Introduction: While obesity and age have historically limited potential living donors in the past, the points at which these factors could affect donor morbidity and mortality are unclear. We sought to identify any age and weight-based limitations for living donor for liver transplantation to expand the pool of potential donors
Methods: A retrospective review was performed using the UNOS Living donor database. Donors were compared on the basis of age and body-weight to the need for re-operation for complications. Re-admission rates were analyzed and were correlated with socio-economic factors, including insurance status and independent sources of income. A cross-sectional study was conducted to determine the level of OHP among 12-15 years old students in the selected Middle schools in Asmara. Data was collected from 572 study participants through structured interviews using a predetermined questionnaire. Pearson's chi-square test and multiple binary logistic regressions were used to analyze and infer the data.
Result: Of 3,539 donors included, 3.5% developed biliary complications, of whom 23 patients required re-operation; 43 in total required re-operation, including 6 for vascular complications. The mean age for those requiring re-operations for biliary complications was 34.9, and 60.8% of these patients were male. Mean body mass index was 25.3 kg/m2. 81.8% were insured, and 86.9% had an independent source of income. Analysis of BMI in donors requiring reoperation showed that there was no predilection for higher weight. Additionally, higher age did not predispose to complications, but was associated with a higher re-admission rate. Socio-economic factors do not predict serious complications for living donors.
Conclusions: Age and body mass index do not play a major role in the risk of donor biliary complications in the setting of living donor liver transplantation, though males appear to be more susceptible to these complications. More consideration should be given to older and more obese patients to increase access.
Liver transplantation, Living-donor transplantation, Donor pool expansion
Living donor liver transplantation (LDLT) has the potential to vastly increase the availability of organs for those who need them, though willing and able volunteers are often difficult to come by. In addition, the obesity epidemic continues to be a problem nationwide. In 2015-2016 prevalence of obesity among U.S. adults was 39.8%, and 1999-2000 through 2015-2016 saw a significant increase in childhood and adult obesity [1]. Aside from the many co-morbidities related to excess weight, it is also strongly associated with the development of hepatic steatosis [2], which could potentially affect graft function in LDLT. Moderate to severe donor hepatic steatosis also strongly increases the risk of poor graft survival in deceased donor liver transplantation (DDLT) [3]. Nevertheless, a clear negative association between donor BMI and LDLT graft survival has yet to be established. In addition, non-alcoholic steatohepatitis is rising as a primary indicator for liver transplantation, which could potentially decrease the size of the available donor pool while increasing need without implementation of expanded criteria donors (ECDs). Common definitions for ECDs include macrovascular steatosis and nonalcoholic fatty liver disease (NAFLD) [4]. It has been previously shown that LDLT from donor BMI ≥ 30 but ≤ 35 with no evidence of hepatic steatosis have similar outcomes from those of BMI < 30 [5], though it is still uncertain as to what outcomes transplant from donors who are BMI ≥ 35 and those with milder hepatic steatosis.
Younger donor age has also been associated with significantly higher recipient survival in patients receiving LDLTs [6], though increased demand for organs has also resulted in an increased use of older donors; 11.9% of US LDLT donors in 2014 donors were age 50-64 [6]. Though not proven, common thought regarding aging is that it reduces the overall organ resilience and makes them more susceptible to ischemia/reperfusion injury. Additionally, increased prevalence of steatosis in older livers can inhibit graft functioning [4] Multiple studies have shown and increased mortality and graft loss after transplantation from older donors, though [4] most have only evaluated age in the context of DDLT. Some reports, including. Kubota and colleagues [7] have found that that donors in their 20s have the lowest complication rates in LDLTs; whether this trend continues and worsens at the opposite end of the continuum as age increases is currently unknown.
We sought to identify age and weight-based limitations for living donor for liver transplantation to expand the pool of potential donors while avoiding complications associated with these co-morbidities.
The United Network for Organ Sharing (UNOS) Living Liver Donation database was queried retrospectively from October1987- January 2018 for a total of 3,539 patients that underwent a living liver donation, with any lobe or portion of liver; patients aged less than 14 years of age were excluded from analysis. Donors were then separated into groups and compared on the basis of age and body-weight to the need for re-operation for complications, with a focus on reoperative biliary, reoperative vascular/bleeding, and limited non-operative complications. Re-admission rates were analyzed and were correlated with socio-economic factors such as source of insurance and independent sources of income.
