Translocation of microbial materials into the circulation via hepatic vein can cause sepsis and deterioration in patient's condition [1]. In clinical setting, this phenomenon may be associated with a fistulous communication between hepatic-abscess and hepatic vein, which is termed "hepato-venous fistula (HVF)" by Chung, et al. [2]. We report a case of postoperative HVF diagnosed radiologically, treated surgically, and confirmed histologically.
A 72-year-old man, who had been received hemodialysis for chronic kidney disease, underwent resection of hepatic bed and hepatocholedochus with satellite lymphadenectomy for incidentally identified gallbladder carcinoma after laparoscopic cholecystectomy. He developed spike fever on postoperative day (POD) 10. Computed tomography (CT) showed small fluid collection around the resection surface of liver (Figure 1). Percutaneous drainage was performed and a little fluid with serous appearance was gotten. Several sessions of percutaneous drainage brought temporary remissions but, after de-clamping or removal of drainage tube, exacerbation occurred in each time. Three months after the second surgery, contrast injection study revealed an opacification of the middle hepatic vein (MHV) (Figure 2). Immediately after the study, the patient developed chill and rigor indicating a presence of a fistulous communication between the fluid-containing cavity and MHV, and occurrence of dissemination of bacterial materials into the circulation. To treat that fistula, it is thought that liver resection including impaired MHV and parenchyma suspected of microbial fouling was necessary and that impaired perfusion area should not be left. Liver resection of the segment V was performed. During the resection of liver parenchyma, MHV with thickened and white colored wall was encircled (Figure 3a) and dissected at proximal side after definite ligation. Histopathological examination showed hepatic vein surrounded by inflammatory cells and disruption of venous wall (Figure 3b). The postoperative course was uneventful.
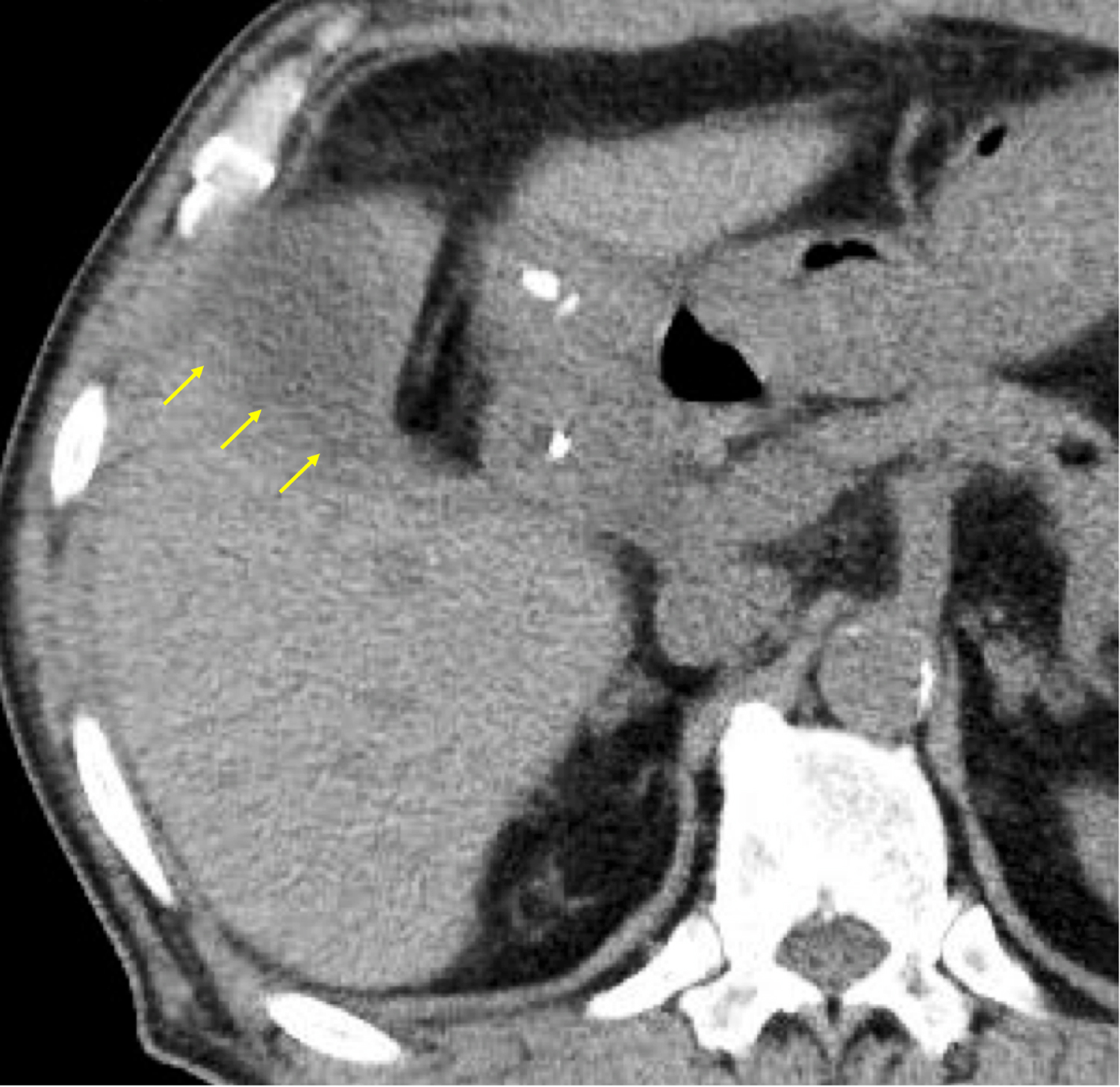 Figure 1: Computed tomography (CT) revealed a low density area around the resection surface (arrow).
