Induction antibody immunosuppressive protocols in children have been extrapolated from experience gained primarily from kidney transplantation in adults and are center-specific. There is a paucity of information on the clinical and immunological effects of these protocols in children.
To assess clinical characteristics and trends in peripheral blood lymphocytes over time after pediatric kidney transplantation with our center-specific dual antibody induction protocol.
Retrospective chart review was performed in all pediatric kidney transplant recipients less than 21 years of age at the Miami Transplant Institute during the period of January 2012 to June 2015. Relevant demographic, clinical characteristics and data on lymphocyte subset analysis were collected. Our protocol consisted of an average of 4 doses of rabbit anti-thymocyte globulin (rATG), 2 doses of basiliximab and rapid methylprednisolone taper.
Between January 2012 and June 2015, 50 children < 21 years were transplanted, of which 40 children received our standard dual induction protocol. Maintenance immunosuppression consisted of tacrolimus (levels -6-8 ng/ml) and mycophenolic acid and was steroid free in 95% of children. Median age was 9.0 years and 60% were Hispanic and African American. Following a normalized square root transformation, there was a post-transplant nadir in CD4+ (-74.3%), CD8+ (-58.8%), NK (-68.5%) and CD25+ cells (-93.7%) at one week, and CD19 and HLADR at 4 weeks (-31.1% and -31.6%, respectively). At one year, most cells returned to just under baseline levels. CD4+CD25 bright (Treg) cells were low at 4 weeks and peaked at 24 weeks post-transplant. One- and 3-year graft survival were 98%, and 94%, respectively, and patient survival was 100%. No patients developed post-transplant lymphoproliferative disease.
This study contributes to understanding the clinical and immunological effects of a dual antibody induction therapy which facilitates steroid sparing and lower doses of calcineurin inhibitors in a multiracial group of children. Future studies comparing these patterns across various immunosuppressive protocols are warranted.
Pediatrics, Kidney transplantation, Lymphocyte subsets, Anti-thymocyte globulin, Induction therapy
rATG: Rabbit Anti-Thymocyte Globulin; CMV: Cytomegalovirus; EBV: Epstein Barr Virus; PCR: Polymerase Chain Reaction; eGFR: Estimated Glomerular Filtration Rate; DSA: Donor Specific Antibodies; cPRA: Calculated Panel Reactive Antibody
Improvement in short-term kidney transplant survival has partly occurred as a result of innovations in immunosuppressive therapies designed to prevent acute rejection [1]. Based on the observation that greater immune suppression is required immediately after transplantation to prevent acute rejection, intensive efforts have been employed to suppress the immune response to the allograft in the peri-operative period [2,3]. With this goal in mind, one approach, which has been associated with improved patient and graft outcome, is to use antibody induction therapy [4].
In children, immunosuppressive protocols have been extrapolated from experience gained primarily from kidney transplantation in adults [1]. Currently, in the United States, 60% of pediatric transplant centers use monoclonal and 25% polyclonal antibodies for induction therapy [5]. There is a wide variation in induction immunosuppressive protocols. However, there is scant data on the clinical effect, immune depletion and recovery after induction immunosuppressive protocols in children after kidney transplantation. In recent years, we have been systematically collecting data on DSAs, lymphocyte sub-sets and viral PCRs at our institution. We therefore used these parameters to evaluate the clinical impact of our immunosuppressive protocol.
The purpose of this retrospective observational study was to evaluate clinical characteristics and trends in depletion and recovery of peripheral blood lymphocytes over time with our center-specific dual antibody induction protocol with basiliximab (IL-2Rα blocker) and rabbit anti-thymocyte globulin (rATG) in children.
