Video-assisted thoracoscopic sympathetic surgery is currently a worldwide accepted treatment of primary upper extremity hyperhidrosis. Compensatory hyperhidrosis is the most common late complication and appeared to correlate with the extent and number of levels of sympathicotomy performed. In patients with combined severe palmar and axillary symptoms, the surgeon must decide whether to divide the chain at multiple levels by combining what is done for palmar and axillary symptoms alone (T2-T3-T4) or simply choose which of the two operations to perform based on which symptom predominates.
Between December 2012 and October 2015, 103 patients with severe combined palmar, axillary and plantar hyperhidrosis underwent to thoracoscopic T2-T3 sympathicotomy.
Target resolution of the disorder in long term follow-up was achieved in 100% (hands), 97.08% (axilla), and 58.25% (foot-through unknown mechanism) of the patients. Long term reduction in plantar sweating was 29.12% and in axillary sweating was 2.9%. Mild to moderate compensatory sweating occurred in 10 patients (9.7%). The long term recurrence rate was 2.9% (axilla), 17.8% (foot) and 0% (hands). The recurrence in axilla and foot was in the form of mild dry. Overall satisfaction rate was 99.02%.
In conclusion, our results suggest that T2-T3 video-assisted thoracoscopic sympathicotomy is a safe and effective procedure for treatment of combined palmar, axillary and plantar hyperhidrosis.
Hyperhidrosis, Sympathicotomy, Thoracoscopic
Primary hyperhydrosis is a disorder characterized by excessive perspiration beyond thermoregulatory needs, particulary in response to temperature or emotional stimuli [1,2]. Various treatment options are available, including topical and systemic therapies, iontophoresis, regional nerve block and botulinum toxin injection. However, each has its own limitations [3]. Video-assisted thoracoscopic sympathetic surgery is currently a world wide accepted treatment of primary upper extremity hyperhidrosis [4]. Thoracoscopic sympathicotomy should be regarded as the current standard surgical technique for the treatment of primary hyperhidrosis [5]. The primary goal of sympathetic nerve surgery for primary hyperhidrosis is the relief of the hyperhidrosis. Secondary goals are to perform the procedures while minimizing complications, recurrence, and hospital and convalescent times. Ideally, minimizing the incidence of compensatory sweating, a well-known side effect of sympathetic nerve surgery, is highly desirable and is spurring investigations to improve these procedures [5]. It was postulated that lowering the level of ablation and reducing its extent would attenuate the amount of compensatory hyperhidrosis [6]. In patients with combined severe palmar and axillary symptoms, the surgeon must decide whether to divide the chain at multiple levels by combining what is done for palmar and axillary symptoms alone (T2-T3-T4) or simply choose which of the two operations to perform based on which symptom predominates [5]. This paper is aimed to show the results obtained with T2-T3 sympathicotomy in treatment of combined palmar, axillary and plantar hyperhidrosis.
Between December 2012 and October 2015, 103 patients with severe combined palmar, axillary and plantar hyperhidrosis underwent to thoracoscopic T2-T3 sympathicotomy (Table 1). Patients with isolated palmar, plantar or axillary hyperhidrosis have been excluded from the study.
Table 1: Clinical characteristics of patients. View Table 1
All patients had excessive sweating in hands ,armpits and foots, severely interfering with their work or social activities. Before surgery, all patients underwent a careful clinical history, pre-operative routine blood examination, spirometry and chest X-ray to exclude pulmonary disease. Informed consent was obtained from all patients after explantation of the nature of the disease, possible treatment, complications and side effects. Patients evaluation was conducted at the time of discharge and after 6, 12 and 24 months. The postoperative follow-up was 24 months. Patients were evaluated according to the results of sweating, compensatory hyperhidrosis, degree of satisfaction, complications, and recurrence. The results of the intervention were evaluated by patients as follows: "Dry" when the patient was not aware of sweat on the palms, axilla or foot, "nearly dry" when the patient had marked improvement whereby minimal sweat sometimes occurred under stressful conditions and "wet when the patient had limited improvement and was very aware of sweating. Compensatory sweating in other regions of the body was graded as "mild" when it was tolerable but sometimes interfered with daily activities, "moderate" when it was barely tolerable and frequently interfered with daily activities and "severe" when it was intolerable and always interfered with daily activities.
