Phosphorus is an essential macronutrient, various functions at the cellular level, it has signals in metabolic pathways and is involved in the production of cellular energy. In grade 3 to 5 kidney disease, the patient suffers alterations in the homeostasis of calcium, phosphorus secondary to dysregulation of FGF 23 (Fibroblast growth factor) and PTH (paratohormone), increasing the risk of vascular calcification, in kidney transplantation, even the levels of FGF 23 and PTH can remain elevated for several months. Several patients post-kidney transplant have hypophosphatemia, due to the high levels of phosphaturic hormones. The objective of this study is to demonstrate that patients who decrease serum phosphorus in early kidney transplantation are associated with good kidney outcomes.
Observational prospective single-center study, 39 patients were studied, who underwent a kidney transplant in the period from January 2018 to March 2019, at the Guadalajara Fray Antonio Alcalde civil hospital, the patients underwent kidney transplantation from a related living donor or brain death donor, two groups were defined according to the serum phosphorus at patient discharge, group A was defined with phosphorus levels < 3.5 mg/dl , Group B was defined with levels greater than or equal to 3.5 mg/dl. The main outcome was eGFR at discharge using the CKD-EPI formula, measuring daily serum creatinine levels until discharge, secondary outcomes: Hospital days, delayed graft function, the data analysis of the quantitative variables the Mann-Whitney U test was used to compare the non-parametric means of group A vs. B, the categorical variables the Pearson chi-square test was used, obtaining a statistical significance value ( p < 0.05). A roc curve was performed to determine the sensitivity and specificity of the phosphorus levels and the relationship with the eGFR.
In the comparison of means using the Man Whitney U test of groups A and B (Table 2), days of hospitalization, patients in group A had fewer days hospitalized 4.9 (IQR 4-5.7) compared to group B 6.4 (IQR 4.5-8.5) (p = 0.04), creatinine levels at patient discharge, patients in the group with phosphorus less than 3.5 mg/dl had a mean of 1.2 mg/dl (IQR 0.7-1.2) in contrast to the group B with a mean of 3.4 mg/dl (IQR 1.5-4.2) (p < 0.001), the estimated glomerular filtration rate in group A performed much better with a mean of 91.7 ml/min (IQR 77-112) compared to group B a mean eGFR 40.2 ml/min (IQR 16-56) (p < 0.001) at discharge, the patients in group A had much more urine volume at discharge compared to those in group B, 3707 ml (IQR 2950-4465), 2011 ml (IQR 0-3385) (p = 0.03) respectively.
Table 1: Baseline characteristics. View Table 1
Post-kidney transplant hypophosphatemia is related that patients have better kidney function, reflected in eGFR, so this may be a good biomarker to predict adequate kidney function in early kidney transplantation.
Phosphorus is an essential macronutrient, it has several functions at the cellular level, signaling in metabolic pathways and is involved in cellular energy production, phosphorus homeostasis is complex and widely studied, phosphate in the kidney is freely filtered through the glomerulus and is reabsorbed via sodium/phosphate cotransporters type 2 (NaPi-2a and NaPi-2c), which are expressed on the luminal side of proximal tubule epithelial cells. Phosphate reabsorption in the kidney is related to parathyroid hormone (PTH) and FGF-23 (fibroblast growth factor), being these phosphaturic hormones, as well as the cause of bone mineral disease in chronic kidney disease and from decreased synthesis of vitamin D [1-4].
Kidney disease grade 3 to 5, the patient suffers alterations in the homeostasis of calcium, phosphorus secondary to dysregulation of FGF 23 and PTH, increasing the risk of vascular calcification and cardiac mortality in patients with chronic kidney disease [5,6], in kidney transplantation, even the levels of FGF-23 and PTH can remain elevated for several months [7]. A large part of the patients after the transplant have hypophosphatemia, due to the high levels of the phosphaturic hormones (PTH and FGF 23) [8,9], calcineurin inhibitors such as cyclosporine have shown decreased expression of the sodium-phosphorus cotransporter in the proximal tubule in rats, mTOR inhibitors, including everolimus, also cause hypophosphatemia and metabolic acidosis [10-12].
