The COVID-19 pandemic had resulted in major disruptions in healthcare globally. As a response to the outbreak, global elective surgeries were suspended to preserve resources. To date, Malaysia's effectiveness in tackling the COVID-19 was an instructive example for many East Asia countries. In addition to the public health preparedness, we report our experience in early restructuring of elective breast and endocrine cancer surgery to ensure a continuum in cancer care during the peak of the pandemic.
Elective surgery, Breast and endocrine cancer, COVID-19 pandemic, Malaysia
On March 11, 2020, the World Health Organization (WHO) officially declared the novel Coronavirus Disease (COVID-19) pandemic as an international emergency. This disease that began in Hubei Province, China in late December 2019 had since infected more than 5 million individuals globally and approximately 7000 individuals in Malaysia, at the time of drafting this editorial. In response to the pandemic crisis, the federal government of Malaysia had implemented a Movement Control Order (MCO) since 18 March 2020 as a strategy to flatten the curve and to slow the virus spread [1]. The Ministry of Health (MOH) Malaysia had promptly identified 35 designated hospitals to manage suspected/confirmed COVID-19 cases across the states [2]. Government hospitals were categorized into screening hospitals and treating hospitals respectively, leaving few being non-COVID-19 hospitals. In the effort to minimize the risks of exposure among patients and to preserve resources in anticipation of an overwhelming surge in COVID-19 cases, MOH issued directives to temporary suspend all elective surgeries starting from 24 March 2020 [3]. This had created a difficult dilemma to both healthcare professionals and patients; especially in those focused on the treatment of cancer. The inherent risks of delaying cancer surgery would inadvertently affect its long term outcome while cancer treatment during this period could lead to an increased risk of infection. Therefore, it is important for the surgeon to balance the risks between potential viral transmission and possible cancer progression [4]. To mitigate such negative impact, a collaborative effort was made to restructure elective breast and endocrine cancer surgery from Hospital Putrajaya (a designated screening COVID-19 hospital) to the nearest non-COVID-19 hospital, the National Cancer Institute. The sole objective was to deliver a safe and high quality care in continuum of oncology surgical services for breast and endocrine cancer patients, amidst an evolving pandemic situation.