Patient's medical charts were reviewed for all pediatric kidney transplant recipients less than 21 years of age at the Miami Transplant Institute during the period of January 2012 to June 2015. Fifty transplant recipients were identified during the study period. Demograghics, donor type and calculated panel reactive antigen were documented. From this group, patients were separated into 2 sub-groups 1) 40 patients who did not receive additional immunomodulatory drugs due to rejection or other graft disease and 2) 10 patients who received additional immunomodulatory drugs because of acute rejection or other disease such as focal segmental glomerulosclerosis (FSGS) in the allograft. Data on lymphocyte subsets (CD4, CD8, CD19, CD25, NK, HLADR+ and CD4+CD25 bright cells), were collected pre-transplant, and at 1, 4, 26, 52- and 156-weeks post-transplantation. Other collected information included episodes of infections, donor specific antibodies, estimated glomerular filtration rate (eGFR) and immunosuppressive drug levels. CD4+CD25 bright cells were used as a surrogate marker for T regulatory cells. Human subject's approval was obtained from the institutional review board of the University of Miami, Miller School of Medicine.
Intra-operatively, all patients received intravenous basiliximab at a dose of 10 mg if weight was less than 35 kg, and 20 mg if weight was greater than 35 kg. This was followed by methylprednisolone at 10 mg/kg body weight (maximum 500 mg) and intravenous thymoglobulin (rATG) at 1 mg/kg. rATG was continued for a total of 3-5 doses (average cumulative dose was 4.2 ± 1.1 mg/kg) and a second dose of basiliximab was given on the fourth post-operative day. If the total white cell count was below 4,000/micro liter, no further doses of rATG were given. Methylprednisolone was continued post-operatively at 10 mg/kg on post-operative day 1, then tapered by 2 mg/kg daily and discontinued between post-operative days 5-7, when therapeutic levels of tacrolimus were obtained (target level 6-8 ng/ml). Two patients required low dose steroids for maintenance therapy because of re-transplantation and microscopic polyangiitis. Oral mycophenolate mofetil was introduced on the second post-operative day at a dose of 500 to 1000 mg/m2/day. Dose adjustments were made depending on the white blood cell count, gastro-intestinal tolerance or evidence of viral PCR replication with cytomegalovirus (CMV), Epstein Barr virus (EBV) or BK Virus. Oral tacrolimus was introduced once serum creatinine was less than 3 mg/dl in children older than six years of age, and less than 2 mg/dl in those who were younger. The mean dose of tacrolimus and mycophenolate mofetil when stable levels were achieved, were 0.17 mg/kg/dose and 484 mg/M2/day, respectively. Risk assessment of recipients for CMV and EBV, were determined pre-operatively. High-risk recipients (CMV or EBV serology positive donor; negative recipient) were given valganciclovir at prophylactic doses for 6 months, and those with low or intermediate risk (CMV or EBV positive or negative donor to CMV or EBV positive recipient) were given prophylaxis for 3 months. All patients received prophylaxis against pneumocystis carinii infection with trimethoprim/sulfamethoxazole which was continued throughout the life of the transplant.
Infections were classified as viral if there was replication of Epstein-Barr virus (EBV), cytomegalovirus (CMV) and BK virus (BKV) greater than 1000 copies/ml by real time polymerase chain reaction (PCR). Invasive viral disease was defined as having a tissue diagnosis of viral infection. Culture-positive febrile urinary tract infections and bacteremia were classified as bacterial infections. Renal function was determined by estimating glomerular filtration rate (eGFR) using the modified Schwartz equation in patients ≤ 18 years or the CKD-EPI equation for patients ›18 years [6,7]. Donor specific antibodies (DSA) was defined as presence of antibodies against human leukocyte antigens to the donor in the recipient. Graft survival was defined as the percentage of functioning grafts at one and 3 years. Acute rejection was defined as a sustained rise in serum creatinine by > 25% with biopsy- proven evidence of rejection.
Aliquots of 100 microliters of whole blood were stained with surface antibody cocktail for 30 minutes at room temperature. Samples were then lysed with VersaLyze™ reagent and IOTest®3 fixative solution (Beckman Coulter A07800). To determine the absolute count of each cell subset, 100 microliters of Flow-count™ fluorophores were added. Samples were then analyzed with the Navios Flow Cytometer (Beckman Coulter) and Kaluza® flow cytometry analysis software. Four color flow panels were used for cytometry. Lymphocytes of interest were then gated from the CD45/SSC plot.