The degree of satisfaction for each patient was evaluated as very satisfied, satisfied and partially satisfied. Patient satisfaction was evaluated using an analogous scale ranging from 1 to 10 with 1 indicating no satisfaction at all and 10, the maximum possible satisfaction. We further divided the analogous scale in 4 parts: Not satisfied (1), partially satisfied (2-4), satisfied (5-7), and very satisfied (8-10). Recurrence was considered when the affected body part had become hyperhidrotic again after it had been rendered dry after surgery.
Surgery was performed under general anesthesia. Double lumen endotracheal intubation and selective one lung ventilation was used. Patients were placed on the operating table in a modified semi-Fowlers position. In this positioning, the patient's back is almost 45 degrees up from horizontal and both arms are abducted 90 degrees while resting and secured to arm boards. Both left and right axillary and chest skin areas are topically prepped and draped at the beginning of the operation in anticipation of bilateral sequential thoracoscopic surgery. A 5 mm trochar was inserted at the anterior axillary line, 2nd intercostal space, in order to introduce the endoscopic dissector, and a second trochar of 5 mm in the anterior axillary line, fourth intercostal space, for the thoracoscope. Once thoracoscopic ports are placed, the lung falls away from the posteriorly located sympathetic chain. We use the hook cautery to open the pleura overlying the sympathetic chain and carefully dissect the chain free from surrounding tissues at the level of division prior to its division. The main sympathetic chain is then divided as it overlies both the second and third ribs. To further prevent reattachment of the chain by natural healing, we carefully distract the two ends away from each other and tuck them under their respective pleural coverings. The bodies of ribs 2 and 3 are then scored horizontally with the cautery from the costovertebral angle laterally for 2 to 3 cm to ablate any accessory fibers of Kuntz. The thoracoscop and endoscopic instruments were then removed. The port incision at the anterior axillary line, 2nd intercostal space, was closed. A temporary pediatric-size chest tube was inserted into the thoracic cavity through the trochar incision (anterior axillary line, fourth intercostal space) and connected to a water seal system applying a mild suction. After re-inflating the lungs, the chest tube was quickly removed and the incision was closed. The same procedure was performed on the opposite side after operation on one side is ended. At the end of surgery a postoperative chest X-ray was routinely taken to rule out pneumothorax or hemothorax.
A total of 103 patients underwent video assisted thoracoscopic sympathicotomies. From this patients, 58 were female (56.3%) and 45 were men (43.6%), with a mean age of 31.6 years (ranging from 20-43 years) (Table 1). All patients had an immediate result after surgery, having warm and dry hands and dry armpits. Plantar hyperhidrosis was improved immediate after surgery in 70.87% (73/103) and reduction in plantar sweating was occurred in 16.5% (17/103) (Immediate after surgery, total response in plantar hyperhidrosis was 87.37%). The postoperative follow-up period was 2 years. No operative mortality, morbidity or conversion to open surgery was recorded. Complications such as pneumothorax, hemothorax and horner's syndrome were not observed. The effectiveness (Figure 1) at the time of discharge, 6 months, 12 months and 24 months was, respectively: 100%, 100%, 100% and 100% (palmar hyperhidrosis), 100%, 100%, 99.02% and 97.08% (Axillary hyperhidrosis), 70.87%, 64.57%, 62.13% and 58.25% (Plantar hyperhidrosis). Recurrence occurred in hands 0%, axilla 2.9% (3 patients) and foot 17.8% (13 patients). Compensatory sweating occurred in 10 patients (9.7%) between 6 and 12 month. It was classified as None, in 93 cases (90.3%), Mild in 8 cases (7.7%), and Moderate in 2 cases (1.94%). The most frequent locations were back, abdomen and groins. The degree of overall satisfaction was 99.02% (Table 2).
