary tumor was discovered during an indirect surgical procedure in 2 patients. In 9 subjects, gastroscopy was used to identify the tumor. In 19 cases, imaging studies were used to find the primary tumor: 4 by US, 14 by CT (Figure 1a), and one by MRI (Figure 2a).
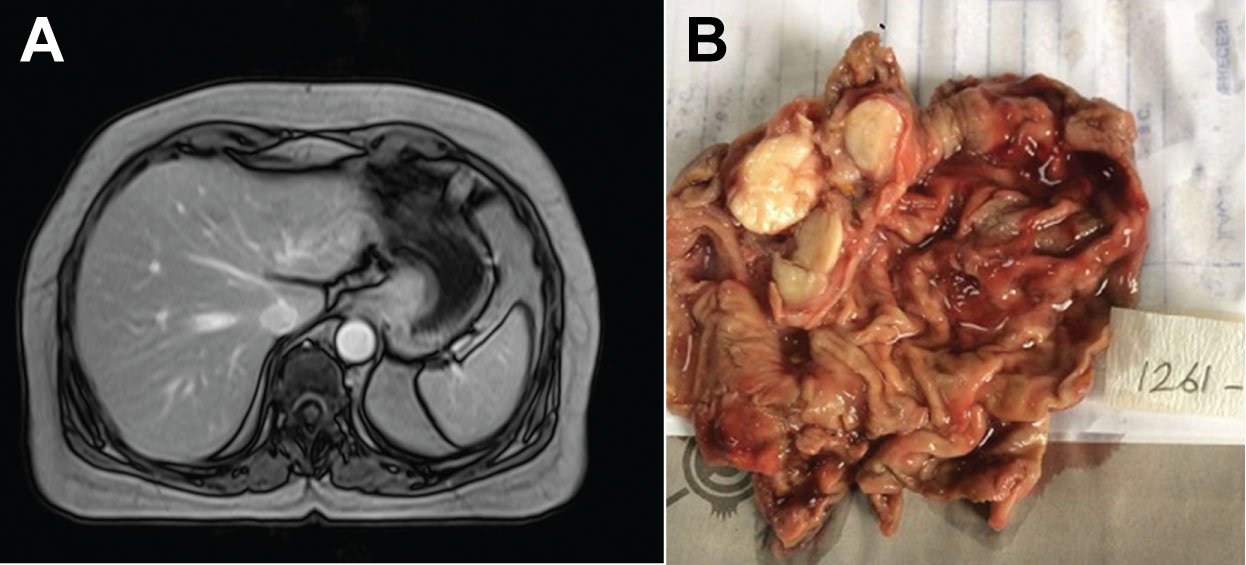 Figure 2: MR imaging a) and specimen of wedge resection b) of a GIST located at the esophageal-cardiac junction.
View Figure 2
Figure 2: MR imaging a) and specimen of wedge resection b) of a GIST located at the esophageal-cardiac junction.
View Figure 2
All tumors were treated surgically and were entirely resectable with R0 resection in 29 subjects and R1 resection in one subject. For these patients with GISTs, 8 had gastric wedge resection, 5 had distal subtotal gastrectomy and one had a total gastrectomy.
The operation was performed laparoscopically in 5 of the patients undergoing gastric wedge resection (Figure 2b). Thirteen patients had a segmental intestinal resection for GISTs localized to the duodenum/small intestine. The single subject with a rectal GIST had a low anterior resection.
Imatinib (400 mg/day) treatment was initiated postoperatively in 12 patients (7 intermediate risk patients and five high-risk patients).
During follow up, 24 subjects had no evidence of recurrence and 5 experienced a recurrence and one with metastasis. A patient with a 6 cm tumor and 60 mitoses per 50 HPF had a stomach wedge resection. Metastasis developed in the liver after 18 months. This patient underwent postoperative Imatinib treatment and died after 41 months. Primary tumor localization was the small intestine in the remaining five patients with recurrence. In this group, recurrence was either a local recurrence or peritoneal dissemination. These patients underwent surgical resection; however, macroscopic or microscopic residual tumors were left behind. These patients, for whom a complete surgical cure could not be achieved, continued to live with the disease. Postoperative Imatinib treatment was continued. Detailed data for these patients are given in Table 4.
