Controversy exists regarding the role of laparoscopic peritoneal lavage in patients with perforated diverticulitis. Our objective was to conduct the first meta-analysis of Randomized Controlled Trials (RCT's) to compare the outcomes of patient undergoing laparoscopic peritoneal lavage with sigmoidectomy in patients with perforated diverticulitis.
In accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement standards, we conducted a systematic search of electronic information sources, including MEDLINE; EMBASE; CINAHL; CENTRAL; The World Health Organization International Clinical Trials Registry; ClinicalTrials.gov; ISRCTN Register and bibliographic reference lists. We applied a combination of free text and controlled vocabulary search adapted to thesaurus headings, search operators and limits in each of the above databases. Overall morbidity, mortality, and postoperative complications were defined as the primary outcome parameters. Procedure time and length of hospital stay were secondary outcomes. The combined overall effect sizes were calculated using fixed-effect or random-effects models.
We identified 4 RCT's comparing outcomes of laparoscopic peritoneal lavage and open sigmoidectomy for perforated diverticulitis. All studies included only Hinchey grade III diverticulitis. The subsequent analysis, including 390 patients, demonstrated that laparoscopic peritoneal lavage of perforated diverticulitis was associated with significantly increased rates of overall morbidity (OR: 1.30, 95% CI 1.07-1.57, p = 0.007) and intra-abdominal abscess (OR: 3.10, 95% CI 1.71-5.63, p = 0.0002) compared to sigmoidectomy. However, there was no significant difference in mortality (OR: 0.86, 95% CI 0.42-1.77, p = 0.69) and re-operation (OR: 1.20, 95% CI 0.36-4.02, p = 0.77) rates between the two groups. Between-study heterogeneity was non-significant in all analyses, except reoperation rate (I2 = 79%, p = 0.002). The available data did not allow an appropriate analysis of procedure time, length of hospital stay and other postoperative complications.
Our analysis of randomised trials demonstrated that laparoscopic peritoneal lavage of perforated diverticulitis may lead to more adverse events than open sigmoid resection. Future high quality RCT's are indeed required to provide stronger evidence as no definitive conclusion can be drawn considering the limited number of available RCT's.
Laparoscopy, Peritoneal lavage, Diverticular perforation, Peritonitis
Diverticular disease is a common colonic pathology in western world. The incidence increases with age to reach 34% to 56% of persons older than 70 years [1,2]. In the presence of diverticulosis, 15% to 25% also develop diverticulitis. This can be divided into uncomplicated and complicated disease in which complicated diverticulitis may require surgical intervention [3-5]. Despite its increased prevalence, only about 10% of acute diverticulitis cases require surgical intervention [1,2].
Hinchey, et al. [6] for the first time classified perforated diverticulitis into 4 grades: I) Walled of pericolic abscess; II) Walled off pelvic abscess; III) Purulent contamination of peritoneal space, and IV) Free faecal contamination of peritoneal space. This classification has been extensively applied in the routine clinical practice. With the advent of cross sectional imaging, it is now possible to grade patients in accordance with Hinchey classification without any operative intervention.
For both Hinchey III and IV in the sigmoid colon, the Hartmann's procedure has historically been considered the standard of surgical management (known as two-stage procedure) in patients with perforated acute diverticulitis with generalised peritonitis [2]. It has an associated mortality of 15.1% and leaves up to 70% of patients with permanent stomas [3,4]. On the other hand, in acutely perforated diverticular disease, primary resection and anastomosis with or without de-functioning stoma has a mortality rate of 10% and anastomotic leak rate of 14% [3]. Hence the choice of surgical approach remains controversial [4,5].