The objective of this study is to demonstrate that patients who decrease serum phosphorus in early kidney transplantation are associated with good kidney outcomes.
Observational prospective single-center study, 39 patients were studied, who underwent a kidney transplant in the period from January 2018 to March 2019, at the Guadalajara Fray Antonio Alcalde civil hospital, the entire study procedure was carried out according to the statements from Helsinki and Istanbul, the patients underwent kidney transplantation from a related living donor or brain death donor: Two groups were defined according to the serum phosphorus at patient discharge, group A was defined with phosphorus levels < 3.5 mg/dl, Group B was defined with levels greater than or equal to 3.5 mg/dl, the normal phosphorus level was taken as reference with reference to the KDIGO guidelines in patients with CKD grade 4 and 5 [3], the measurement of serum phosphorus levels from the first day of hospitalization until the patient's discharge, all patients were induced with thymoglobulin and a regimen of prednisone, mycophenolic acid, and tacrolimus.
The main outcome was eGFR at discharge using the CKD-EPI formula [13], measuring daily serum creatinine levels until discharge, secondary outcomes, hospital days, delayed graft function defined as the need for dialysis in the first week of transplantation [14].
The data were collected on the days that the early kidney transplant patients were hospitalized. Prior to the kidney transplant, studies of hemoglobin, creatinine, urea, and serum electrolytes were taken, taking these as baseline values and these blood tests were performed after the kidney transplant. Blood test were taken every day of the hospital stay until the patient's discharge, for the division of the two groups of studies, the serum phosphorus levels were taken into account at the patient's discharge, however daily phosphorus monitoring was performed.
Prospective observational study of 39 kidney transplant recipients, the distribution of variables using the Shapiro-Wilk test, quantitative variables that are not normally distributed are presented as mean (first to third quartiles), categorical variables are presented in percentages, in the data analysis of the quantitative variables, the Mann-Whitney U test was used to compare the non-parametric means of group A vs. B, of the categorical variables, the Pearson chi-square test was used, obtaining a statistically singular value (p < 0.05). Auroc curve was performed to determine the sensitivity and specificity of the phosphorus levels and the relationship with the eGFR.
All statistical analysis was performed using SPSS software, version 22.0 for MacOs (IBM, Armonk, NY) and Excel Microsoft Office for MacOs.
According to the general baseline characteristics of the patients (Table 1), a total of 39 patients with early kidney transplantation were analyzed, per group there were a total of patients: group A = 28(71.8%) and group B = 11(28.2%). 76.9% were male, mean age was 29.5 years (IQR 22-36), 97.4% had a history of being on dialysis therapy prior to transplantation, 69.2% on HD and 28.2% on PD, with a mean total time in renal replacement therapy of 37 months (IQR 11.7-48), 51.3% of the patients had residual uresis at the time of transplantation, laboratory studies prior to transplantation, Hb 11 g/dl (IQR 9.6-12.3), Serum glucose 91.9 mg/dl (IQR 82.7-97), Urea 136 mg/dl (IQR 99.6-171), Serum creatinine 12.9 mg/dl (IQR 9.5-16.7), Serum sodium 136 mg/dl (IQR 134-138), serum potassium 4.8 (IQR 4.1-5.4), Calcium 8.9 mg/dl (IQR 8.3-7.1), in group A serum phosphorus levels had a mean of 5.6 mg/dl (IQR 3.5-7), group B of 5.9 mg/dl (IQR 4.5-5.4), In the events associated with the transplant, 46.2% were from a brain death donor that was diagnosed by a cerebral angiotomography study, 53.8% were from a living donor.
