Background: Nasal dermoid sinus cyst (NDSC) is a rare congenital lesion, typically presenting at birth or in early infancy. Treatment of NDSC includes complete resection of the mass and the sinus tract, which may extend intracranially. Incomplete resection of the track is associated with high recurrence. We were looking for methods to delineate the NDSC track, without increasing the financial burden to the patient.
Method: The patient was a 12-year-old female who came with a recent onset nasal swelling, which developed near a punctum present since birth. Intraoperatively, we cannulated the sinus and injected methylene blue (MB) dye through it. The dye served as a visual guide for the dissection.
Result: Complete excision could be achieved. No complications or recurrence has been noted after more than a year.
Conclusion: We advocate the use of MB for precise and complete excision of NDSC. The method needs to be explored in a larger series.
Nasal dermoid sinus cyst, Dermoid, Methylene blue, Intracranial, Recurrence, Complete resection
NDSC: Nasal Dermoid Sinus Cyst; MB: Methylene Blue; CECT: Contrast Enhanced Computed Tomography; CT: Computed Tomography; MRI: Magnetic Resonance Imaging
Nasal dermoid sinus cysts (NDSC) are uncommon, occurring in 1 in 20000 to 40000 live births [1]. Here we demonstrate an effective surgical approach involving intraoperative visualization of the sinus track with methylene blue (MB) dye to facilitate complete resection and reduce the incidence of recurrence.