The use of laparoscopic peritoneal lavage for management of perforated diverticulitis was first reported by O'Sullivan, et al. [7]. All eight patients in their series made full recovery. Since then, few more small case series have been reported but no definitive conclusions were derived [8,9]. The peritoneal lavage results in the reduction of endotoxin levels in the peritoneal cavity by promoting drainage of blood, bacteria, faecal material, fibrin, purulent exudates and devitalised tissue. It reduces the septic load, improves haemodynamic stability and decreases the risk of multiorgan failure [10]. The intraperitoneal lavage is described as safe, easy to perform and not associated with significant complications [11]. The American Society of Colon and Rectal Surgeons categorically stated that there is no clear consensus on the use of laparoscopic lavage in the management of peritonitis from acutely perforated diverticular disease [12].
We aimed to a comprehensive systemic review of the literature and the fist meta-analysis of the related outcomes to compare outcomes of laparoscopic peritoneal lavage with sigmoidectomy in patients with perforated diverticulitis.
We pre-specified the inclusion criteria, methods, and outcomes of our study in a review protocol. The study was carried out in line with Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement standards.
We selected all RCTs comparing the outcomes of laparoscopic peritoneal lavage and sigmoidectomy in patients with diverticular perforation. All patients with diverticular peritonitis, either Hinchey III (purulent peritonitis) or Hinchey IV (faecal peritonitis), in the descending colon and/or sigmoid colon were included.
Perioperative mortality, overall morbidity and complications were defined as the primary outcome parameters. Procedure time and length of hospital stay were secondary outcome measures.
Literature search strategy: Two independent authors (Shahin H and Shahab H) searched the following electronic databases: MEDLINE, EMBASE, CINAHL and Cochrane Central Register of Controlled Trials (CENTRAL). The last search was run on 28 December 2016. In addition, the following trial databases were searched for ongoing and unpublished studies: World Health Organization International Clinical Trials Registry http://apps.who.int/trialsearch/, ClinicalTrials.gov http://clinicaltrials.gov/, and ISRCTN Register http://www.isrctn.com/. We applied a combination of free text and controlled vocabulary search adapted to thesaurus headings, search operators and limits in each of the above databases. Moreover, we searched the reference lists of relevant articles and reviews for further eligible trials.
Data collection: Computerised data spreadsheet was created for data extraction in line with the Cochrane's data collection form for intervention reviews. We pilot-tested the spreadsheet in randomly selected articles and adjusted it accordingly. Our data extraction spreadsheet included the following information:
• Study-related data
• Baseline demographic and clinical information of the study populations
• Primary and secondary outcome data
Two authors (Shahin H and AM) independently collected and recorded data in the data extraction spreadsheet. Disagreements were resolved by discussion. If no agreement could be reached, a third author (Shahab H) was consulted.
Selection of studies: Two authors (Shahin H and AM) independently assessed the title and abstract of articles identified through literature searches. The full-texts of relevant reports were assessed and those articles that met the inclusion criteria of our study were selected. We resolved discrepancies in study selection by discussion between the authors. An independent third author (Shahab H) was consulted in the event of disagreement.
Assessment of risk of bias: The methodological quality and risk of bias of the included articles were assessed independently by two authors (AP and Shahab H). We used the Cochrane's tool ref for assessing the risk of bias of randomised. The Cochrane's tool assesses the following domains: Selection bias, performance bias, detection bias, attrition bias, reporting bias, and other sources of bias and, for each individual domain, classifies studies into low, unclear, or high risk of bias. We resolved disagreements by discussion between the two assessing authors. If no agreement could be reached, a third reviewer (Shahin H) acted as an adjudicator.
Summary measures and synthesis: For dichotomous outcome variables we calculated the risk difference Odds Ratio (OR) as the summary measures. The OR is the odds of an adverse event in the laparoscopic peritoneal lavage group compared to the sigmoidectomy group. An OR of less than one would favour the laparoscopic peritoneal lavage group compared to the sigmoidectomy group. For continuous parameters we calculated the Mean Difference (MD) between the laparoscopy and laparotomy groups.