Table 2: Outcomes after kidney transplantation. View Table 2
The means comparation using the Man Whitney U test between groups A and B (Table 2), days of hospitalization, patients in group A had fewer days hospitalized 4.9 (IQR 4-5.7) compared to group B 6.4 (IQR 4.5-8.5) (p = 0.04), creatinine levels at patient discharge, patients in the group with phosphorus less than 3.5 mg/dl had a mean of 1.2 mg/dl (IQR 0.7-1.2) in contrast to the group B with a mean of 3.4 mg/dl (IQR 1.5-4.2) (p < 0.001), the estimated glomerular filtration rate in group A performed much better with a mean of 91.7 ml/min (IQR 77-112) compared to group A. group B a mean eGFR 40.2 ml/min (IQR 16-56) (p < 0.001) at discharge, the patients in group A had much more urine volume at discharge compared to those in group B, 3707 ml (IQR 2950-4465), 2011 ml (IQR 0-3385) (p = 0.03) respectively, in the variable of delayed function of the graft in the comparison using the chi-square test, group A presented: 2 patients (7.1%) and g Group B presented: 5 patients (45.5%) (P = 0.003), the rest of the outcomes at discharge such as hemoglobin, glucose, urea, sodium and serum potassium, there was no statistical significance in the comparison of means in the two groups (P > 0.05), in the graphs of daily monitoring of creatinine and phosphorus levels in both groups, a trend is evident in patients in which phosphorus levels decrease as the days go by and is correlated to serum creatinine levels (Figure 1). The roc curve was performed with the aim of determining the specificity and sensitivity of serum phosphorus (blue line) to predict eGFR greater than 60 ml/min, AUC 0.76 (0.7-0.9) (serum phosphorus cohort 3.1 mg/dl) (p =< 0.001) (Figure 2).