A 12-year-old female presented with a swelling over nasal dorsum of few days duration (Figure 1 and Figure 2). She had a pit over dorsum of nose, since birth, from which occasionally greyish, cheesy, sebaceous material was expressed, for which medical attention was never sought. There was no history of nasal infection or abscess.
 Figure 1: Frontal view of patient showing punctum on dorsum of nose.
View Figure 1
Figure 1: Frontal view of patient showing punctum on dorsum of nose.
View Figure 1
 Figure 2: Right lateral view of patient, showing swelling on dorsum of nose.
View Figure 2
Figure 2: Right lateral view of patient, showing swelling on dorsum of nose.
View Figure 2
The swelling was non tender, smooth, diffuse, globular, not adherent to skin, the deeper margins were insinuated between the nasal bones. There were no signs of inflammation. A midline punctum was noted. A provisional diagnosis of NDSC was made. Contrast enhanced computed tomography (CECT) of head and neck was done. CECT scan detected a small volume of fluid along the nasal dorsum (Figure 3). There was no evidence of bony erosion along anterior cranial fossa and crista galli appeared to be normal for the age (Figure 4).
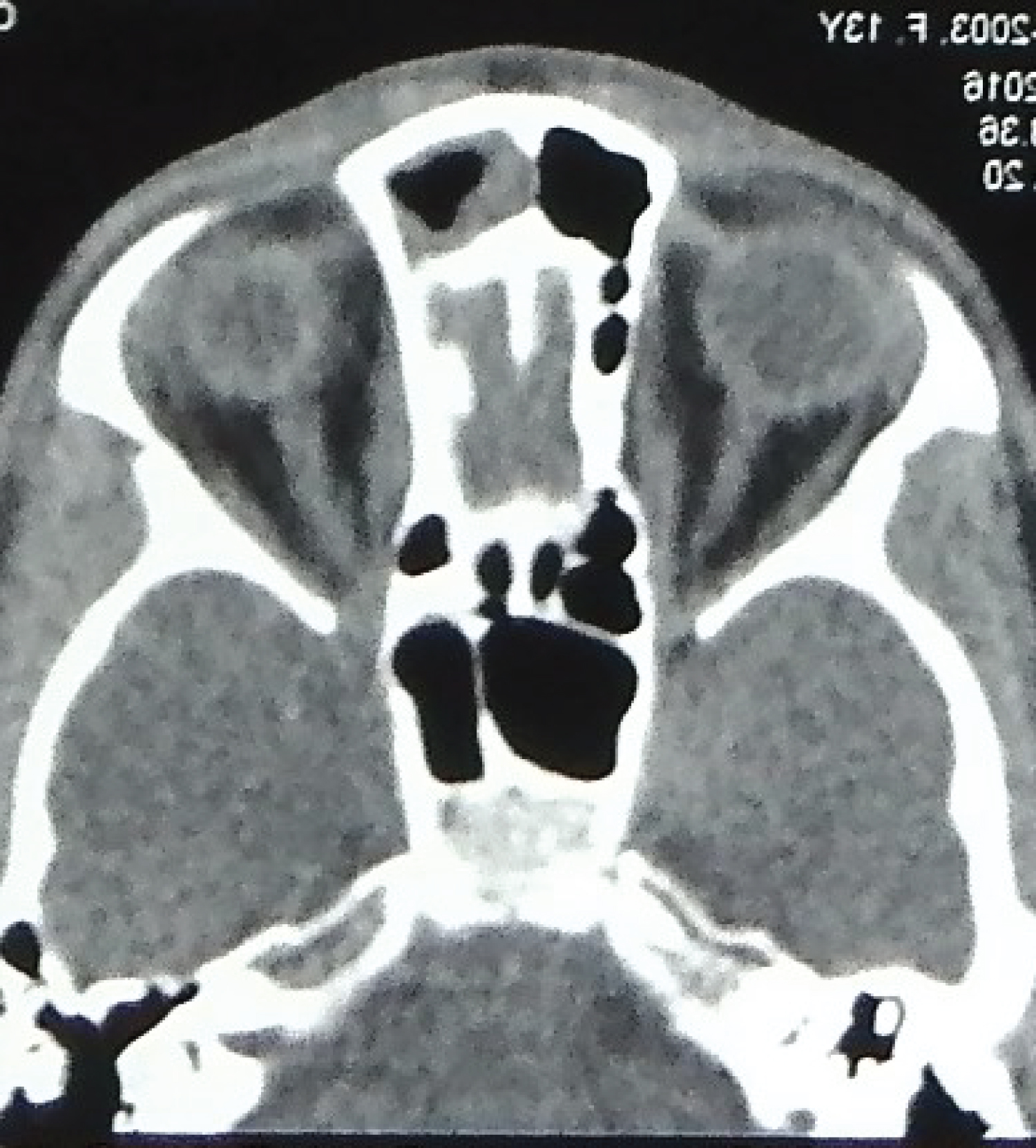 Figure 3: Axial cut of CT scan, showing fluid collection on dorsum of nose.
View Figure 3
Figure 3: Axial cut of CT scan, showing fluid collection on dorsum of nose.
View Figure 3
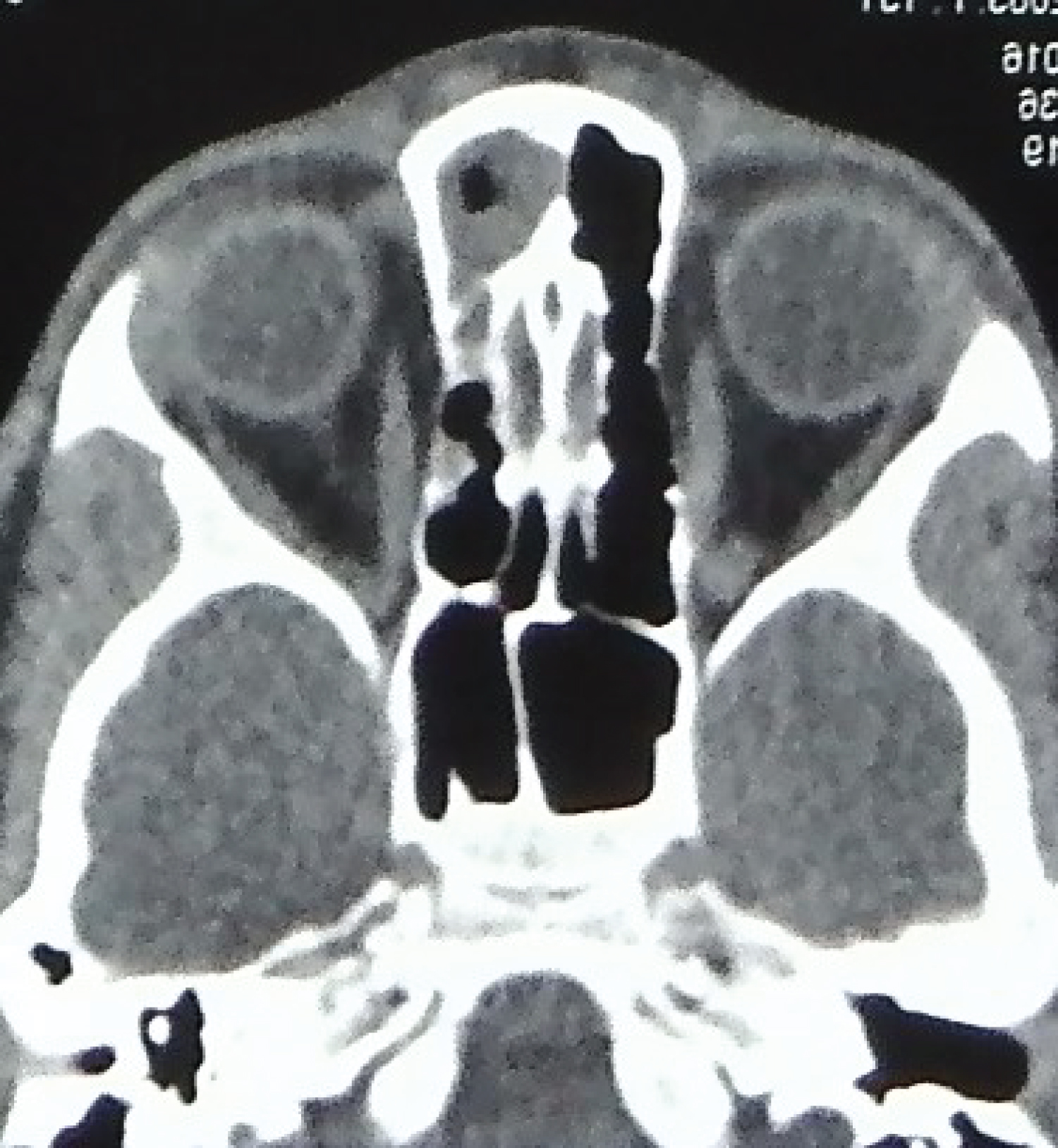 Figure 4: Axial cut of CT scan, showing normal crista galli.
View Figure 4
Figure 4: Axial cut of CT scan, showing normal crista galli.
View Figure 4