We used the individual patient as the unit of analysis. We recorded information about dropouts, withdrawals and other missing data and, if not reported, we contacted the study authors. The final analysis was based on intention-to-treat data from the individual clinical studies where possible.
We used the Review Manager 5.3 software for data synthesis [7]. The extracted data were entered into Review Manager by the first independent author (Shahin H) and checked by a second independent author (Shahab H). We used random-effects or fixed-effect modelling, as appropriate, for analysis. We applied random-effects models if considerable heterogeneity among the studies, as defined by Higgins, et al. [7], was identified. The results were reported in a forest plot with 95% Confidence Intervals (CIs).
Heterogeneity among the studies was assessed using the Cochran Q test (χ2). We quantified inconsistency by calculating I2 and interpreted it using the following guide: 0% to 25% might not be important; 25% to 75%: May represent moderate heterogeneity; 75% to 100% may represent substantial heterogeneity. We planned to use the Comprehensive Meta-Analysis (CMA) software (Biostat, Englewood, NJ) to calculate the Egger's regression intercept to formally assess reporting bias in our review. Also, we planned to construct funnel plots and evaluate their symmetry to visually assess publication bias, as long as a sufficient number of studies (more than 10) were available.
Additional analyses were planned to explore potential sources of heterogeneity and assess the robustness of our results. For each outcome, we repeated the primary analysis using random-effects or fixed-effect models. In addition, we calculated the pooled OR, Risk Ratio (RR), or Risk Difference (RD) for each dichotomous variable. We assessed the effect of each study on the overall effect size and heterogeneity by repeating the analysis after removing one study at a time.
The searches identified 154 articles (Figure 1) Following reviewing the titles and abstracts, which was followed by assessing the full text, we identified 4 RCT reporting a total of 390 patients of whom 202 patients underwent laparoscopic peritoneal lavage and the remaining 188 patients had open sigmoidectomy for perforated diverticulitis. All of the included the studies included patients with Hinchey grade III diverticular perforation.
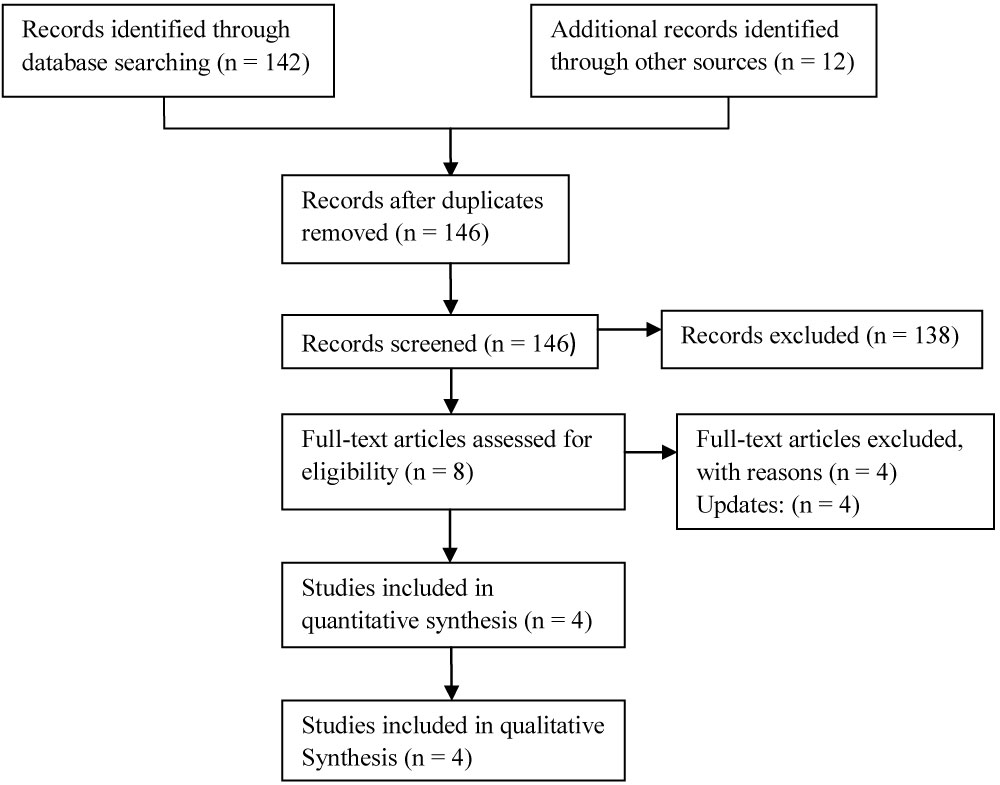 Figure 1: Study flow diagram.
