Breast conservative surgery (BCS) and oncoplastic procedures are becoming more and more popular, providing better aesthetic outcome but one of the main draw-back of these procedures is involvement of the margin and return to theatre, causing undesired economic and cosmetic outcome in addition to psychological burden on the patients. Frozen section can decrease incidence of involved margin however, it is not always available in addition to increasing the cost. Using Intra-operative ultrasound (IOUS) is a proposed solution to overcome this dilemma.
In this systematic review, publication between 2001 and 2019 assessing the use of intra-operative US for margin clearance were identified in MEDLINE EMBASE CINAHL AMED and the Cochrane library, with the primary outcome looking into margin involvement and return to theatre and secondary outcome as cosmetic outcome, and the volume of removed breast tissue. 7 papers were identified for this systematic review.
These papers were critically appraised using PRISMA guideline, with main focus on margin involvement, and also looking into the volume of specimen removed.
Intra-operative ultrasound can decrease return to theatre and improve surgical margin as well as cosmetic outcome and patient satisfaction. On the other hand, ultrasound overestimated the pathology margins in most cases. Margin overestimation by ultrasound may lead the surgeon to incorrectly believe that the excised margins are inappropriate. The overestimation of the majority of the tumour margins may be explained in part by the tendency of ultrasound to underestimate the pathologic tumour diameter.
Because of routine screening mammography and increased public awareness, breast cancer is increasingly detected at an earlier stage. For women with operable breast cancer, surgical resection options are breast conservation surgery (lumpectomy) and mastectomy. For many women in whom lumpectomy is feasible, a breast conservation approach is the preferred option [1].
One of the primary goals of breast-conserving surgery is to obtain cancer free margin. Margins positive or focally positive for tumor cells are associated with a high risk of local recurrence, and in the case of tumor positive margins, re-excision or even mastectomy are sometimes needed to achieve definite clear margins. For focally positive margins, either second surgery or additional boost radiotherapy should be considered.
Re-excision surgery of the tumor bed has a negative impact on cosmesis. This is mainly as a consequence of the increased total volume of tissue excised from the breast. There is no limit to the number of re-excisions that a patient can have to achieve complete removal of all invasive and in situ disease, but with the greater number of re-excisions more tissue is removed and so the likelihood of a good cosmetic result decreases. Intra-operative frozen section can be used as a planning strategy for the surgeon as to which direction requires a greater excision margin for safety by using the pathologist's report. However, the hospital has to employ the pathologist, the result is also at the discretion of the pathologist, and this step can add approximately 20-30 minutes to the operating time. Additionally, and perhaps most significantly, some authors have concluded that IFSA may not be reliable for the detection of Ductal carcinoma in situ (DCIS).
Various imaging modalities have been used to locate and stage tumors before surgery and to locate and remove tumors and masses during surgery. Ultrasound has particularly lent itself to both preoperative and intraoperative use. US guidance gives the advantage of resecting less normal tissue while maintaining the clear margins with both palpable and non-palpable masses [2]. It has been shown to be feasible and, in some series, even superior to the gold standard technique of needle localization.
Intraoperative ultrasound guided surgery (IOUS) has extensively shown to be a more effective tool compared to Wire localization (WL) and Palpation-guided surgery (PGS) [3,4]. It also improves rates of negative margins, consequently reducing the need of second surgeries [5-7]. In addition, The COBALT study showed a significant reduction in the volume excised when using IOUS as compared to PGS (38 cm3 vs. 57 cm3, p = 0.002) [8].
The structured question for this review was as follows (Table 1).
Table 1: The structured question for review. View Table 1
Publications through electronic databases including (MEDLINE EMBASE CINAHL AMED and The Cochrane library) were searched without time limit till 2019 using Boolean operators ''AND'' and ''OR' to run the search.
The extracted articles were organized. Duplicate articles were deleted, and then 2 reviewers assessed the titles and abstracts of search results independently and selected potentially-relevant studies according to the main question (Table 1). The articles that were deemed to be irrelevant to the research objectives were excluded. Then, the full texts of the selected articles were gathered.