Categorical data were analyzed with Chi square or Fisher's exact test as appropriate. To normalize the distribution of lymphocyte counts, a square root transformation was applied. Lymphocyte counts were plotted over time - pre-transplant, 1, 4, 26, 52 and 156 weeks, post-transplant. These data represent a single sample longitudinal study in which time was the sole fixed independent effect. Accordingly, the statistical model used to access average statistical changes over time was a single sample mixed model where subject-to subject variation was accounted for by a random subject component. Trend analysis, including polynomial regression and specific multiple comparisons (i.e., Tukey's HSD), was derived from the overall repeated measures model. An autoregressive variance-covariance structure (i.e., Autoregressive (1) was used to model the dependency between repeated measurements. Statistical analysis was performed with JMP® Pro statistical analysis software (SAS Institute Inc. Cary, NC, version 12.0.1). Graphs were created in Graphpad Prism® software.
Demographics, donor source and mean HLA mismatches are displayed in (Table 1). A majority of the subjects were Hispanic or African American (60%) and there was a predominance of deceased donor transplants (78%). Among the 11 (22%) patients with living donor (LD) transplants, 3/11 (27.3%) received living unrelated kidney transplants. The most common primary diagnosis was congenital anomalies of the kidneys and urinary tract (70%). Four of the fifty patients had other graft disease and six had acute rejection. These patients received additional immunomodulatory drugs.
Table 1: Demographic characteristics. View Table 1
Of the initial 50 patients, 40 patients received our standard antibody induction protocol of 3-5 doses of anti-thymocyte globulin, 2 doses of Basiliximab and methylprednisolone taper. They did not receive additional immunomodulatory therapy such as anti-CD20 monoclonal antibody, intravenous immunoglobulin or plasmapheresis. Patients in this category were more likely to have congenital kidney disease (OR: 5.2; 95% CI 1.2-24.7; p < 0.03).
Lymphocyte subsets: The sub-group of 40 patients were separately analyzed with the rationale that the additional lymphocyte depletive effect of the immunomodulatory drugs would confound the results if patients with rejection or other graft disease were included. The (Figure 1A) and 1B display the square root of the ALC, CD4+, CD8+, CD25+, CD 19+, NK cells and HLADR+ cell counts plotted by time. After initiation of therapy, there was a decline (all P's < 0.0001) in CD4, CD8 and CD25 at one week with an increasing linear (CD25, P < 0.0001) or quadratic (CD4 and CD8, P's < 0.0371) trend in counts from 1 to 52 weeks (Figure 1A and Figure 1B). The percent decline in each subset was: CD4+ (-74.3%), CD8+ (-58.8%), NK (-68.5%) and CD25+ cells (-93.7%) at one week post-transplant; CD19+ and HLADR+ cells reached a nadir at 4 weeks post-transplant (-31.1% and -31.6%, respectively). The response of CD19 to therapy was muted compared to CD4, CD8, and CD25 and the decrease from baseline was not statistically detectable until 4 weeks (P < 0.0001). This decrease remained constant for 26 weeks with a slight increase at 52 and 156 weeks (Figure 1B). The time course of the NK cells was similar to that of the CD4, CD8, and CD25 cells, while the time course of the HDLR cells were similar to that of the CD19 cells (Figure 1B). There was a modest suppression of CD4+, CD 19+ lymphocytes and NK cells at one year. CD8+ T cells and HLADR cells reached baseline levels at one year.