View Figure 1
Figure 1: Study flow diagram.
View Figure 1
Figure 2 presents the risk of bias assessment of the included RCTs. There were low risk of attrition and reporting bias in all 4 RCTs. Selection bias were low in 3 studies and unclear in 1 studies. Performance bias were high and unclear in 3 and 1 studies, respectively.
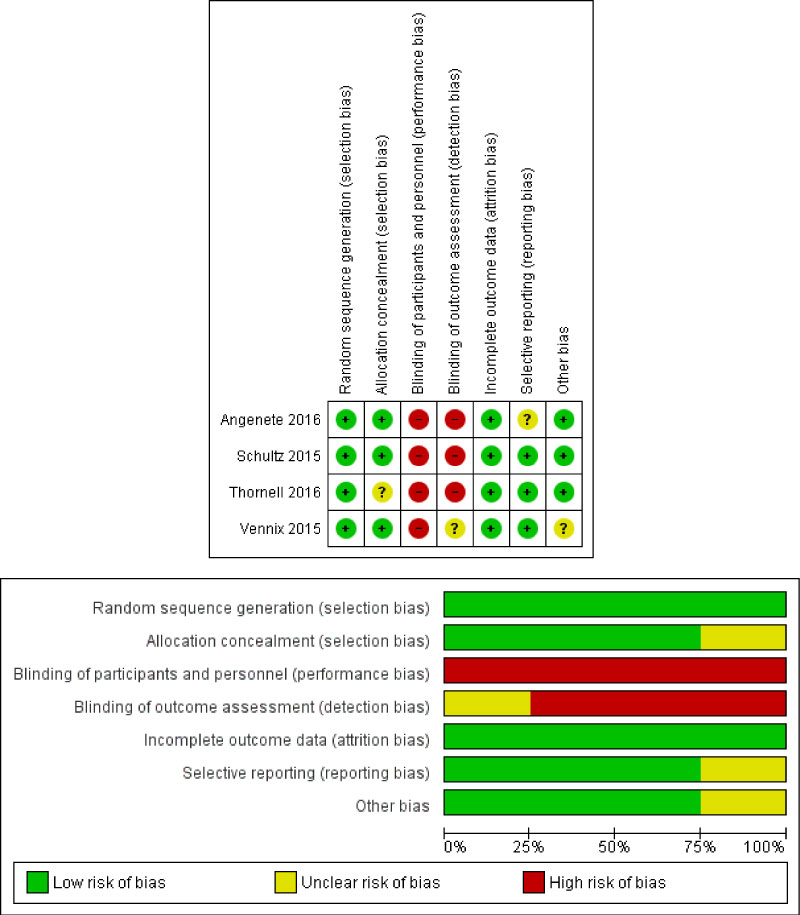 Figure 2: Risk of bias summary and graph showing authors' judgments about each risk of bias item.
View Figure 2
Figure 2: Risk of bias summary and graph showing authors' judgments about each risk of bias item.
View Figure 2
Laparoscopic peritoneal lavage versus sigmoidectomy: Outcomes are summarised in Figure 3.
