Whole-body computed tomography (WBCT) is one of the standard non-invasive tests for trauma patients, to avoid the overuse of the WBCT and unnecessary radiation to the patients, a combination of evidence-based indications, approved guidelines and clinical decisions should be used.
This study was done to emphasize on limitation of unnecessary WBCT following international or local criteria along with clinical assessment and decision without compromising the patient's safety.
This study was performed in King Fahad Hospital-Emergency Department in Albaha region in the kingdom of Saudi Arabia, the study was done in the period from January 2020 to December 2020, the study population is polytrauma patients of the age of 18 years old and above, it is a descriptive, retrospective database analysis of 233 patients diagnosed with polytrauma in the emergency department, all patients were received by emergency physicians and trauma team members, where they received their initial management and stabilized then sent to the Radiology department for WBCT according to the order by senior ED physician or on-call surgeon who is a member of the trauma team, Informed consent was taken according to the hospital protocol.
Whole-body CT was carried out on 233 polytrauma patients arriving at the emergency department, the outcome of the WBCT was n ≈ 70 (30%) were reported as, n ≈ 87 (37.3%) they have a single organ involved in trauma and n ≈ 76 (32.7%) the reports came with multiple organs (more than 1) involved in trauma.
This study showed slight overuse of WBCT in our facility, of the studies were reported. The combination of the senior clinical staff, application of appropriate local or international evidence-based criteria for performing WBCT will lead to avoiding a good number of unnecessary WBCT, radiation exposure, and side effects of contrast materials besides reducing the costs for the health services.
Whole-body CT, Polytrauma, Single organ, Emergency department
Whole-body CT is one of the standard non-invasive investigations in polytrauma patients in the emergency setting; proper clinical examination and standard indications for WBCT will reduce the unnecessary WBCT and convert it to the selected organ.
Discharging of patients from ED based on normal WBCT report is becoming questionable and controversial, furthermore, the high radiation dose of WBCT for younger patients and the risk of cancer cannot be ignored [1], one of the objectives of this article is to encourage health care systems and emergency settings to develop guidelines for utilization of WBCT in emergency departments [2].
Using other modalities of imaging in polytrauma patients like FAST and X-rays, might not be satisfactory for some physicians to avoid WBCT, this might be due to lack of skills of operating the bedside ultrasound machine, lack knowledge of interpretation the simple X-rays or for medicolegal purposes, although some researches showing that when medical staff using others modalities of imaging the result is reducing the percentage of negative WBCT [3].
Saudi Arabia has a high number of road traffic accidents, 2020 according to the Ministry of health statistics there are total injuries of 25,561 and 4,618 deaths, the Saudi health system is providing the emergency departments and trauma centers with very advanced high technical machines for imaging and scanning of trauma patients in which we need to make a proper prioritization and utilization of it especially the CT machines to avoid the disadvantages of unnecessary radiation [4].
Many trauma centers have clear justifications for performing WBCT which is shared between the physicians and radiologists [5], however, there is several patients seem to be matching with the criteria for WBCT but the final report is normal WBCT, this safety margin of error looks acceptable for the most of the physicians and health system as well [4].
Whole-body CT enhanced with single contrast has special indications for detecting penetrating abdominopelvic trauma and suspected bowel injuries, studies are showing that single contrast is accurate as of the same of triple contrast (IV, Oral and rectal) [6], many physicians when they request a WBCT they are requesting contrast study either intravenous, oral or rectal as routine regardless the presents of abdominal trauma or penetrating injuries, contrast materials have many immediate or delayed side effects which should be considered by the treating physicians and to avoid it whenever it is possible [7].
It is the responsibility of the health system and quality sections in the hospital to provide the emergency system and physicians with established guidelines and protocols to reduce the overuse of WBCT in the polytrauma patient.
This study was performed in King Fahad Hospital-Emergency Department in Albaha region in the kingdom of Saudi Arabia, the study was done in the period from January 2020 to December 2020, the study population is polytrauma patients of the age of 18 years and above, it is a descriptive, retrospective database analysis of 233 patients diagnosed with polytrauma in the emergency department, all patient was received by emergency physicians and trauma team members, they have received their initial management and stabilized then sent to the radiology department for WBCT according to the order by senior ED physician or on-call surgeon who is a member of the trauma team, Informed consent was taken according to the hospital protocol.
All WBCT requested with enhanced single intravenous contrast, requests are excluding non- contrast studies, single organ trauma, and pregnant.
The information extracted from the hospital database after appropriate ethical permissions, we took the age, sex, mode of trauma, and later the radiology report findings.