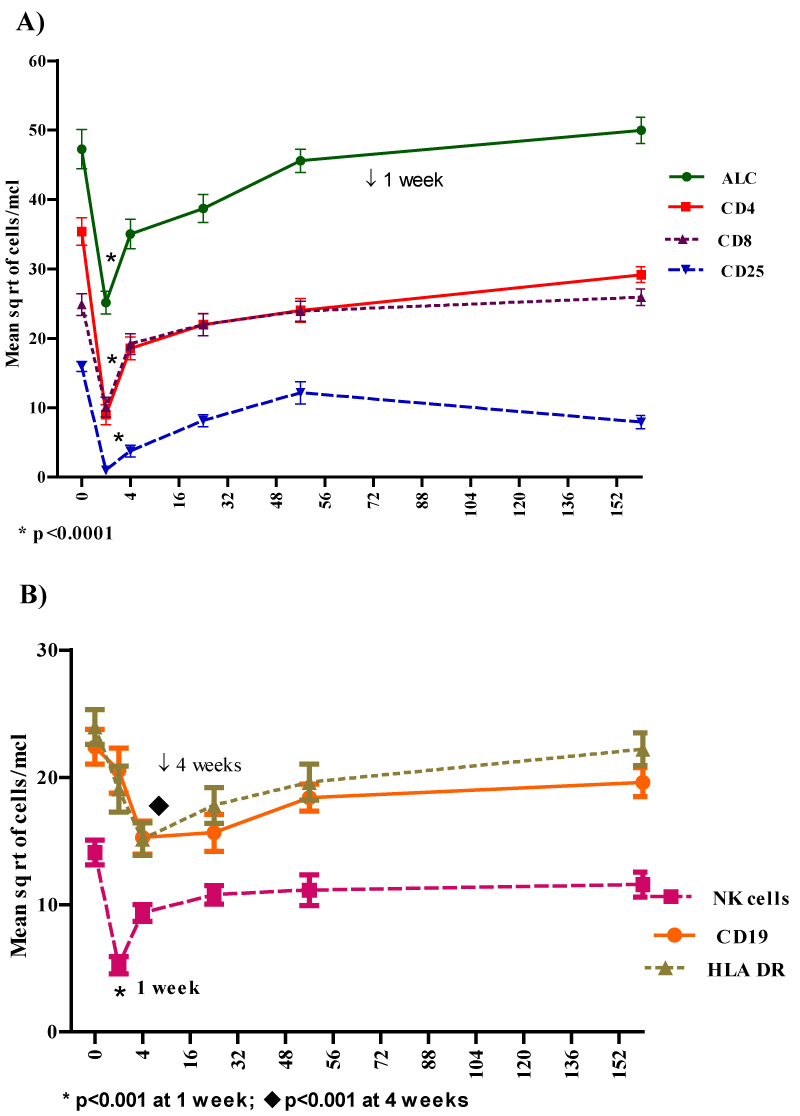 Figure 1: A) Absolute lymphocyte count (ALC), CD4+, CD8+ and CD25+ T cells over time following the dual induction protocol in patients who received no additional immune-modulating treatment for rejection or other graft disease. The nadir occurred at 1 week with a gradual recovery. B) CD19 and HLA DR positive cells reached a nadir at 4 weeks with gradual recovery. NK cells followed the pattern of CD4+ and CD 8+ cells.
View Figure 1
Figure 1: A) Absolute lymphocyte count (ALC), CD4+, CD8+ and CD25+ T cells over time following the dual induction protocol in patients who received no additional immune-modulating treatment for rejection or other graft disease. The nadir occurred at 1 week with a gradual recovery. B) CD19 and HLA DR positive cells reached a nadir at 4 weeks with gradual recovery. NK cells followed the pattern of CD4+ and CD 8+ cells.
View Figure 1
The square root of CD4+CD25 bright T regulatory cells were evaluated at 4, 24, 52 and 156 weeks. These cells were low at 4 weeks, reached a peak in 24 weeks and thereafter had a slow decline (Figure 2).
 Figure 2: Figure depicts pattern of depletion and recovery over time of CD4+CD25 bright cells in patients who received no additional immune-modulating treatment for rejection or other graft disease CD4+CD25 bright cells are a surrogate marker of T regulatory cells.