View Figure 1
Figure 1: Computed tomography (CT) revealed a low density area around the resection surface (arrow).
View Figure 1
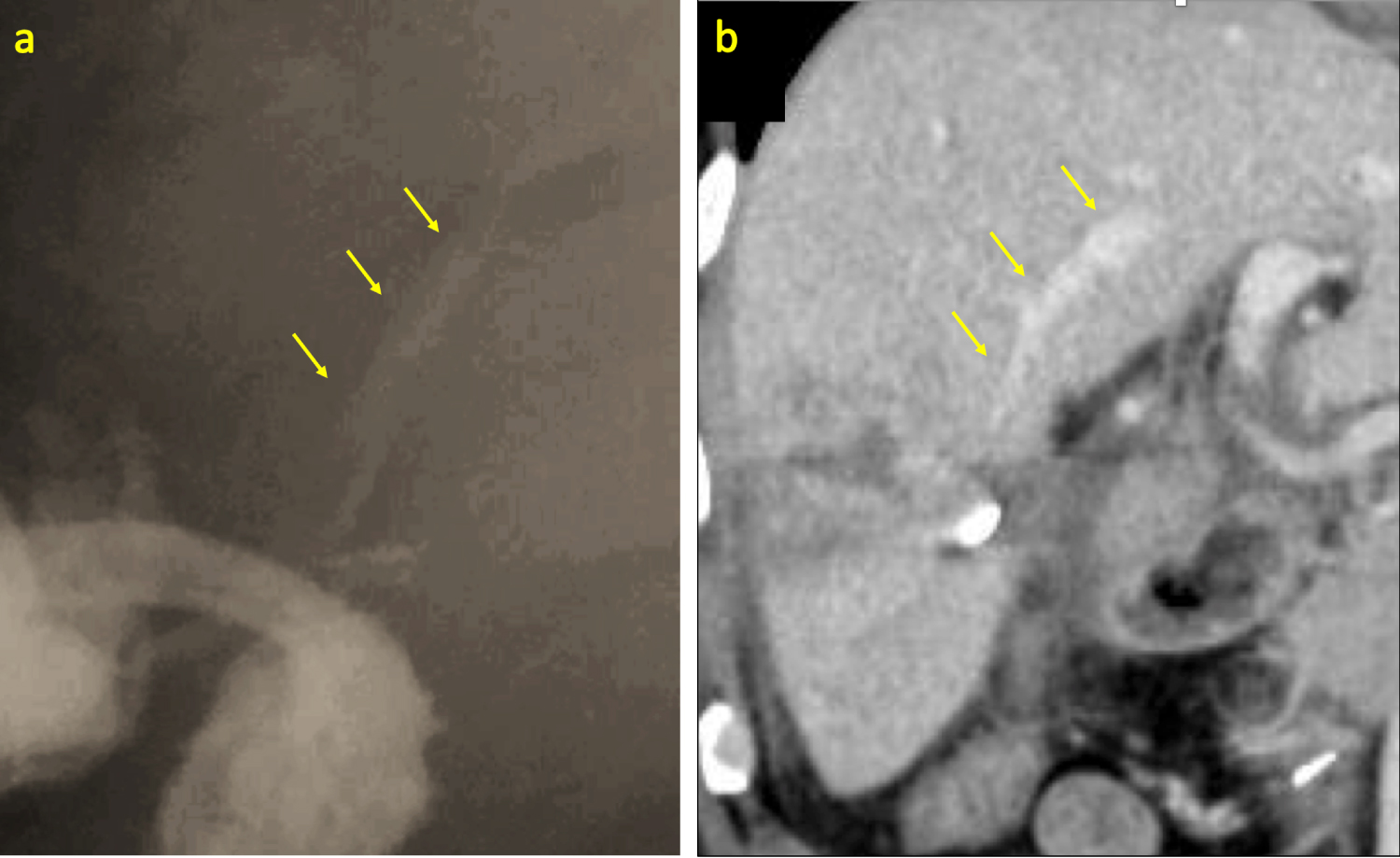 Figure 2: a) Contrast study showed opacification of the Middle hepatic vein (MHV) (arrow); b) A contrast coronal CT image showed MHV running through the marginal area of the fluid collection (arrow).