Both prospective and retrospective studies were included studies in English were searched for and studies in other languages was excluded. Main inclusion criteria for this study was: a) Female patient undergoing breast conservative surgery (include Wide local excision (WLE) and level 1 oncoplastic procedure; b) Female patient with level 2 oncoplastic surgery; c) Ductal carcinoma in situ (DCIS) and Invasive cancer.
Main exclusion criteria were: a) Patients undergoing modified radicle mastectomy; b) Male patients as the standard procedure is mastectomy not breast conserving surgeries.
Primary outcomes:
1. To assess margin positivity rates in patients undergoing breast conservation surgery by intra-operative ultrasound guidance method.
2. Local recurrence rate.
3. Return to theatre for involved margins.
Secondary outcomes: Included
1. Cosmetic outcome and quality of life in patients undergoing breast conservation surgery using intra‐operative ultrasound guidance method.
2. Volume of removed breast tissue.
The articles selected for the review will be individually assessed for their external and internal validity. Two review authors will independently critically appraise the internal validity and external validity of the included studies. This will be assessed according to the criteria of Critical appraisal tools from the Cochrane Collaboration and the Critical appraisal skills program (CASP) for RCT and Non-RCT. Another qualitative method of assessing data that will be used for Randomised controlled trials is (Jadad scoring system) [9]. The Newcastle-ottawa scale (NOS) will be used to assess the observational studies.
A standardized excell data extraction form was prepared and used to extract data from the included papers. Data on the population, study characteristics and results will then be extracted independently by two review authors. Any disagreement will be discussed, and a third review author consulted if disagreements persist.
Based on the exclusion criteria and removal of duplicated results 37 studies were included after first selection. All articles were subsequently selected on title, abstract, and full text. Out of these 37 studies 7 publications met the eligible inclusion criteria for the study. The total number (first and second selection) Identification, screening, eligibility, and inclusion details all are shown in PRISMA flow chart (Figure 1).