Descriptive statistical analysis, Student's t-test, and Chi Square testing were performed for continuous variables and integer comparison. Data was maintained and descriptive analyses were performed using an IBM SPSS 2018 database; (IBM, Armonk, NY, USA) Student's t-tests and Chi Square analyses were performed using GraphPad Prism 2018 (GraphPad Software, San Diego, CA). Statistical significance was accepted at p-values less than 0.05. Error bars are representative of means ± the standard error of the mean (SEM).
We first set out characterize the patients included in our study. 3,539 LDLT donors were captured from the database, as represented in (Table 1A). Mean age of the patients prior to segregation into different groups was 33.9 ± 10 years, while the BMI of the cohort was 28.2 ± 22.2. Males made up approximately 49% of the study population, while whites and Hispanics were the most common race within the study. A majority of patients were married (55%), employed, (82.5%) with access to health insurance (87.1%). The most common blood type was O (65.4%) followed by AO (26.9%).
Table 1: Living donor liver transplantation by demographics and complications. View Table 1
We first assessed overall management of the LDLT cohort and found an overall readmission rate of 7.1%. (Table 1B). Upon further investigation, the most common indications for readmission were non-specific complaints such as nausea, pain, constipation (n = 21) and unspecified reasons (n = 28) as illustrated in (Table 2). The overall complication rate requiring intervention aside from biliary or vascular complications was 7.2%. (Table 1C) The overall need for re-operation (all causes) was 1.9%, with the most frequent indication being biliary complications for the entire cohort. Biliary complications overall were 3.5%. of whom 23 patients required re-operation. 43 in total required re-operation, including 6 for vascular complications. Higher age did not predispose to operative complications, though it was associated with a higher rate of readmission (Figure 1A). No such relationship was found for BMI (Figure 1B).
Table 2: Most common indications for readmission in living donor liver patients. View Table 2
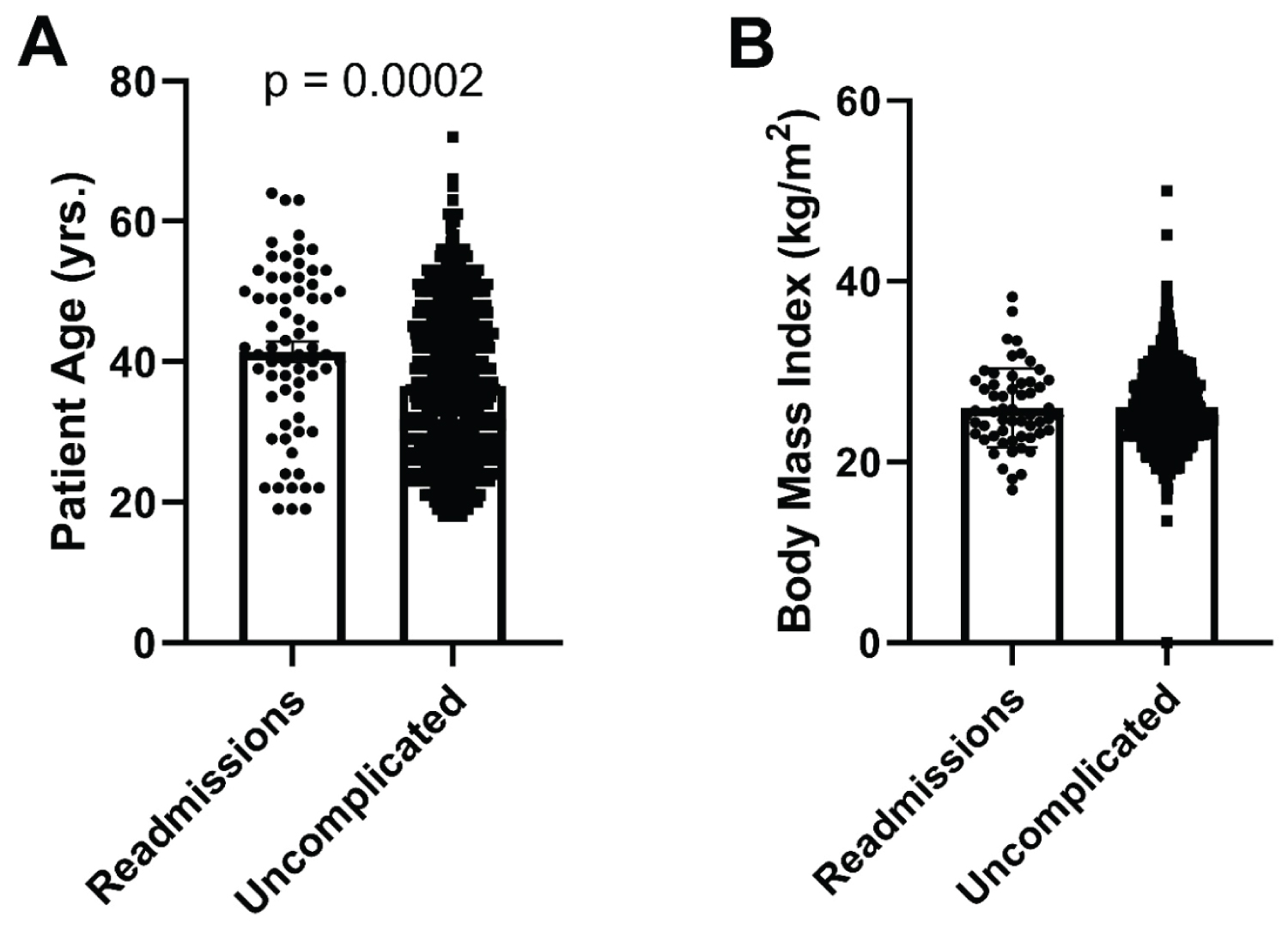 Figure 1: A) Readmissions by Age; B) Body Mass Index.
View Figure 1
Figure 1: A) Readmissions by Age; B) Body Mass Index.
View Figure 1
The mean age for those requiring re-operations for biliary complications was 34.9, and 60.8% of these patients were male as represented in (Table 1D). Mean body mass index was 25.3 kg/m2. 81.8% were insured, and 86.9% had an independent source of income. Analysis of BMI in donors requiring re-operation showed that there was no predilection for larger BMI, nor was the mean age of the patients requiring re-operation for biliary or vascular complications