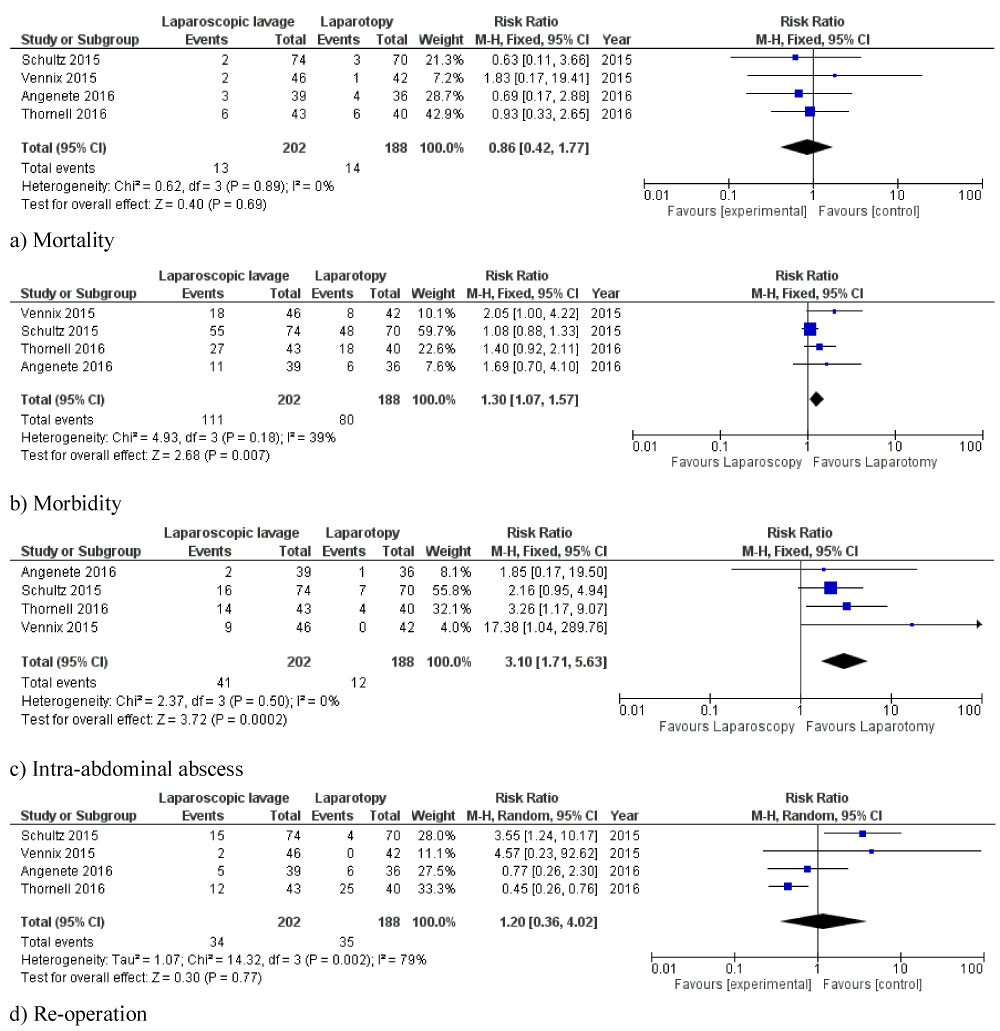 Figure 3: Forest plots of comparison of a) Mortality; b) Overall morbidity; c) Intra-abdominal abscess, and d) Re-operation. The solid squares denote the Risk Difference (RD), Risk Ratios (RRs), or Mean Difference (MD). The horizontal lines represent the 95% Confidence Intervals (CIs), and the diamond denotes the pooled effect size. M-H, Mantel Haenszel test.
View Figure 3
Figure 3: Forest plots of comparison of a) Mortality; b) Overall morbidity; c) Intra-abdominal abscess, and d) Re-operation. The solid squares denote the Risk Difference (RD), Risk Ratios (RRs), or Mean Difference (MD). The horizontal lines represent the 95% Confidence Intervals (CIs), and the diamond denotes the pooled effect size. M-H, Mantel Haenszel test.