View Figure 2
Figure 2: Figure depicts pattern of depletion and recovery over time of CD4+CD25 bright cells in patients who received no additional immune-modulating treatment for rejection or other graft disease CD4+CD25 bright cells are a surrogate marker of T regulatory cells.
View Figure 2
Infections and donor specific antibodies: As seen in (Table 2), nine of forty patients (22.5%) had evidence of viral replication of which 8 had no evidence of clinical disease. All were managed with reduction in immunosuppression and 5 were treated with anti-viral agents. One of the nine had evidence of BK virus nephropathy. No patients developed post-transplant lymphoproliferative disease. Eleven of 11/40 (27.5%) had a urinary tract infection. When these clinical characteristics were assessed at 3 years, there was no significant difference in incidence (Table 2).
Table 2: Clinical characteristics. View Table 2
Mean tacrolimus levels at 1 month and 1 year were 6.6 ± 0.9 and 6.25 ± 0.9 ng/ml, respectively. Average dose of mycophenolate mofetil at 1 year was 464 ± 208 mg/M2/day. Donor specific antibodies developed de novo in 3 of 40 patients at 1 year and resolved in 1 of 3, after increasing immune suppression with no significant difference at 3 years as seen in (Table 2).
Of the initial 50 patients, 6 had rejection, 3, recurrent FSGS and 1, drug induced interstitial nephritis. Of the 6 patients who had acute rejection, 3 had early rejection within the first 6 weeks of transplant. Of the early rejecters, two had high pre-transplant panel reactive antibodies and one had sub-optimal tacrolimus levels from gastrostomy tube leakage. The others were non-adherent to their treatment regimen and had rejection at ≥ 6 months. Graft loss occurred in 1 patient in the first year from consequences of systemic bacterial infection and 2 others in 2 years because of repeated episodes of rejection. Mean tacrolimus levels at 1 month was 8.2 ± 2.5 and at 1 year 5.1 ± 1.7 ng/ml, respectively. At 1 year, 3 patients were also on sirolimus to achieve lower levels of tacrolimus and to preserve kidney function. Average dose of mycophenolate mofetil in this group at 1 year was 739 ± 300 mg/M2/day. Demographic characteristics, donor source, primary disease, calculated panel reactive antibody (cPRA) > 50% and donor specific antibodies (DSA) were compared between those with no rejection versus those with rejection as seen in (Figure 3). The nature of the primary disease did not increase the odds of rejection. The odds of rejection trended higher with male gender, African American race, older age and higher pre-transplant cPRA. However, the presence of DSAs posed the most risk of rejection (OR: 62; CI 5.3-700; p < 0.0002).
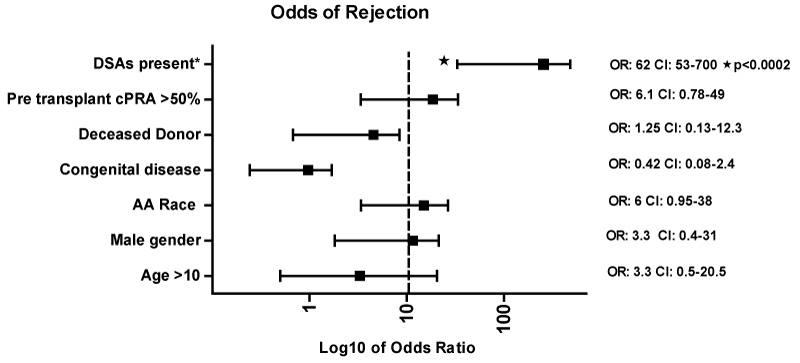 Figure 3: Forest Plot depicting the association of variables with rejection. Presence of DSAs was significantly associated with rejection.
View Figure 3
Figure 3: Forest Plot depicting the association of variables with rejection. Presence of DSAs was significantly associated with rejection.
