Primary cardiac tumors are rare, and most are benign. Cardiac lymphangiomas are extremely rare, being most frequently diagnosed casually in asymptomatic patients or upon complications derived from compression. As in most benign tumors, the treatment is resection. We report the case of a 69-year-old female who debuts with congestive heart failure and is then diagnosed with a giant unresectable lymphangioma. The literature regarding the treatment of this tumor is scarce, to the best of our knowledge, especially if right coronary artery involvement is present. When the tumor is considered unresectable, cardiac transplantation may be considered as treatment.
Lymphangioma, Heart neoplasms, Heart transplantation
According to the 2015 World Health Organization classification, cardiac and pericardial tumors are classified into benign, malignant and of uncertain behavior. Primary cardiac tumors are rare, and approximately 70% of them are benign. Cardiac myxomas are the most frequent primary tumor in adults [1,2]. Cardiac lymphangiomas are extremely rare, usually being diagnosed casually in asymptomatic patients or when producing compression-related symptoms or complications. As with most benign tumors, the treatment is usually resection [3,4]. However, given its infiltration of cardiac structures, it can become unresectable, and alternative treatment strategies must be taken into consideration [5-7].
We present a case of a 69-year-old woman who was admitted because of new onset congestive heart failure, with dyspnea on minimal exertion. Echocardiography revealed an apparently extracardiac mass causing compression of right cardiac chambers, with constrictive physiology. Biventricular function was preserved, and no significant valve dysfunction was evident. Computed tomography confirmed the finding of a large, hypodense paracardiac mass measuring 15 × 12 × 10 cm, with predominantly peripheral punctate calcifications in its interior, being directly in contact with the right-sided cardiac chambers and resulting in their displacement and compression. The right coronary artery (RCA) was surrounded by the mass (Figure 1A). No other distant lesions were evident. Workup was complemented with magnetic resonance imaging, visualizing a large paracardiac, heterogeneous mass causing compression of the right cardiac chambers. Its signal was isointense in T1- and hyperintense in T2-weighted images, without contrast enhancement (Figure 1B). Upon the finding of an apparent plane between the mass and the cardiac tissues, preoperative workup was completed with a coronary angiography that showed normal coronary arteries, and the patient was scheduled for tumor resection surgery.
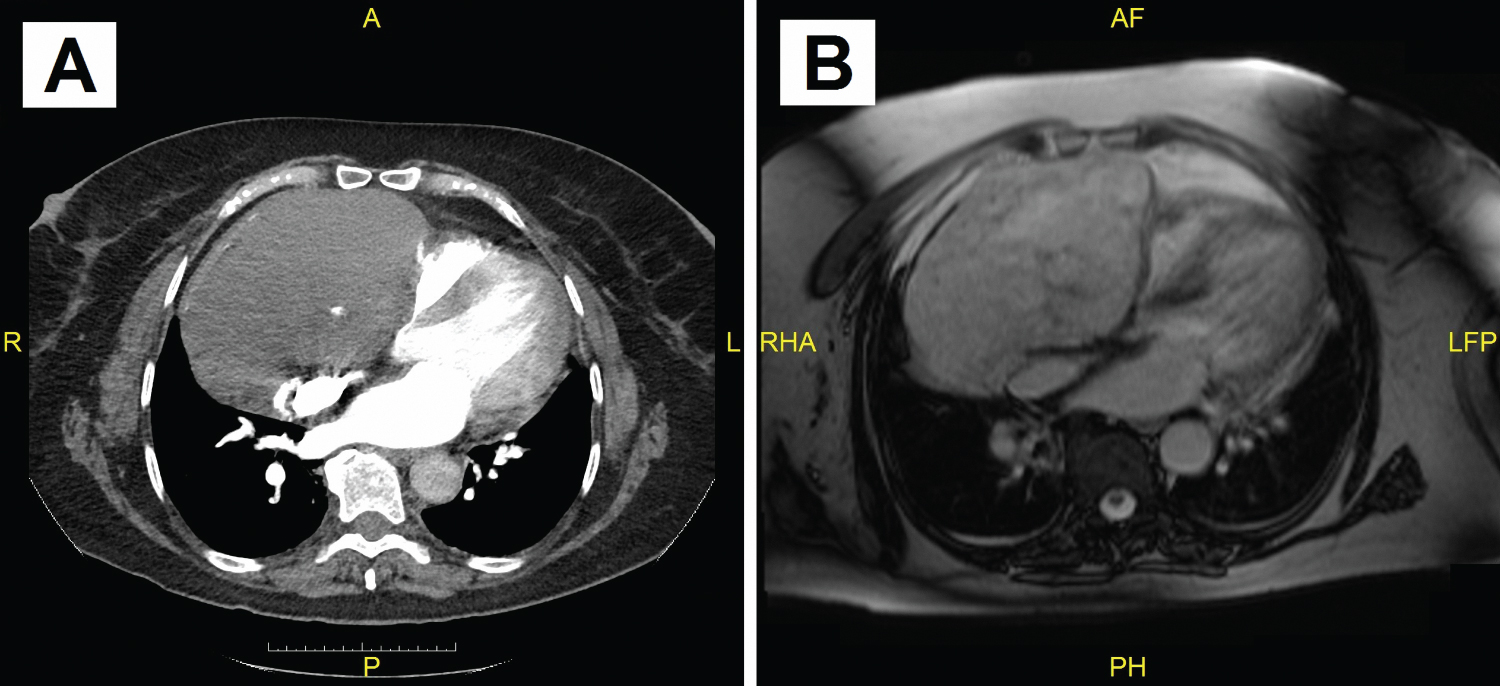 Figure 1: (A) Computed tomography imaging. Large, 15 × 12 × 10 cm - hypodense mass, intimately in contact with the right cardiac chambers with associated displacement and compression. The right coronary artery is surrounded by the mass; (B) Cardiac magnetic resonance imaging. Large, non-contrast-enhancing mass causing compression of the right cardiac chambers.