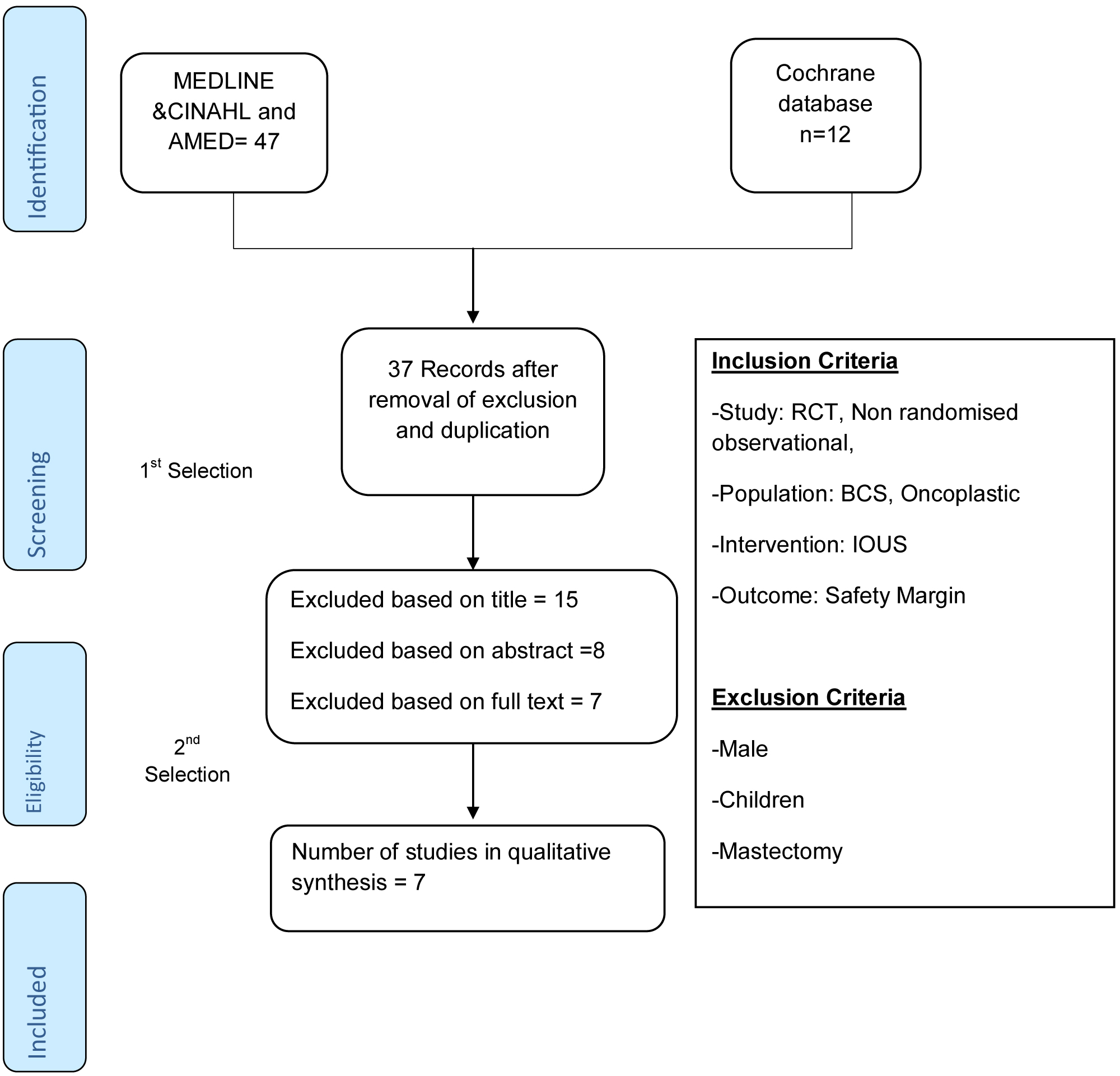 Figure 1: Prisma flowchart.
View Figure 1
Figure 1: Prisma flowchart.
View Figure 1
The need for second surgery was mentioned in all 7 studies. Four studies, Esqueva, Moore, Ramos, et al. and Karnalik, et al. showed that IOUS can reduce need for second surgery [10]. However, Moore, et al. included patients with DCIS in his study which may have resulted in his conclusion of superiority of US. Ramos, et al. and Karnalik, et al. showed that IOUS can improve surgical margin but their results can be attributed to the fact that US underestimate clear margin and result in removing excess breast tissues. Only Esqueva, et al. RCT showed that IOUS is efficient method in detecting clear margin without underestimation of the clear margin. The COBALT trial and Larson, et al. and Fisher, et al. findings were that IOUS does not improve surgical margin when compared to control group [11].
The total number of patients included in all 7 studies was 1166 number of those, patients who had intra-operative ultrasound was 711 patients. The number of the pooled patients is significantly higher than any individual study individual which is one of the major advantages when performing systematic review.
All seven studies mentioned the rate of safety margin involvement after performing breast conservative surgery, all the studies used ultrasound as an intra-operative radiological method in determining margin involvement, one study used additional radiological tool beside US in assessing the margin which was mammogram.
Volume of breast tissue removed was reported in studies. Cosmetic outcome and patient satisfaction were assessed in 3 papers. Volders, et al. assessed quality of life using EORTC-QLQ-C30 and the breast cancer module QLQ-BR23 questionnaire. Operative time was mentioned in 2 studies only. Doyle, et al. assessed the use of High frequency ultrasound in assessment of margin using 50 MHz transducers and results from high-frequency ultrasonic measurements of human breast tissue specimens indicate that characteristics in the ultrasonic attenuation, spectra, and cepstra can be used to differentiate between normal, benign, and malignant breast pathologies. Another aspect of development is usage of 3D Ultrasound, use of this system has the potential to reduce the number of re-excision surgeries that these patients undergo which delays their systemic chemotherapy with potentially negative long-term outcomes.