statistically higher, (Table 1D, Figure 2B and Figure 2C) though most patients included in the study with complications were less than or equal to 45 years of age (Figure 2A). When combining both BMI and age when looking at complication rates, no statistically significant association was found, though take backs for bleeding complications trended higher as both BMI and age increased concomitantly (Figure 3A). Readmissions were equally distributed across ages and BMI when combined (Figure 3B). Socio-economic factors such as health insurance status, employment, or marriage were not associated with increased re-operative complication rates (Table 1D).
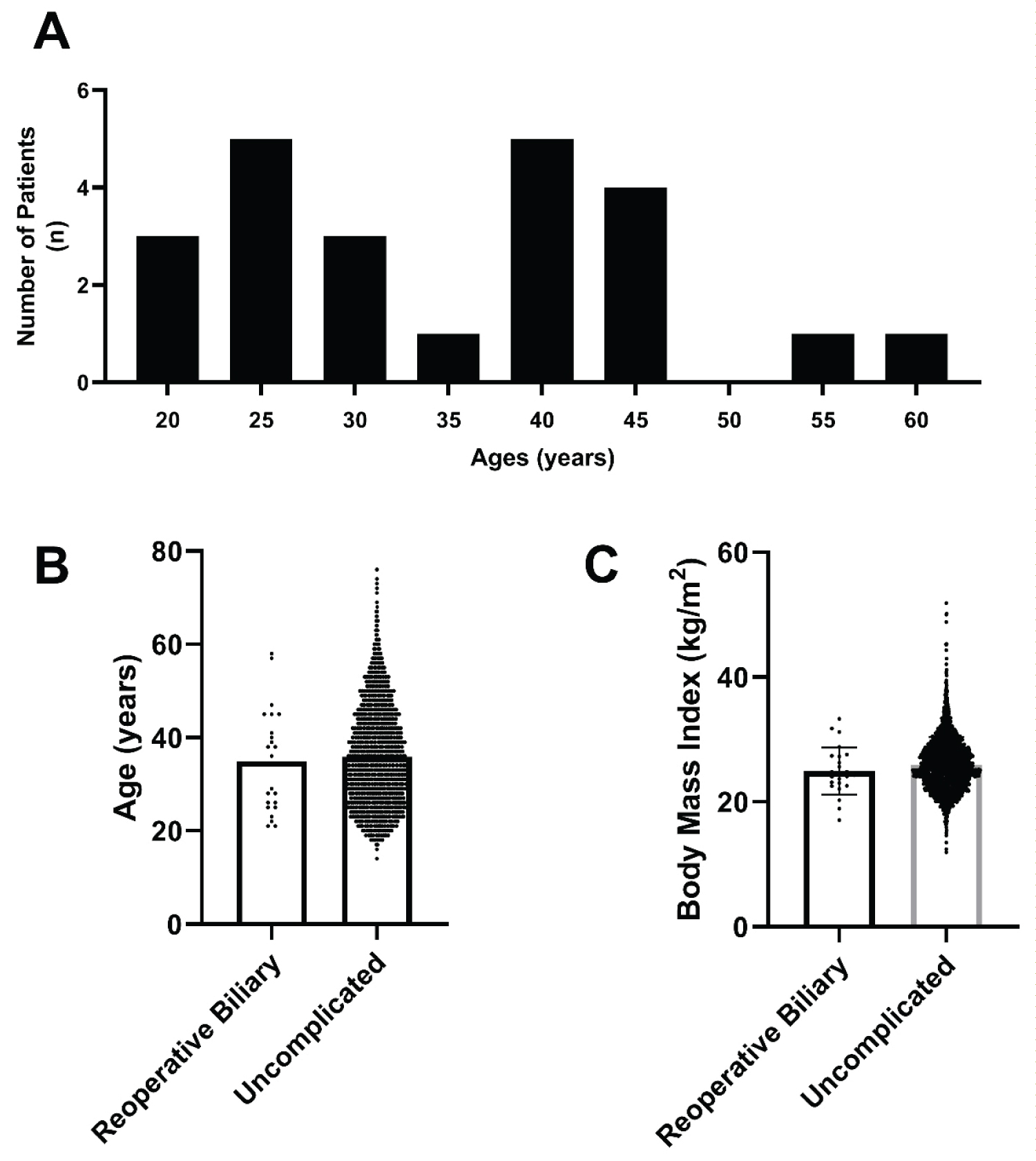 Figure 2: Age and BMI in relation to biliary complications. A) Histogram representation of biliary complications by age; B) Age distribution for uncomplicated and re-operative living donations; C) BMI distribution for uncomplicated and re-operative living donations.
View Figure 2
Figure 2: Age and BMI in relation to biliary complications. A) Histogram representation of biliary complications by age; B) Age distribution for uncomplicated and re-operative living donations; C) BMI distribution for uncomplicated and re-operative living donations.
View Figure 2
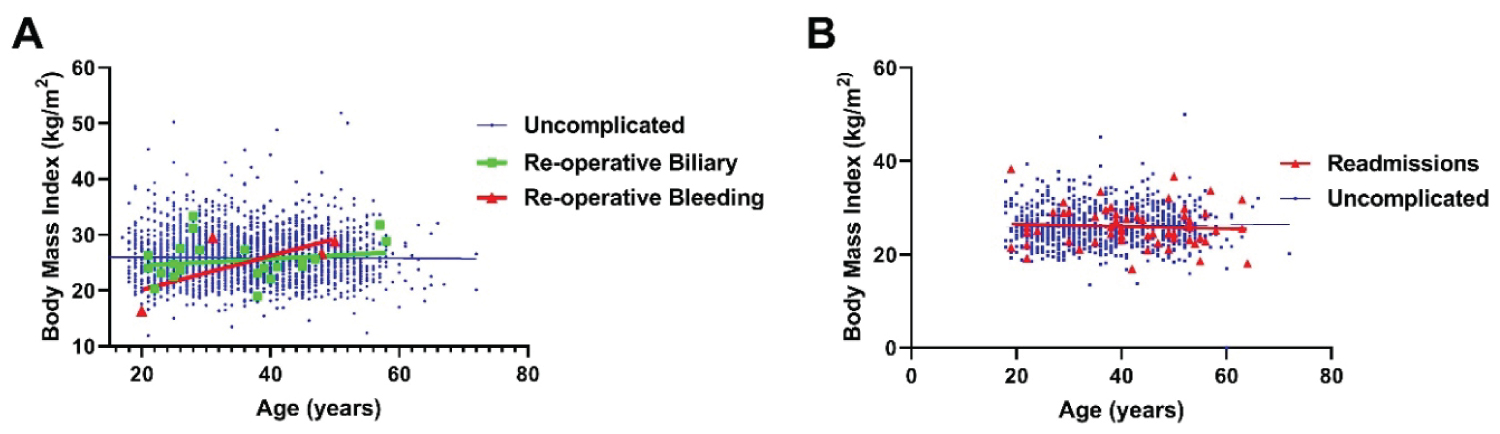 Figure 3: Complications by Age and BMI Combined. Re-operative complications by BMI and age. Readmissions by BMI and age.