View Figure 2
Figure 2: a) Contrast study showed opacification of the Middle hepatic vein (MHV) (arrow); b) A contrast coronal CT image showed MHV running through the marginal area of the fluid collection (arrow).
View Figure 2
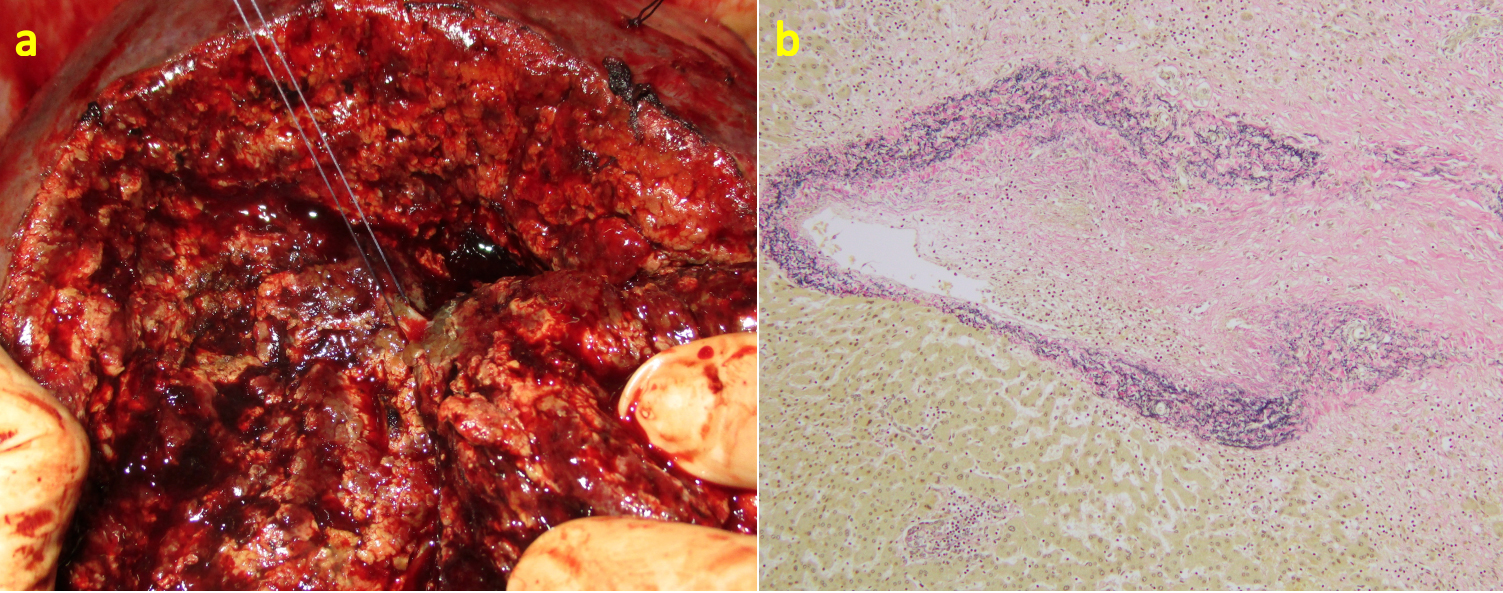 Figure 3: a) Intraoperative; and b) Pathological findings. a) During the resection of liver parenchyma, MHV with thickened and white colored wall was encircled. Histological examination of resected specimen revealed disruption of hepatic vein wall (Elastin van Gieson stain).
View Figure 3
Figure 3: a) Intraoperative; and b) Pathological findings. a) During the resection of liver parenchyma, MHV with thickened and white colored wall was encircled. Histological examination of resected specimen revealed disruption of hepatic vein wall (Elastin van Gieson stain).
View Figure 3
Percutaneous abscess drainage can be followed by bacteremia presumably due to venous backflow of bacterial materials into the circulation. The communications between the abscess cavity and veins are small and are usually not demonstrated on abscessography. Therefore, reports of images which show fistulous communication between liver abscesses and hepatic veins documented on such study are scarce [2]. In the present case, the volumes of drainage, including the one from intraoperative drain, were small (less than 20 mL/day). It was thought that when fluid accumulation, even if it is small amount, increased the pressure within the cavity and precipitated the fistulous communication, he developed spike fever due to bacteremia. Formation of protracted fistula between resection surface and hepatic vein after liver surgery are very rare. In this case, it is supposed that our patient's condition undergoing chronic dialysis might have contributed to adhesion-resistance and infection [3], and we cannot deny the possibility that handling of vessels during liver resection was insecure which might have facilitated formation of fistula. Embolization by endovascular approach is a treatment option for intrahepatic fistula [4], on the other hand, placement of foreign material at the suspected contaminated area should be avoided. Hepatectomy is a good therapeutic option for HVF when percutaneous drainage or other less-invasive approach fails, as indicated in previous reports about pyogenic hepatic abscess [5,6]. Familiarity with HVF and a high index of this rare condition are required. Hepatectomy is the treatment of choice, especially when it is intractable.
T. Iwasaki transferred from Kindai University to National Defense Medical College in April 2019.