Definition of and evaluation of surgical margins is essential for oncological sound treatment of breast cancer. IOUS seems to improve the rate of clear margins and reduce re-excision rate for invasive disease. Larson, et al. had slightly different results as in his study he used mammogram as well as US. On the other hand, other methods for assessment of margin were compared in 6 studies. And margin clearance varied between 70% and 84%. There were 675 patients of all 711 patients in these studies who had clear margin representing 94.9%. Clear margin definition was variable between different studies, Esgueva, et al. definition was: (close (≤ 2 mm) or positive margins) and this is considered involved margin and warrant re-excision. This was also used by Fisher, et al. [11], for Larson, et al. tumour on ink is considered involved margin for invasive cancer and for Ductal carcinoma in situ (DCIS) < 2 mm from margin is involved margin. Moore, et al. had similar principle a positive margin was defined as any margin where tumour cells were microscopically visible on final histopathologic evaluation. For Ramos, et al. positive margin if the margin 3 mm close to the tumour. Volders, et al. defined clear margin in their study as "no tumour cells at the margin" however, they aimed to remove at least 1 mm of healthy tissue on all margins. Karanlik, et al. reported positive margin if involved or less than 5 mm from tumour margin. As mentioned, the concept of clear margin was variable between authors in different studies from tumour on ink to 5 mm, and till now there is controversy on definition of safety margin for invasive breast cancer, despite most surgeon agree that no tumor cell at margin is sufficient for a clear margin this cannot be generalised. This variability in margin definition in each study can alter the results and the outcomes as well, in another word, one patient could have described as having involved margin in one study and that same patient can have clear margin in another study and avoid second surgery.
Another difference in these studies was the ultrasound machine and US probe used to assess intra-operative margin. Moore, et al. used 7.5 -mHz linear-array ultrasound while Karanlik, et al. multi frequency 10 -MHz linear array ultrasound probe. The US machine used by Ramos, et al. was 6-12 MHz high-frequency linear array transducer (Falcon Ultrasound Scanner, B-K Medical Systems, MA 01960, USA). Volders, et al. used a 14 MHz ultrasonography probe (Toshiba Viamo, Tokyo, Japan). Esqueva, et al. used Esaote MyLab25Gold (Genova, Italy). And Fisher, et al. Sonosite Micromax device (Bothell, WA) but both did not mention the probe size. Larson, et al. mentioned that L- shaped probe was used with no further details.
The implication of using variable US machines and probes may result in different outcomes, as the sensitivity of each probe is different, and interpretation of the sonographic findings based on each machine. Another fact that should be considered is the experience of the US operator and his experience as US is operator dependent and results may vary between different individual.
Another point to take in consideration is the time gap between these studies as first study included in the review was done 2001 while the last study was published in 2019, during these 18 years the advancement and the technology behind US could have affected the outcome with relatively more advanced US equipment (Table 2).
Table 2: Definition of and evaluation of surgical margins is essential for oncological sound treatment of breast cancer. View Table 2
Less patients had further excision in IOUS group across all studies. However, percentage of patients having second surgery was variable among different studies, Ramos, et al. had only 3 out of 225 cases that had second surgery representing 1.3% that was the lowest second surgery rate among the chosen studies. Volders, et al. had similar results with second surgery rate about 2%, Moore, et al. had 3.5% second surgery rate. Esgueva, et al. and Karanlik, et al. second surgery rate of 5.4% and 6% respectively. The remaining 2 studies had over 10% second surgery Larson, et al. had 10% and Fisher, et al. was the highest 23%. Second surgery rate was insignificant from other methods of assessment of intra-operative margin in all studies apart from Moore, et al. Patients who had subsequent mastectomy were mentioned in 3 studies with a total number of 17 patients having mastectomy 6 patients had mastectomy after using US and the other 11 when using other methods. IOUS as a tool for assessment of intraoperative margin can result in decreasing second surgery for involved margin, however at the moment there is no statistical difference between using ultrasound and other conventional methods, but this can be related to the small sample size of these studies. Reducing the number of second surgery due to margin involvement can result in improved cosmetic outcome and patient satisfaction. In addition, it has financial implication by reducing the cost of second operation and decreasing overall hospital stay (Table 3).