A systematic algorithm (Figure 1) was drafted prospectively with adaptation from international recommendations [5,6] by a group of consultant surgeons, anaesthetists, microbiologists/pathologists as well as hospital administrative stakeholders. Six key components of the restructuring are: Triage & prioritization, clinical health screening, pre-operative COVID-19 testing for all patients, in-patient pre-anaesthetic assessment, intraoperative preparation, post-operative home care with symptoms surveillance. A special task force was formed to coordinate the entire process; ensuring a smooth and safe transition of patients care from one hospital to another (Table 1, Table 2 and Table 3).
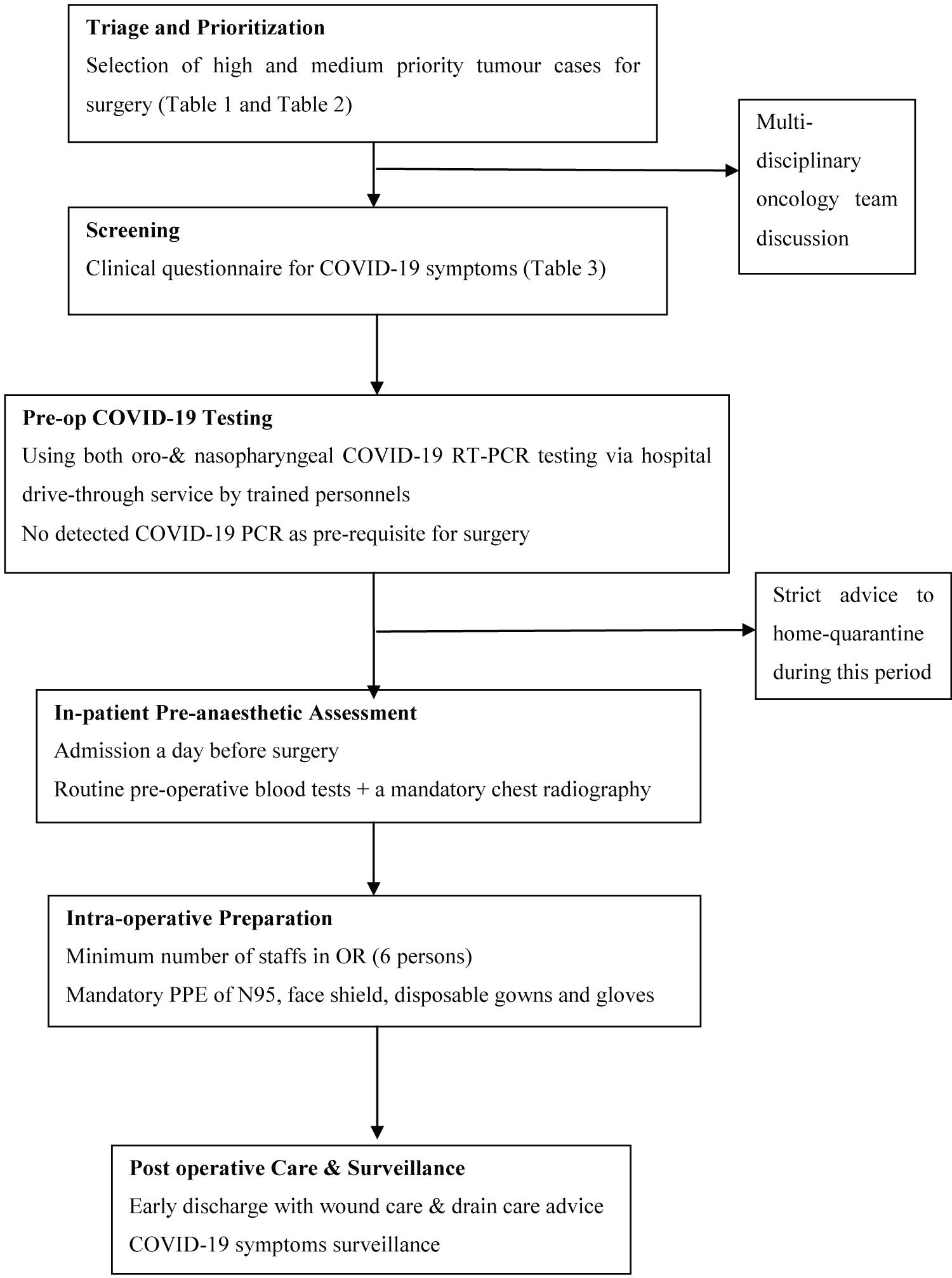 Figure 1: A systematic approach on restructuring breast and endocrine elective cancer surgery from Hospital Putrajaya to National Cancer Institute during COVID-19 pandemic.
View Figure 1
Figure 1: A systematic approach on restructuring breast and endocrine elective cancer surgery from Hospital Putrajaya to National Cancer Institute during COVID-19 pandemic.
View Figure 1
Table 1: Triage & Prioritization of breast tumour cases for surgery tailored to local case-mix (adapted from ACS [11], ESMO [12]) (ACS-American College of Surgeons, ESMO-European Society of Medical Oncology). View Table 1
Table 2: Triage & Prioritisation of endocrine tumour cases tailored to local case-mix (adapted from ACS). View Table 2
Table 3: Screening questionnaires adapted from Health Declaration Form, Ministry of Health Malaysia. View Table 3
A total number of 85 elective breast and endocrine surgeries that were scheduled from 24 March 2020 onwards were subjected to cancellation or postponement following MOH directives. With the implementation of this systematic approach to shift elective surgery to a non-COVID-19 hospital, we successfully performed 34 out of 85 cases (40.0%) during our country's peak pandemic crisis from 30 March 2020 to 22 May 2020 (8 weeks) (Table 4). Only cases of high to medium priority were selected for surgery. All patients had passed their preliminary clinical health screening questionnaires for COVID-19 symptoms via telecommunications, prior to the diagnostic COVID-19 swabs tests. Similarly, all patients were confirmed negative for COVID-19 PCR prior to surgeries. Neither patients nor health care workers developed COVID-19 symptoms/disease throughout this period of hospital admission and surgery.