View Figure 1
Figure 1: (A) Computed tomography imaging. Large, 15 × 12 × 10 cm - hypodense mass, intimately in contact with the right cardiac chambers with associated displacement and compression. The right coronary artery is surrounded by the mass; (B) Cardiac magnetic resonance imaging. Large, non-contrast-enhancing mass causing compression of the right cardiac chambers.
View Figure 1
After sternotomy and pericardiotomy, the mass was observed to be adhered to the right atrium and ventricle, infiltrating said structures, as well as the right atrioventricular groove. It was heavily vascularized, bleeding upon minimal manipulation, and satellite extensions of the mass were evident in the diaphragmatic surface of the right ventricle. There was no evident macroscopic difference between the mass and normal cardiac tissue, with important infiltration of the myocardium, which made it technically impossible to resect without significant damage to cardiac structure, considering the RCA was surrounded by the mass. A sample was obtained and sent to Pathology for analysis. The tissue was described as parallel, fibrous bands with dilated, irregular vascular structures with a flattened epithelium that stained positive for CD31, D2-40 and ERG, with collagenous walls and smooth muscle fascicles, and lobules of adipose tissue. No mitoses or necrotic zones were evident. A diagnosis of lymphangioma was made, with no signs of malignancy. Due to the benign nature of the mass, with no extension at the time of diagnosis and no therapeutic alternatives for resection, her case was discussed in a multidisciplinary session, and cardiac transplantation was decided to be the optimal treatment.
Approximately one month after the initial intervention, a compatible cardiac donor was found, and she was subjected to bicaval orthotopic cardiac transplantation. Cardiectomy confirmed the tumor was unresectable, infiltrating the free walls of the right cardiac chambers and surrounding the RCA (Figure 2). The immediate postoperative period was marked by cardiogenic shock due to primary graft dysfunction, and circulatory assistance with venoarterial extracorporeal membrane oxygenation was required. She was successfully weaned off circulatory support on the fifth postoperative day. However, she later developed right lower lobe pneumonia and acute renal failure requiring renal replacement therapy. Due to the mentioned complications, she had a prolonged stay in the Surgical Intensive Care Unit but was able to slowly recover enough to be discharged to a hospital ward after four weeks. The first endomyocardial biopsy showed only mild cellular rejection. Follow-up echocardiography demonstrated preserved biventricular function. However, amidst the slow recovery, the patient presented with an episode of sudden, severe lower digestive tract hemorrhage that proved to be lethal despite blood derivative transfusions and invasive endoscopic measures.