Table 3: Second surgery. View Table 3
IOUS would improve cosmesis by enabling the surgeon to position the incision on the breast optimally and minimize the resection of normal breast parenchyma.
Volders, Esqueva, et al. and Fisher, et al. showed that there is statistically significant reduction in the removed breast volume when using intra-operative US compared to other methods. Despite Moore, et al. and Karanlik, et al. showed that using US reduced amount of breast volume that was statistically non-significant. This is another benefit of using US in assessment of margin, as it resulted in decreasing amount of the breast volume removed. There is also evidence that the cosmetic result depends on the volume of breast excised and the number of reoperations performed. 3 studies commented on cosmetic outcome and patient satisfaction 2 of those studies showed no noticeable difference in cosmetic outcome and patient satisfaction when comparing IOUS guided resection with palpation guided resection. Moore, et al. and Karanlik, et al. had non-significant difference for removed breast tissue using IOUS and PGE and hence there was no significant difference in cosmetic outcome, However, for Volders, et al. in the COBALT trial volume of breast tissue removed was significantly less in US group compared to PGE group and Cosmetic self-evaluation at 3 years when comparing 2 groups was significant wit a P value < 0.001. This is consistent with the fact that the more breast tissue removed the worse cosmetic outcome.
This is another advantage for using US to assess margin during surgery where it was noted that there is less breast tissue removed when using ultrasound and consequently better cosmetic outcome. However, 2 studies did not show any superiority in cosmetic outcome for IOUS group. This can be explained by using oncoplastic technique which is aesthetically appealing despite removing excess tissues. Another explanation is that cosmetic outcome was not affected by removing excess tissue is that patients had larger breast volume, hence the excess tissue removed will have trivial effect in cosmetic outcome as the percentage of removed breast tissue is the determinant not the exact volume, and this was not addressed in any of the studies.
The quality of the studies included in this systematic review was relatively poor 2 of the RCT scored one on Jadad score and the other scored 2 this score does not reflect the actual quality of the involved studies as it is technically difficult to design a double blinded study in surgery, which attributed to the low score. Other studies scored relatively better on Newcastle Ottawa Score two studies scored 5 and one study scored one and another scored 4, this numerical guide is helpful in assessment of the quality of each individual study and the main strength and weakness of each study and how to improve it in the future for example, follow up of the patients was not done in 3 of these studies and it would have markedly improved their score and quality if included in the study design.
There are few limitations in this systematic review.
First, there was no uniformity in definition of positive margin in different studies; each study had its own definition of clear margin. Second, the limited number of RCT and variability of study design means that performing metanalysis was not feasible.
US is a safe and cheap tool that can be used to help surgeon in assessing intra-operative margin large RCT's need and metanalysis need to be designed to show the efficacy of US as a modern technique for reducing margin involvement. From the studies that has been involved in this systematic review there is no strong evidence to recommend using routine US to assess intraoperative margin form the 7 studies involved in the systematic review only 3 were RCT's and they were of poor quality by Jadad score one study scoring 2 and the other two scored 1 . Four of these studies showed IOUS superiority in assessing safety margin and three showed similar results to control group. Well-designed RCT's can help in proper evaluation of IOUS taking in consideration unified definition of clear margin. There is still a room for development for this technique with development in the industry of ultrasound machine, Another benefit of using this system will be the improved aim of the surgeon's resection directly to the tumour area, minimizing the unintended resection of large amounts of normal breast tissue, which has a large impact on the postoperative cosmetic appearance of the breast.
On the basis of this systematic review it is clear that Intra-operative ultrasound can decrease return to theatre and improve surgical margin as well as cosmetic outcome and patient satisfaction. On the other hand, ultrasound overestimated the pathology margins in most cases. Margin overestimation by ultrasound may lead the surgeon to incorrectly believe that the excised margins are inappropriate. The overestimation of the majority of the tumour margins may be explained in part by the tendency of ultrasound to underestimate the pathologic tumor diameter [12]. Another possible factor that needs to be taken into account as a cause for overestimation of tumor margins by ultrasound is the compression of the specimen by the ultrasound probe during ex vivo examination of the margins [10].