Table 4: Type of surgery and total number of cases successfully performed electively. View Table 4
Hospital Putrajaya is one of the three highest volume tertiary breast and endocrine centre in Malaysia. Statistically, our hospital manages approximately 600 elective breast and endocrine surgeries annually; averaging 12 cases per week. The impact of elective surgery cancellation would undoubtedly add to a growing backlog that needs to be addressed once the pandemic is over. The CovidSurg Collaborative Researchers from Birmingham recently estimated 28.4 million elective surgeries will be cancelled or postponed worldwide during the peak 12 weeks disruption due to COVID-19. This data was then statistically modelled to estimate totals for cancelled surgery across 190 countries; generating an overall 12-week cancellation rate to be 72.3% with 2.3 million cases (37.7%) being cancer surgery. If countries increase their normal surgical volume by 20% post-pandemic, it would take a median of 45 weeks (11 months) to clear the backlog of operations resulting from COVID-19 disruption [7]. Using a similar iQueue Elective Surgery Backlog Recovery Calculator [8], it estimated 8.8 months were required to clear the backlog if all our cases (n = 85) were postponed. Following this early restructuring, we were able to reduce our backlog and time- predicted to recover to 5.1 months (Figure 2a and Figure 2b). Thus, cancellation rate was reduced to 60%. However, resuming elective cancer surgery was not without its risks. As cancer patients were considered as high risk individuals, it is crucial to provide them adequate information regarding potential serious adverse events that could occur during an elective surgery. Evidence was scarce and largely retrospective then; Shaoqing, et al. [9] studied 34 patients that have surgery during the incubation of COVID-19 infection which carried a mortality rate of 20.5%. But his report was limited by the small number of representation of only five cancer cases and all patients had prior direct exposure to Wuhan City. Liang, et al. [10] with the largest prospective cohort COVID-19 patients (n = 1571), reported that cancer is associated with an increased risk of death and/or intensive care unit admission in COVID-19 disease (odds-ratio of 5.4, 95% CI 1.8-16.2). But due to the small number of 18 cancer cases in his study, it did not establish a definitive correlation of increase in incidence of cancer with COVID-19 infection. By far, we had no COVID-19 infection in our 34 cancer patients that underwent surgery.
 Figure 2: (a,b) Estimating total time taken to recover from backlog of cases using iQueue elective surgery backlog recovery calculator between 49 cases vs. 85 cases (5.1 months vs. 8.8 months).
View Figure 2
Figure 2: (a,b) Estimating total time taken to recover from backlog of cases using iQueue elective surgery backlog recovery calculator between 49 cases vs. 85 cases (5.1 months vs. 8.8 months).
View Figure 2
Two samples of nasopharygeal and oropharyngeal swabs were performed in each patient prior to surgery. The Abbott Realtime SARS-COV-2 assays that were used have 100% sensitivity. Our patients were subjected to a screening test five days prior to surgery following which they were strictly self-quarantined in line with the MCO. A negative result was a pre-requisite to undergo elective surgery under general anaesthesia. A positive result would bar the patient from surgery and treatment as per COVID-19 patient. Surgery would then be carried out following clearance of two negative swabs post-treatment. All surgeries were performed under general anaesthesia in full Personal Protective Equipment (PPE) with biohazard measures implemented. Intubations were performed with ‘intubation box' following which patients and machines were covered with plastic sheets to reduce droplet spread. Restricting number of staffs to only six personnel (i.e. one surgeon, one assistant surgeon, one anaesthetist, one anaesthetist medical officer, one scrub nurse and one circulating nurse) to minimise exposure to staffs. Post-operatively, patients were discharged as early as day one if feasible. Home surveillance by daily telecommunication as well as to follow up on any development of COVID-19 symptoms [11,12].
The COVID-19 disease outbreak had resulted in many uncertainties in all sectors of health care management. As the elective surgeries are slowly being reintroduced globally, we were fortunate to have had first-hand experience in triaging, prioritizing and treating cancer patients that required elective cancer surgery care during the peak disruption. This systematic approach served as an exemplary to safely resume elective surgery within the limits of national protocols as the pandemic gradually abates. The need to strategize, restructure and sustain cancer surgery services should always be balanced against patient's safety.