View Figure 3
Mortality: All included studies reported mortality as an outcome. There were 13 (6.4%) and 14 (7.4%) perioperative deaths in the LPL and sigmoidectomy groups, respectively. The pooled analysis of 390 patients did not find any significant difference in mortality between both groups (OR: 0.86, 95% CI 0.42-1.77, p = 0.69). Between-study heterogeneity was low (I2 = 0%, p = 0.89).
Morbidity: All included RCTs reported overall morbidity as an outcome. In the laparoscopic peritoneal lavage group, 111 (54.9%) patients were considered to have significant perioperative morbidity whereas 80 (42.5%) patients in the sigmoidectomy group had significant morbidity. Our pooled analysis of 390 patients demonstrated that laparoscopic peritoneal lavage significantly increased overall perioperative morbidity compared to sigmoidectomy (RR: 1.30, 95% CI 1.07-1.57, p = 0.007). There was moderate between-study heterogeneity (I2 = 39%, p = 0.18).
Intra-abdominal abscess: All 4 studies (390 patients) reported intra-abdominal abscess as an outcome parameter. There were 41 (20.2%) events in laparoscopic lavage group and 12 (6.3%) events in the sigmoidectomy group. Laparoscopic peritoneal lavage was associated with a significantly higher rate of intra-abdominal abscess formation compared to sigmoidectomy (OR: 3.10, 95% CI 1.71-5.63, p = 0.0002). Heterogeneity among the included studies was not significant. (I2 = 0%, p = 0.50).
Re-operation: All studies reported re-operation rate as an outcome. There were 34 (16.8%) and 35 (18.6%) re-operations in the laparoscopic peritoneal lavage and sigmoidectomy groups, respectively. The pooled analysis of 390 patients did not find any significant difference in re-operation rate between the two groups (OR: 1.20, 95% CI 0.36-4.02, p = 0.77). There was significant heterogeneity among the included studies (I2 = 79%, p = 0.002).
The available data did not allow an appropriate analysis of procedure time, length of hospital stay and other postoperative complications.
Sensitivity analysis: Using random-effects or fixed-effect models did not affect the pooled effect size in any of the outcomes. The direction of pooled effect size remained unchanged when the OR, RR, or RD was calculated. Moreover, removal of on study at a time did not change the direction of pooled effect size in the analysis of any of the outcomes.
The management of complicated acute diverticulitis has continued to evolve over the last one century. During the early part of the 20th century a three stage procedure involving defunctioning colostomy, colonic resection and finally reversal of stoma was adopted [13]. Mikulicz, et al. promoted immediate laparotomy and peritoneal wash out for peritonitis resulting from perforated diverticular disease [14]. When these studies were compared to emergency Hartmann's procedure outcome it was identified that Hartmann's procedure can reduce mortality by 25% [15]. Rehn, et al. reported first series of patients with improved outcome undergoing peritoneal lavage. The observed mortality was reduced by 38% following saline irrigation of peritoneal cavity in patients undergoing laparotomy with faecal peritonitis [8].
In the last two decades with advancement in laparoscopic surgery the minimal invasive approach has progressed to include perforated diverticular disease. A less invasive approach of Laparoscopic Peritoneal Lavage (LPL) has been advocated. It involves standard pre-operative resuscitation, creation of pneumoperitoneum, irrigation with normal saline, aspiration of exudates, fibrinous material and siting of pelvic drains.