Table 4: Treatment of patients with disease progression. View Table 4
Survival rates are shown in Table 4. With a median follow-up of 35.5 ± 12.9 months, the disease-free survival rate was 100%, 96%, 87%, and 68% at 1, 2, 3, and four years, respectively. Status for survival was as follows: alive, 29 (97%); free of disease, 24 (80%); alive with disease, 5 (17%); and death from disease, 1 (3%). The approximate time for patients to relapse was 47.8 ± 2.3 months (Figure 3).
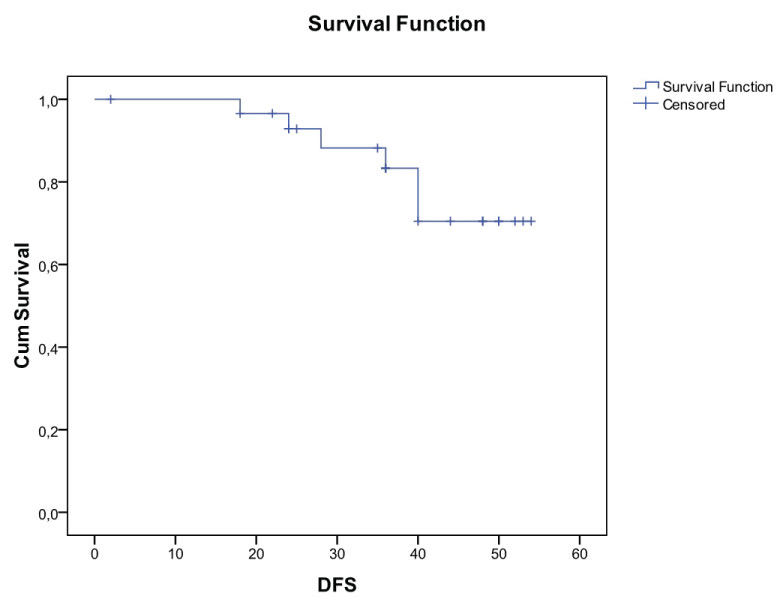 Figure 3: Overall survival.
View Figure 3
Figure 3: Overall survival.
View Figure 3
The relationship between the mitotic index and disease-free survival is shown in Figure 4. Statistically, the mitotic index increased and the disease-free survival decreased. The relationship between AFIP-Miettinen classification and disease-free survival is shown in Figure 5. According to the AFIP-Miettinen classification, the risk-free survival rate decreased as the risk of progression increased.
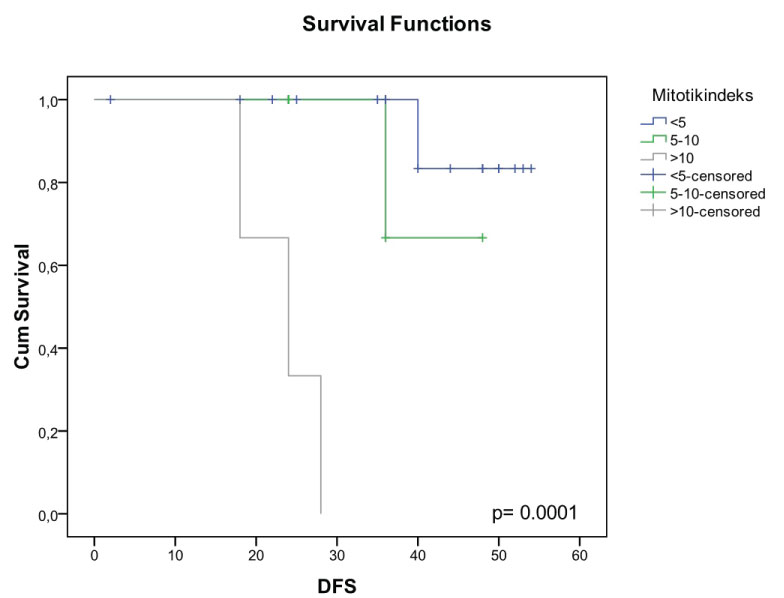 Figure 4: Relationship between the mitotic index and disease-free survival.
View Figure 4
Figure 4: Relationship between the mitotic index and disease-free survival.