View Figure 3
Figure 3: Complications by Age and BMI Combined. Re-operative complications by BMI and age. Readmissions by BMI and age.
View Figure 3
Identifying organs for liver transplantation can be difficult for a variety of reasons, aside from immune compatibility and regardless of whether or not living or deceased donors are used. Further complicating the issue, the ability to tolerate a liver resection is yet another consideration for patients wishing to make such a sacrifice. Generous living donors of either more advanced age or with higher body weights are often turned away, limiting a donor pool that is already stretched thin and unable to meet current demands [8]. Previous efforts to expand the donor pool have studied many potential sources, including immune compatibility, risk stratification, and others [8]. Previous studies have also alluded to worse graft functioning from older donors, though it doesn't necessarily affect overall outcomes; [9] in addition, there have also been reports documenting the use of older donor livers, though not yet nationally [10]. This recent, large study across institutions demonstrates that living liver donation can be done safely in these groups without increasing the risk of serious complications. Not surprisingly, older patients who donate their livers seem to be more prone to readmission, though the relationship is likely not borne out in increased major morbidity or mortality given the low-acuity nature of most of the re-admissions.
Because of the possible additive effect of age and weight in consideration of these potential complications, we sought to assess them synergistically; even in this context, the rates of biliary and vascular operative complications were not statistically significant, though a trend in reoperations for bleeding complications was observed as illustrated in (Figure 3). Though not significant, these findings are not unexpected given previous reports of the need for caution but ultimate safety of liver resection in elderly and obese patients [11,12]. We also looked to assess the rates of admission based on both weight and BMI combined, though there does not appear to be any particular clustering towards any extreme. This suggests that while readmissions are higher in older patients than the rest of the population, weight has no synergistic effect to this end. The most common reasons for readmission were non-specific complaints, which may be more indicative of an abundance of caution on the part of each transplantation program, though most re-admissions had multiple indications according to the registry.
Demographically, the study population included all major race classifications, though the majority was made up of whites and Hispanics in comparison to the other major ethnicities. Males were more susceptible to significant complications for reasons that are unclear at this time, and may be a new finding, though the relationship was not significant; male recipients of female livers have previously been shown to have higher rate of mortality, [13] though there is little data regarding male donors. A possible mechanism at this time is unclear, as other studies have indicated that females may actually have perioperative risk in association with liver resection [14].
This study has a number of important limitations. The UNOS registry is limited in that not all patients have data included, especially for more qualitative items such as readmission indication or obscure complications. In addition, we have purposefully limited the scope of this study, though it is very possible that both and BMI can put patients at risk for a wide variety of severe complications outside of need for reoperation, and there may be other risk factors worth looking at to better define the limits of safe living-donation. We are continuing to identify other potential expansion points from the available data to meet the significant levels of need in organ donation.
These findings suggest that age and body mass index do not play a major role in the risk of donor biliary complications in the setting of living donor liver transplantation, though males appear to be more susceptible to these complications, and age can be a risk-factor for re-admission. More consideration should be given to older and more obese patients in an effort to increase the availability of organs for those in need of liver transplantation.
The authors would like to thank John Behrend, PA-C, and all those at Temple University Hospital who make this work possible.
The authors declare no conflicts of interest. This work has been submitted to the Academic Surgical Congress Conference, 2019.
This study was supported by the Abdominal Organ Transplant Program at Temple University Hospital.
This study was approved by the Institutional Review Board at Temple University and was performed in accordance with the Code of Ethics of the World Medical Association.
P.E.M. designed the study and wrote the manuscript. S.K. performed a literature review and offered critical feedback on the manuscript. R.S.R. and C.C. performed the statistical analyses detailed here. A.D., K.L., and A.D.C. offered critical feedback on the manuscript. S.S.K. designed the study, oversaw the project and critically revised the manuscript.
Transplantation/Immunology.
This work was submitted to and approved by the Human Research Protection Program / Institutional Review Board at Temple University.