Since 2010 multiple randomised controlled trails have been conducted incorporating laparoscopic lavage as a management option for patients diagnosed with perforated diverticulitis. Angenete, et al. provided positive evidence supporting laparoscopic lavage for perforated diverticulitis to be feasible and safe and concluded favourable outcome for peritoneal lavage in patients with perforated diverticular disease [16]. Thornell, et al. concluded laparoscopic lavage to be better then laparotomy for management of patients with Hinchey III diverticular perforation as well [17]. Sheikh, et al. in their meta-analysis concluded laparoscopic lavage to be safe and quick alternative to sigmoidectomy for acutely perforated diverticular patients [18]. A recent literature review by Cirocchi, et al. also favoured laparoscopic lavage as a definitive treatment in 25% of cases [10].
Vennix, et al. in their RCT concluded no superiority of laparoscopy when compared to sigmoid resection for purulent perforated diverticulitis [19]. SCANDIV (Scandinavian Diverticulitis Trial) randomised controlled trial by Schultz and colleagues recently concluded no reduction in severe postoperative complications in laparoscopic lavage against primary resection [20].
Other techniques of use of fibrin glue for perforated diverticulitis has been described but has not been widely adopted [8]. Advent of CT guided drainage combined with broad spectrum antibiotics has established role in care of patients with localised perforation forming a walled off collection with no generalised peritonitis [18]. European Association for Endoscopic Surgery currently recommends LPL in a select group of patients in specialised units [21]. At present peritoneal lavage is not a recommendation for faecal peritonitis and Hartmann's procedure is the treatment of choice in such situations.
In view of existence of controversy regarding the role of laparoscopic peritoneal lavage in patients with perforated diverticulitis, we conducted a comprehensive systemic review of the literature and meta-analysis of the related outcomes. We identified 4 RCTs reporting a total of 390 patients with Hinchey grade III diverticular perforation of whom 202 patients underwent laparoscopic peritoneal lavage and the remaining 188 patients had open sigmoidectomy. Our subsequent analysis demonstrated that laparoscopic peritoneal lavage of perforated diverticulitis was associated with significantly increased rates of overall morbidity and intra-abdominal abscess compared to sigmoidectomy. However, it did not significantly increase mortality and reoperation rates. The between-study heterogeneity was not significant in the analysis of mortality, overall morbidity and intra-abdominal abscess which suggests that our findings regarding these outcomes may be robust. Moreover, the results of our sensitivity analysis was consistent with our main analysis.
Toorenvliet, et al. [22] systematically reviewed 13 series including 231 patients and reported a success rate of 96% associated with laparoscopic lavage with low mortality (2%) and morbidity (10%). In this context, Myers, et al. [23] conducted the largest series including 92 patients and reported 95% success rate associated with laparoscopic peritoneal lavage and suggested laparoscopic lavage as a definitive treatment of purulent peritonitis. However, it should be considered that these studies included a large number of patients without perforation (Hinchey II) which, undoubtedly, subjects their outcomes to bias. More recent case series demonstrated higher failure rates of up to 34% and a morbidity rates of up to 56% associated with laparoscopic lavage [24,25].
Our study has some limitations. Only 4 RCTs, the gold standard study design for comparative studies, was identified to provide high quality evidence for or against laparoscopic peritoneal lavage or sigmoidectomy. The available evidence comes mainly from a limited number of RCTs with small sample sizes. Moreover, the included studies did not provide appropriate data for analysis of some of the defined secondary outcome parameters. Finally, the performance bias was high in 3 studies and unclear in one.
Our analysis of all available RCTs demonstrated that laparoscopic peritoneal lavage of perforated diverticulitis may increase the risk of overall morbidities and perioperative complications than open sigmoid resection. However, it may not increase mortality and the need for re-intervention. The available evidence comes from a limited number of RCTs with small sample sizes that are subject to performance bias. Future high quality RCT's are indeed required to provide stronger evidence as no definitive conclusion can be drawn considering the limited number of available RCT's.
We do not have commercial interest and no connection with any commercial entity, which can directly or indirectly influence the findings from this study.
All author(s) has agreed for publication of this article and has contributed equally towards research, study design and preparation of this article.
The author(s) received no funding with respect to research, authorship and publication of this article.