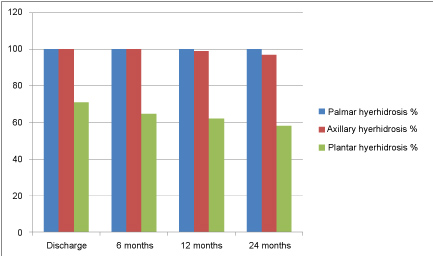 Figure 1: Effectiveness of the thoracoscopic sympathicotomy.
View Figure 1
Figure 1: Effectiveness of the thoracoscopic sympathicotomy.
View Figure 1
Table 2: Surgical outcomes after 2 years. View Table 2
The evolution of modern minimally invasive thoracic surgery in the last two decades has rendered thoracoscopic sympathetic nerve surgery an attractive and highly effective surgical treatment option for patients afflicted with the medical malady known as primary hyperhidrosis. As experience with minimally invasive surgery has grown, these operations have become the most effective treatment for this medical problem in patients who have failed to benefit from nonsurgical treatments [5]. Thoracoscopic sympathectomy involves resection of a segment of the thoracic sympathetic nerve chain, but this is now an operation of historical interest, as equivalent or improved results are readily achieved with operations such as thoracoscopic sympathicotomy or sympathetic nerve clamping. In thoracoscopic sympathicotomy, the sympathetic nerve chain is surgically divided and the intervening nerve segment is either left in situ or cauterized. This operation yields excellent improvement of hyperhidrosis as compared with sympathectomy, but with significantly less surgical dissection and concomitant tissue trauma. Thoracoscopic sympathicotomy should be regarded as the current standard surgical technique for the treatment of primary hyperhidrosis [5]. Compensatory hyperhidrosis (postoperative increase of sweating in regions of the body where it had not been previously observed) is the most common late complication, with different incidence reported in previous studies, ranging from 33% to 85% [7,8]. The mechanism of compensatory sweating is unclear, but it is unlikely to represent a normal thermoregulatory compensation, as not all patients experience this side effect after surgery. Kwong and colleagues reported that compensatory sweating appeared to correlate with the extent and number of levels of sympathicotomy performed [9]. Compensatory sweating is greater with T2-T4 resection than with T2 or T3 only or T2-T3 resection [10]. The published results do not provide a consensus regarding the most favorable technique, although treatment of axillary hyperhidrosis requires resection as far as T4 [11]. In patients with combined severe palmar and axillary symptoms, the surgeon must decide whether to divide the chain at multiple levels by combining what is done for palmar and axillary symptoms alone or simply choose which of the two operations to perform based on which symptom predominates. Still the debate is ongoing about which levels and how many levels of sympathectomy ensure the highest success rate and carry the lowest incidence of compensatory hyperhidrosis [12]. Up to 69% of patients with hyperhidrosis of the upper extremities also suffer from plantar hyperhidrosis, and this modification cannot be explained by conventional anatomy [13]. The improvement of plantar hyperhidrosis is 50% at 6 months postoperative and decreases to 23.4% at 12 months as a consequence of recurrence [13]. In this report, we showed that T2-T3 video-assisted thoracoscopic sympathicotomy for combined palmar, axillary and plantar hyperhidrosis are successful procedures with minimal invasiveness and few postoperative complications. In our series, target resolution of the disorder in long term follow-up was achieved in 100% (hands), 97.08% (axilla), and 58.25% (foot-through unknown mechanism) of the patients. Long term reduction in plantar sweating was 29.12% and in axillary sweating was 2.9%. Mild to moderate compensatory sweating occurred in 10 patients (9.7%). The long term recurrence rate was 2.9% (axilla), 17.8% (foot) and 0% (hands). The recurrence in axilla and foot was in the form of mild dry. Overall satisfaction rate was 99.02%.
In conclusion, our results suggest that T2-T3 video-assisted thoracoscopic sympathicotomy is a safe and effective procedure for treatment of combined palmar, axillary and plantar hyperhidrosis.
Reza Ershadi and other co-authors have not conflict of interest.