View Figure 4
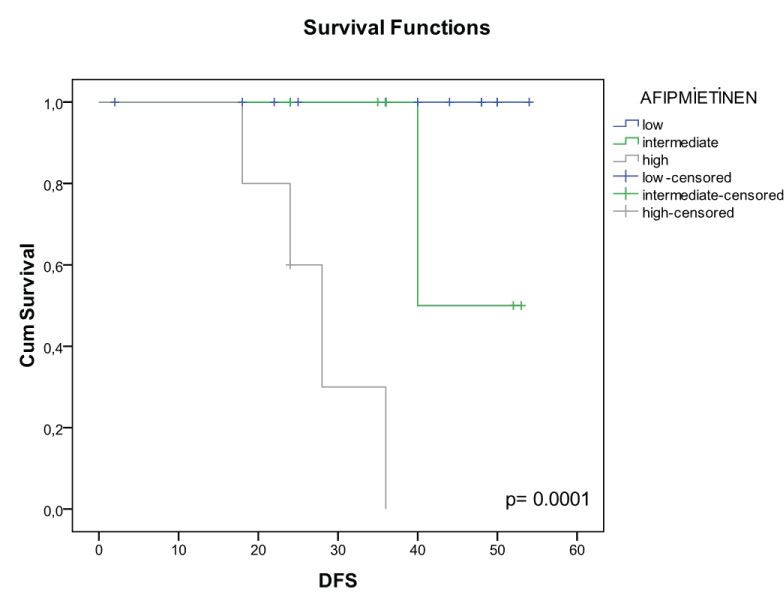 Figure 5: The relationship between AFIP-Miettinen classification and disease-free survival.
View Figure 5
Figure 5: The relationship between AFIP-Miettinen classification and disease-free survival.
View Figure 5
In this report, we retrospectively analyzed 30 patients with GISTs who were admitted to our clinic over the last ten years. We report that GIST occurred predominantly in elderly subjects with a median age of 63 years at diagnosis. This finding was consistent with those documented in previous studies [4,14]. A marginal male predominance was observed in this report.
In adult GISTs, the commons sites of localization have been documented [2]. In our study, GIST sites were stomach (46.7%), small intestine (43.3%), esophagus (6.7%), and rectum (3.3%), which is consistent with the previous literature.
GISTs present with a broad range of symptoms. In our study, gastrointestinal bleeding (36.6%), abdominal pain (23.3%), intestinal obstruction (13.3%), and asymptomatic (13.3%); likewise, the findings here are consistent with those from Miettinen, et al. [14].
Tumor size has a significant role in disease progression. In this report, the median tumor size was 7.0 cm (range 3-20 cm). According to the NCCN Task Force report, the most common size is approximately 5 cm.
Previous reports have shown that tumor location, tumor size, tumor rupture, and mitotic index are associated with GIST prognosis [2,4,5,8]. In our study, the mitotic index and tumor size were found to be statistically significant regarding prognosis. Tumor location, however, was not significantly associated with recurrence. In contrast, Miettinen, et al. [14] and Demetri, et al. [4] consider tumor location as the foundation for risk classification. The reasons for the lack of significance may be related to the limited number of subjects and data collection from a single center. The primary tumor site was the small intestine in 5 of 6 patients with recurrence in the stomach in 1 patient.
AFIP-Miettinen's criteria take into consideration the tumor anatomic site [8]. Gastric GISTs of 10 cm and 5 mitoses/50 HPFs are low metastasis risk. However, greater than 5 mitoses/50 HPFs and greater than 5 cm in diameter are higher risks. Conversely, all intestinal GISTs greater than 5 cm and all those greater than 5 mitoses/50 HPFs are placed at high risk for metastases [8,14,15]. Table 2 shows a comparison of all 30 subjects using the Miettinen scale. In our study, 60% of patients were at low risk, 23.3% were at intermediate risk, and 16.7% were in the high-risk category.
Presently, surgical resection is the gold standard for the treatment of localized GISTs. Laparoscopy has gained widespread acceptance for gastric stromal tumors that measure 5 cm or smaller [16-19].