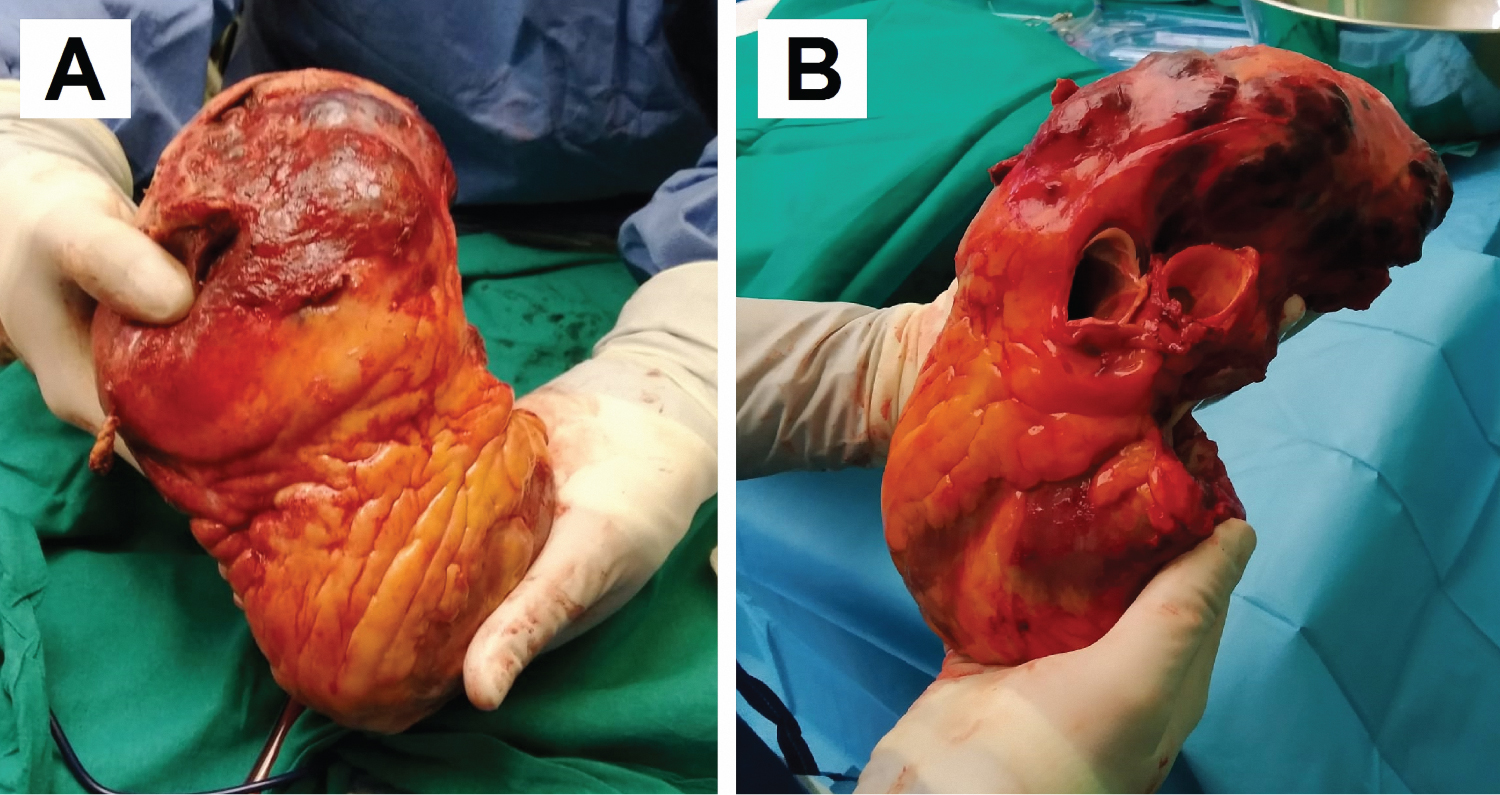 Figure 2: Heart and paracardiac mass after cardiectomy. The highly vascularized mass can be seen, with no clear delimitation between normal myocardium and tumoral tissue, involving the right cardiac chambers. (A) Anterior wall; (B) Lateral wall and great vessels.
View Figure 2
Figure 2: Heart and paracardiac mass after cardiectomy. The highly vascularized mass can be seen, with no clear delimitation between normal myocardium and tumoral tissue, involving the right cardiac chambers. (A) Anterior wall; (B) Lateral wall and great vessels.
View Figure 2
Primary cardiac tumors are unusual, and most of them are benign [1,2]. Primary cardiac lymphangiomas are extremely rare, usually being diagnosed casually in asymptomatic patients or when producing compression-related symptoms, as in this patient. Despite being benign, they can lead to dyspnea, cardiac tamponade, arrhythmias or chylopericardium. Most tumors are diagnosed in children or young adults, resulting from a proliferation of endothelium-covered lymphatic ducts. As in most benign tumors, the ideal treatment, whenever possible, is resection, given that an increase in tumor size can lead to complications [3,4]. However, in this case, given the evident infiltration of cardiac free walls and surrounding the RCA, the tumor was considered unresectable. To the best of our knowledge, this is the third case reported in the literature where the RCA is involved.
Proceeding with resection in this case, with the considerable involvement of the cardiac free walls and of the RCA, would have most likely led to significant morbidity and postoperative complications such as intractable bleeding after resection and severe right ventricular dysfunction, among others. Therefore, alternative treatment strategies had to be taken into consideration. Cardiac transplantation is a viable therapeutic alternative in patients with unresectable cardiac tumors, and has been described in benign tumors, as well as in malignant tumors such as sarcomas, when the spread is limited to the heart, although its role is still not wholly determined [5-7].
In conclusion, this is a rare case of a giant cardiac lymphangioma in an adult, with significant myocardial and coronary involvement, which proved to be unresectable. There are few cases published in the literature about the treatment of this tumor, especially when there is RCA involvement. Despite the fatal outcome due to an extracardiac complication, cardiac transplantation proved to be an optimal solution for the treatment of this patient with a rare, unresectable tumor.
All authors have contributed equally.
No potential conflicts exist.
No funding was provided.
Approved by the Hospital Universitario y Politécnico La Fe Ethics Committee.