Patient was planned for excision of the NDSC. Written consent for photography, for publication of photographs and for surgery was taken. Neurosurgeon was kept on standby in case the track extended intracranially. The patient was taken under general anaesthesia. Sinus track was cannulated using 24 G cannula (Figure 5). 0.2 mL methylene blue dye was injected through the cannula. A vertical elliptical incision was given around the punctum and extended towards the sinus track (Figure 6). Careful sharp dissection was done around the track. 1.2 centimetre sinus track was excised in toto (Figure 7). After excision, no dye was seen in the field. There was open roof deformity in the nasal bones (Figure 8). A percutaneous osteotomy of nasal bones was performed. Layered closure of the incisions was performed.
 Figure 5: Intraoperative picture showing cannulation of the sinus track and marking of incision.
View Figure 5
Figure 5: Intraoperative picture showing cannulation of the sinus track and marking of incision.
View Figure 5
 Figure 6: Intraoperative picture showing dissection of the sinus track.
View Figure 6
Figure 6: Intraoperative picture showing dissection of the sinus track.
View Figure 6
 Figure 7: The excised sinus track.
View Figure 7
Figure 7: The excised sinus track.
View Figure 7
 Figure 8: Intraoperative picture showing total excision of sinus track and open roof deformity of nasal dorsum. There is no dye in the field.
View Figure 8
Figure 8: Intraoperative picture showing total excision of sinus track and open roof deformity of nasal dorsum. There is no dye in the field.