View Figure 3
Lymphocyte subsets: Analysis of lymphocyte subsets in children who received immunomodulatory drugs for rejection or other disease, revealed a significant suppression of CD8 (p < 0.04), NK cells, CD19 and HLADR+ cells (p < 0.001) at all time points. CD 4+ or CD25+ cells were suppressed significantly at 1 and 4 weeks (p < 0.0004) but not after 24 weeks. However, lymphocyte subsets were not analyzed prior to rejection therapy in late rejecters. The square root of CD4+CD25 bright T regulatory cells was low at 4 weeks, reached a peak in 24 weeks and was low in 3 patients evaluated at 3 years.
Infection: (Table 1) displays these characteristics in patients with rejection and other graft disease. Two patients with recurrent FSGS had CMV and BKV viral replication without clinical evidence of disease requiring anti-viral treatment (CMV) and lowering of immunosuppressive maintenance therapy.
One- and three-year graft, patient survival and eGFR: One-year graft and patient survival was 98% and 100%, respectively. In the second and third year after transplantation, two patients from the initial cohort of 50 patients had repeat episodes of rejection from nonadherence with loss of their allograft. Three-year graft and patient survival were 94% and 100%, respectively. Although there was a slight decrease in trend in eGFR at 1 and 3 years in those without rejection, the difference was not statistically significant. eGFR was decreased at 1 year in those with rejection compared to those without rejection ((p ≤ 0.03); (Table 2).
Graft rejection and infections play an equally important role in morbidity, mortality and graft loss in transplant recipients [8]. An ideal goal in solid organ transplantation would be to determine the net state of immune suppression in order to decide the optimal dose of immunosuppressive drugs that would prevent rejection without increasing the susceptibility to infection. Currently, post-transplant induction and maintenance treatment regimens are guided by center-specific protocols and experience. Given the paucity of controlled comparative studies between specific induction protocols in children, it is important to understand the clinical impact of immunosuppressive regimens following transplantation [2,3,9]. Our study highlights the fact that most of the children were on a steroid free protocol and were maintained on a relatively low calcineurin inhibitor therapeutic regimen. An additional advantage of the dual induction therapy was that it allowed the use of a lower cumulative dose of rATG compared to other studies [6,7,10,11].
The rationale for our dual induction protocol was based on our institutional observation that r-ATG alone did not result in a sustained decrease in CD25 expressing cells. Therefore, basiliximab was added to the induction regimen [12,13]. Furthermore, the addition of basiliximab had the added advantage of minimizing the dose of rATG which was a unique feature of our dual induction therapy. Immune reconstitution is dose dependent, as higher cumulative doses of rATG result in longer time to reconstitute [6,9,13]. There was a faster recovery of lymphocyte subset counts with our immunosuppressive protocol compared to other studies [6,9,13]. However, alternative strategies need to be devised in highly sensitized patients (as they continue to be at a higher risk of rejection) and in patients with nonadherence.
Steroid avoidance regimens are associated with a higher risk of rejection and therefore are characterized by an increased use of induction agents such as monoclonal antibody or lymphocyte depleting agents [14,15]. Evidence from the united network for organ sharing database suggests that children who receive steroid-free immunosuppression are more likely to be recipients of living donor kidneys and non- African American [15]. The TWIST study compared anti-CD25 monoclonal antibody induction and steroid avoidance, with a steroid based immunosuppressive protocol. Doses of MMF were high and tacrolimus levels were maintained as high as 10-20 ng/ml in the first 3 weeks with a wider therapeutic range (5-15 ng/ml) in the short follow up period of 6 months [16]. Therefore, alternative approaches to immune suppression need to be considered for steroid avoidance to minimize the risk of rejection. We were able to use lower doses of maintenance immunosuppression with the dual induction protocol.
Prolonged lymphopenia results in a higher risk of infections and malignancy [17-19]. Added advantages to our protocol were, most patients were maintained steroid free, with comparatively lower doses of maintenance immune suppression with mycophenolate mofetil and tacrolimus. This may be a contributing factor in the low incidence of invasive infections which has been reported with higher doses of mycophenolate mofetil [20,21]. Viral replication is often observed in children following kidney transplantation [22]. However, in our study only one patient had invasive BK virus nephropathy, and none developed post-transplant lymphoproliferative disease during the observation period. Therefore, our protocol does not seem to confer an increased risk of invasive viral disease or malignancy in the first post-transplant year, when the degree of immune suppression is at its peak and in the following 2 years. The incidence of urinary tract infections requiring anti-bacterial treatment was comparable to other studies [23].