Whole-body CT was carried out on 233 polytrauma patients was arrived at the emergency department (Table 1), 197 (85.5%) are males 36 (14.5%) are females, the age of n ≈ 167 (71.6%) were between 18-40 years-old (Table 1), n ≈ 212 (91%) of those patients mode of trauma is road traffic accidents (RTA), n ≈ 17 (7.3%) fall from high more the 2 feet, n ≈ 4 (1.9%) were assaulted, trauma by a heavy object and gunshot (Table 2), the outcome of the WBCT were n ≈ 70 (30%) were negative findings, n ≈ 87 (37.3%) they have a single organ involved in trauma and n ≈ 76 (32.7%) the reports came with multiple organs (more than 1) involved in trauma (Figure 1).
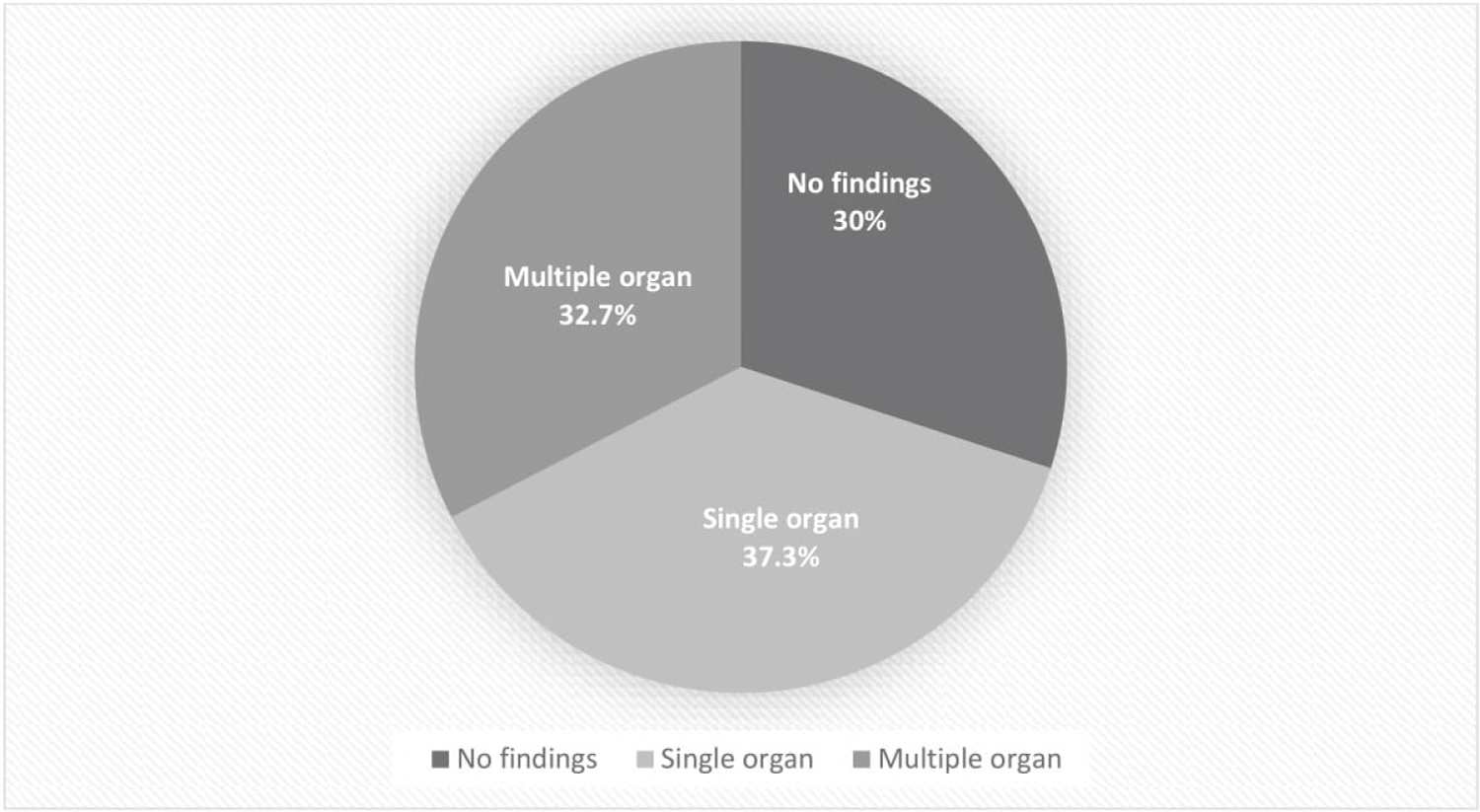 Figure 1: The outcome of WBCT reports.
View Figure 1
Figure 1: The outcome of WBCT reports.
View Figure 1
Table 1: The age group of the patients. View Table 1
Table 2: The mechanism of trauma. View Table 2
The frequency of organs involved in trauma we found chest injuries n ≈ 35 (15%) as an isolated injury head injuries n ≈ 28 (12%), head and chest trauma n ≈ 26 (11.2%), while vascular and pelvic injuries are minimal percentages n ≈ 1 (0.4%) (Table 3).