View Figure 8
Wound healed well without any complications. The excised tissue was sent for histopathological examination, which confirmed the diagnosis of NDSC. The patient is in our follow up for more than five years now and there has been no recurrence.
Cruvelier first described a nasal dermoid cyst [2]. Various terms used to describe the lesion-dermoid, dermoid sinus, dermal cyst-led to confusion. Sessions coined the term NDSC to include all lesions containing ectoderm and mesoderm located in the nose [2].
The prenasal theory, by Grunwald attempts to explain the development of NDSC [1]. Between 4 to 8 weeks of gestation, fonticulus frontalis separates nasal and frontal bones, and a prenasal space separates the nasal bones and cartilage [1-3]. A diverticulum of dural mater extends from the anterior cranial fossa through the foramen cecum (which lies anterior to the crista galli) into the prenasal space. It touches the skin of the nose briefly and quickly involutes [1-3]. The nasal and frontal bones fuse, obliterating the fonticulus frontalis. Finally, the foramen caecum is filled with fibrous tissue [1-3].
NDSC occurs when skin is pulled along with the regressing dural diverticulum [1-3]. A sinus tract may form anywhere along the course of the diverticulum [1-3]. Frequency of intracranial connection have been variably reported by Wardinsky (45%), Sessions (31%), Rahbar (19%) and Bradley (4%) [1,2].
The possibility of a transcranial extension necessitates a thorough radiographic evaluation by CT and magnetic resonance imaging (MRI) [1]. It was believed that CT findings of wide foramen cecum and bifid crista galli, are suggestive of intracranial extension [4]. A number of false positive findings led Penslar to review the radiographic images and conclude that an enlarged foramen caecum and a bifid crista galli did not always correlate with intracranial extension [4]. However, a normal foramen caecum and crista galli certainly rules out intracranial disease [3].
On T1 weighted images of MRI, NDSC appear hyperintense [5]. It must be distinguished from the intraosseous fat deposition of crista galli that occurs with normal maturation in most children, by age of 5 years [3].
When there is a dorsal ostium, a vertical elliptical incision has been preferred by Rahbar, which we too, have used [1].
Intracranial extension must be assumed until proven otherwise [1-3]. Incomplete resection is associated with meningitis and recurrence in up to 15% of cases [1]. Sessions and Pensler advocated that craniotomy can be avoided if there is only fibrous track at the cranial base [2,4]. An epithelium lined track would be stained by MB dye and revealed, whereas a fibrous track would not. Thus we used the dye as a tool to guide dissection.
A search of literature revealed other surgeons too used the method for similar indications. Phalen, et al. found that in about 20% of their cases, preoperative imaging was not consistent with intraoperative findings, and they used MB to delineate the extent of dermoid cyst [6]. Verma and Saha used MB to facilitate dissection of the dermoid sinus [7,8]. Histological examination of frozen sections of the tissue from base of track to detect dermal elements, is another method to determine completeness of resection [9].
Use of MB to stain tissues for dissection is not new. MB has been used to stain cysts, sinuses and ulcers of pressure sore, pilonidal sinus and ganglion [5,10,11]. Dorafshar used the dye to detect minute sinuses in burn wounds [12]. MB is used to stain suspected cancerous tissues of uterus, cervix, oral cavity, liver and colon [13,14]. It was the first synthesized drug used for treating malaria [15]. MB has been used to facilitate removal of accidentally embedded metallic foreign bodies in children [15].
Extensive systemic use have shown it to be a safe drug [12,13]. It can be sterilized by autoclaving and is stable after high temperature and high pressure sterilization [13]. The dye is inexpensive and widely available [12]. The time and labour added to the surgery is far outweighed by the benefits of complete resection.
NDSC is a rare congenital lesion, which often poses diagnostic and surgical dilemma. Extent of surgery is guided by the sinus track and an intracranial approach may be needed. Intraoperatively we were guided by MB in our dissection. MB has a long history of use, for a myriad list of conditions and has a safe record. The dye has the potential to reduce surgical trauma and improve success rate. The technique needs to be explored in a larger series.
The author acknowledges the faculty and staff of the parent institute.
None declared.
None.