According to the ESMO guidelines, adjuvant therapy with imatinib is a regimen for patients with significant relapse risk [4,20]. In our study, postoperative Imatinib therapy was administered to the majority of intermediate risk patients and all of the high-risk patients.
Long-term results have shown disease progression after discontinuing Imatinib [21,22]. In the present report, adjuvant imatinib therapy was continued for 1 to 3 years. Six subjects experienced abdominal recurrence after the regimen was discontinued (Table 4). Is a longer duration of adjuvant imatinib therapy more beneficial? Due to the retrospective study and a small patient cohort, we could not determine a definitive conclusion.
GIST recurrence is frequent, and one report documented only 10% of their subjects as disease-free post-long-term follow up [23]. Recurrence typically comprises the liver or peritoneal surface. In the 30 subjects that had the complete resection, liver involvement was found in one patient who suffered a recurrence. On the other hand, local recurrence developed in 3 subjects (10%), and peritoneal dissemination occurred in two subjects (6.7%).
For locally advanced inoperable and metastatic GISTs, imatinib is the recommended first-line treatment [4]. Regarding median survival, no difference was found at either the initial daily dose of 400 or 600 mg [24]. For progressive disease, imatinib treatment as a second-line therapy is controversial, even though doses of 800 mg daily are well-tolerated and have demonstrated a benefit to patients [25]. In our study, five patients had an abdominal recurrence and underwent a second surgery. However, the role of surgery during imatinib treatment, in advanced and metastatic disease is being investigated. Even though surgery has not been suggested as a first-line treatment option for advanced disease, existing evidence has shown that surgical resection in patients who respond to Imatinib has been beneficial [26].
In comparison to other intra-abdominal cancers, GIST patient survival following surgery alone has been favorable. One retrospective study indicated that the 5-year disease-specific survival rate for GIST patients following complete resection was 54%; conversely, when survival was predicted by tumor size, the survival rate was 35% [27]. Other studies have indicated that, following a complete resection, the 5-year patient survival rate was 40%-63% [28]. In our study, the 4-year disease-specific survival rate was 68%. The median time to recurrence following surgical intervention was 47 months (Figure 4). In one study [29], the median disease-specific survival of patients with metastatic GIST (N = 94) was 19 months. In our study, the disease-specific survival of patients with recurrence was also 19 months.
Mitotic index is the main variable used in the risk stratification systems first developed by the National Institute of Health [30]. In this system, more than 5 mitoses/50 HPF were associated with worse outcomes (Figure 4), which is similar to an analysis by Wong, et al. [31]. Consistent with the literature, our results confirm the importance of mitotic rate as an independent prognostic factor associated with disease-free survival.
In this report, disease-free survival was associated with the AFIP-Miettinen classification (Figure 5). According to the AFIP-Miettinen classification, the disease-free survival rate decreased as the risk or progression increased. Based on our findings, the classification system is useful for predicting disease-free survival rate following a localized GIST resection.
Collectively, our studies validate recent findings that GISTs most commonly occur in the stomach. In addition, a marginal male prevalence was found. Successful management of GISTs is complete surgical resection and adjuvant imatinib therapy for intermediate and high-risk patients. In this study, the mitotic index and tumor size were found to be statistically significant regarding prognosis. In some cases, GIST relapse was observed after termination of Imatinib treatment. It was thought that a longer duration of adjuvant treatment would be necessary and would benefit more. For recurrent and metastatic GISTs, targeted, personalized therapy is highly recommended, and consideration for further surgery should be based on individual need. Altogether, the combination of surgery with targeted, individualized treatment can improve overall patient survival.
Written approval was obtained from Cukurova University Faculty of Medicine Clinical Ethical Board.
Written informed consent was obtained from all patients and parents.
Not applicable.
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no competing interests.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
All authors have made substantial contributions to the conception and design of the study, acquisition of data, or analysis and interpretation; drafting the article or revising it critically for important intellectual content and final approval of the version to be submitted. MB performed the operations and interpreted the patient's data regarding gastrointestinal stromal tumor and YA analyzed and interpreted the patient data regarding gastrointestinal stromal tumor and was a major contributer in writing the manuscript. All authors read and approved the final manuscript.
American Journal Expert's extraordinary scientific proof reading and editing services were made.