Table 3: The organs involved in the trauma. View Table 3
In the disposition of the patients, we found that n ≈ 171 (73%) of the patients were admitted in different wards between intensive care unit and regular wards, and n ≈ 62 (26.6%) was discharged from the emergency department.
Further, Bivariate statistical analysis was done with chi-square test, which showed statistical significance with p-value < 0.05 between the number of organs involved in trauma and the positive outcome of WBCT, admission of the patients, age of the patient is correlated significantly with the age (p-value < 0.05).
There is an increasing concern in health systems regarding the risks of radiation from advanced modalities of computed tomography imaging especially when it is repeated either immediately when patients are transferred between facilities or departments, another concern raises when some articles show that there is a considerable percentage of healthcare workers are not aware of the risks of radiations, which is found around 40% of emergency departments doctors are not aware of radiation risks in the Australian research, same research done in Kingdome of Saudi Arabia showing the need of more education about radiation risks.
In this study, there is a percentage of 30% of WBCT done in the emergency department for trauma patients of no findings which are considered in the middle site in percentages in comparison with several international studies which the negative WBCT ranges from 7% to 57% in some international centers [8,9], but it is almost the same in comparison with two studies done in KSA which one showing 30% of negative WBCT in trauma patients and other one fare less around 20% of negative WBCT [10], this finding in our research although it shows reasonable percentage in KSA but still in the higher limit and raising the concern regarding the unnecessary exposure to radiation which supporting the author's theory, which it might lead to many unfavorable effects for patients from radiation dose although it proved that the chance of causing cancers from medical radiation is very low but also some patients might have their fear and should be considered, also the direct effect is to health economic system and considered part of the unnecessary waste of resources either human or financial resources.
Furthermore, our study found that 37.3% of the trauma patients had a report of single organ trauma mostly head 12% and chest 15% trauma respectively, in some international guidelines of trauma management the most first indication for WBCT is trauma to two or more organs, although there is important meta-analysis research showing that WBCT in patients with major trauma will reduce the mortality and the time of admission in the emergency department [11], still, the emergency physicians should assess the needs of WBCT especially when clinically there is one organ from simple trauma and not to use to do WBCT unless for selected patients and senior physicians and surgeons opinions.
We have found that the trauma 91% of the patients were due to MVA, this might indicate the increasing tendency of emergency physicians or surgeons to request WBCT for trauma patients, appropriate clinical assessment, the use of Focused Assessment Sonography for Trauma (FAST), XRs and local trauma guidelines might reduce this tendency and unnecessary WBCT as well.
Our additional observation during data review and analysis shows that most of the requested WBCT based on the mechanism of injuries, according to international researches in the trauma field the indications of WBCT has multiple criteria including the mechanism of trauma, anatomical criteria, and physiological criteria [12] assisted by others approved international criteria like NEXUS criteria for spinal injuries, NIC criteria for CT brain [13] and FAST scan, along with frequent monitoring combined with clinical decisions [14].
During our review of the database, we noticed some patients who were transferred to KFH for further management from peripheral hospitals, WBCT have been repeated for them for different reasons like technical issues when they transfer the WBCT data, or for reassessment issues by admitting teams, this observation is out of the scope of this article but we recommend to make further separate statistics and workup regarding this issue to avoid double radiation exposure to the trauma patients within hours or days, also the use of contrast for these patients although Contrast materials are safe; reactions ranging from mild to severe and fatal might happened, severe reactions are uncommon [15]. While serious allergic or other reactions to contrast materials are rare, but the admitting team of the emergency physician should make all the effort to use the same previous WBCT unless there are strong clinical indications and not to be as routine for further documentation.
This study has some limitations. One of the major limitations it is conducted in a single hospital in the region which might limit the results to this facility without integrating the same results from other centers and hospitals in KSA, the study is only done in the patients who are received through the emergency department and missing some trauma patients accepted directly for admission from others hospitals, also we couldn't include the patients who had repeated WBCT in our hospital when it has been done before in others peripheral hospitals due to unavailability of data. finally, all patients who have done WBCT due to trauma are included in the study regardless of their condition on arrival to ED required trauma team activation or not which might indicate the routine utilization of WBCT.
This study shows a slight overuse of WBCT in our facility, 30% of reports came of negative findings, and 37.3% of patients their WBCT reports came with single organ trauma. The combination of senior's clinical decisions; application of appropriate local or international evidence-based criteria for performing WBCT will lead to avoiding a good number of unnecessary WBCT, radiation exposure, and side effects of contrast materials besides reducing the costs for the health economic system.