Other adverse factors associated with maintenance immunosuppressive therapy limiting long term kidney transplant and patient survival include nephrotoxic, cardiovascular, malignant and metabolic complications. Decreased doses of calcineurin inhibitors and a steroid free regimen, could potentially mitigate these complications [24].
Studies suggest that after depletive induction therapy, there is homeostatic proliferation of lymphocytes of which some assume a regulatory or memory cell phenotype [6]. We observed a resurgence of T regulatory cells at 6 months, but a gradual decline after that. This phenomenon requires further study, but could be related to maintenance immunosuppressive therapy which may have also contributed to a modest suppression of CD4+, CD 19+ lymphocytes and NK cells in our patients even at one year [25]. Similar to what was observed in other studies, CD8+ T cells reached baseline levels at one year [9,13]. We observed a modest initial decrease in HLADR expression which returned to baseline levels at one-year post-transplant. Up-regulation of HLADR has been shown to increase with both rejection and viral infections [26]. The practical application of this observation is yet to be determined.
The limitation of this study is that it is retrospective and purely observational. As this was a single-center experience, comparisons between different immunosuppressive protocols were not made. Protocol biopsies were not routinely performed to evaluate histologic correlates of treatment effects. Six subjects experienced rejection but had justifiable explanations such as high degree of sensitization and non-adherence. Thus, the generalizability of our results only extends to immunologically low risk patients and those not experiencing rejection.
The optimal dose and type of induction therapy after kidney transplantation in children which has minimal risk of acute rejection and/or infection is not known. The non-inferiority of this dual induction therapy cannot be established in this study because of a lack of a comparison group. However, a steroid free maintenance regimen and lower calcineurin inhibitor levels were attained. Risk of infection and malignancy are major concerns with excessive doses of induction. However, the combination regimen of basiliximab and low dose rATG did not result in excessive infectious complications or post-transplant lymphoproliferative disease.
Traditionally, monitoring maintenance immunosuppressive treatment is based on maintaining drug levels within a specified range. Urinary chemokines and cytokines can be used as predictors of inflammation but may not predict the net state of immune suppression which could be useful to stratify the risk of infection and malignancy [27]. Consideration should be given to routinely monitoring immunological parameters in addition to monitoring markers of inflammation to individualize immunosuppressive therapy. Our study gave us the opportunity to observe the effects of this protocol in a group of children with a lower ratio of Caucasians. The immune depletion effect of our dual induction therapy appears to last for approximately one-year post-transplant. One-year graft and patient survival are comparable to published normative data and 3-year graft survival exceeded the national average [3]. Continued emphasis needs to be placed on research that improves allograft acceptance while avoiding excessive immune suppression, particularly in younger patients who are more susceptible to infectious complications. Future studies which compare these patterns across various immunosuppressive protocols are needed to determine the optimum immunosuppressive therapy.
We thank Philip Ruiz, MD, PhD and Casiana Fernandez-Bango for their assistance in describing the flow cytometry technique and Dr. Yonique Petgrave for her assistance with data collection.
None of the authors have any potential conflict of interest relative to the content of the report or the medications discussed therein.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Dr. Mariselis Rosa Sanchez contributed towards formulating the research design, data acquisition and organization and contributed to drafting the manuscript. Drs. Defreitas, Katsoufis Seeherunvong, Chen and Abitbol contributed in conceptualizing the research, and critically reviewing the manuscript. Drs. Burke and Ciancio were responsible for conceptualizing the dual induction protocol and critically appraising the manuscript. Dr. Chandar mentored Dr. Rosa and made substantial contributions in the concept and design of the study, organizing the data and preparing the manuscript.