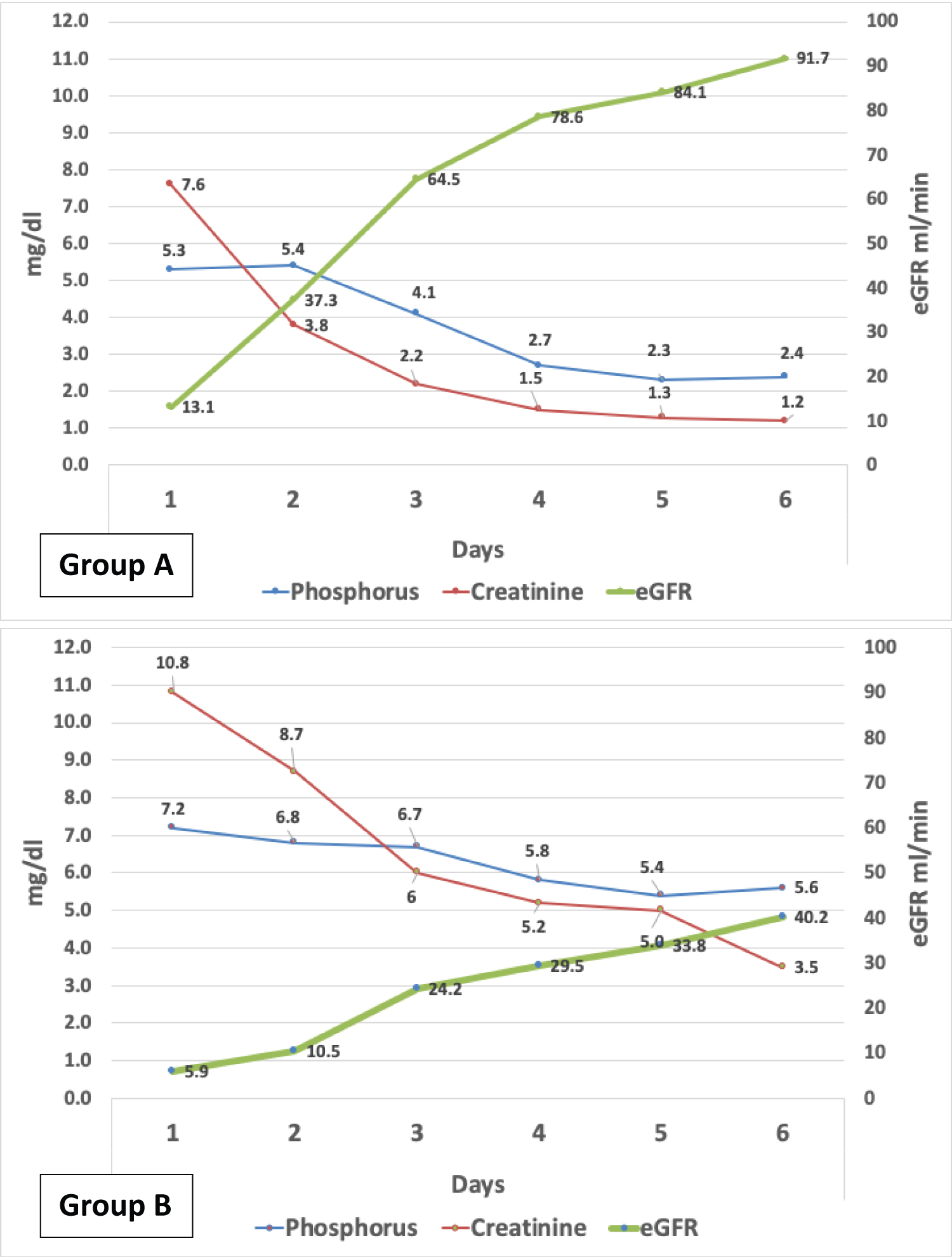 Figure 1: Daily monitoring of creatinine, phosphorus levels and eGFR (mean).
View Figure 1
Figure 1: Daily monitoring of creatinine, phosphorus levels and eGFR (mean).
View Figure 1
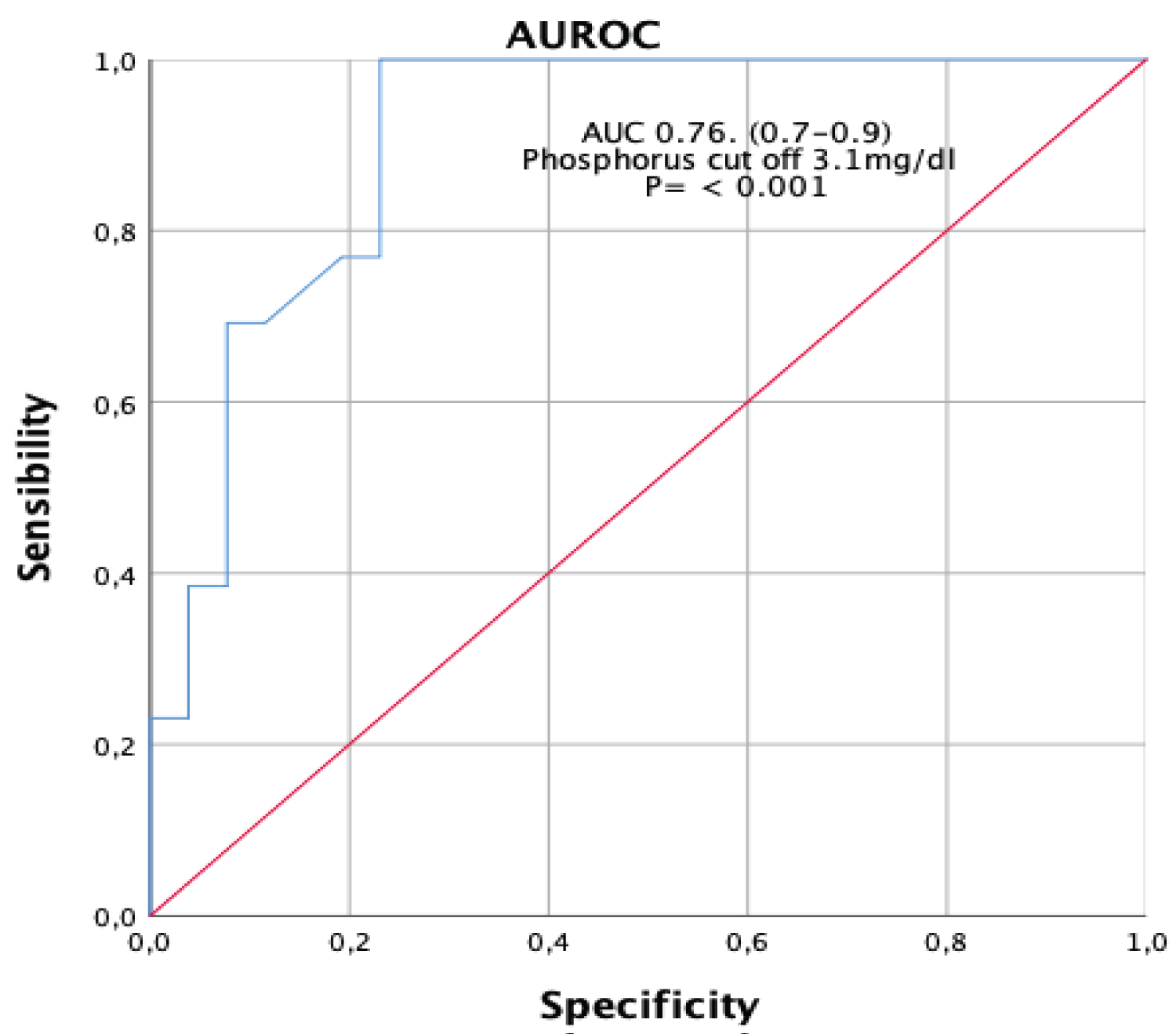 Figure 2: Graph 2. Serum phosphorus (blue line) to predict eGFR greater than 60 ml/min (red line).
View Figure 2
Figure 2: Graph 2. Serum phosphorus (blue line) to predict eGFR greater than 60 ml/min (red line).
View Figure 2
Kidney transplant patients may have hydroelectrolytic changes during their evolution, in most cases they are related to serum phosphorus levels. In our study we found that patients with phosphorus levels below 3.5 mg/dl have a better evolution in eGFR and serum creatinine at discharge, even these patients had fewer days of hospital stay.
Previous studies have assessed phosphorus alterations in kidney transplant patients and have been associated with good renal function decline. In our study, a progressive decrease in phosphorus levels was observed in the days after the transplant and it was observed that the patients who had levels below 3.5 mg/dl at discharge had a better eGFR, similar studies are consistent with these results [15], Marco van Londen, et al., in a longitudinal observational study, evaluated 957 patients with kidney transplantation and the Patients who had hypophosphatemia were favorably associated with less graft dysfunction in the first year after transplantation, and it was not associated with greater cardiovascular death [16]. Maximilian R. Ralston, et al. in an observational study, demonstrated that phosphorus levels from 0.3 to 0.69 mmol/l is related to less delayed graft function [17], these data are similar to our results.
Our hypothesis is that patients with low levels of phosphorus in the immediate transplant and who show a good evolution in relation to serum creatinine levels and eGFR is associated with the fact that the renal graft has a functional renal parenchyma with expression of the receptors of PTH and klotho in the proximal tubule, coupled with the fact that most patients with chronic kidney disease have elevated levels of FGF 23 prior to their transplantation and favor the excretion of phosphorus in the urine, Andrea Trombetti, et al. in a study In a prospective observational study with 69 transplant patients, 62% presented hypophosphatemia in the first 12 days and this was related to high levels of FGF23 [8], parathormone (PTH) also plays an important role in phosphorus regulation and is associated with the internalization of type 2 Na/Pi receptor in the proximal tubule [18,19], however, patients whose hyperphosphatemia persists even after renal transplantation present less renal function and we consider that the graft has less functioning tubules.
Patients who present a decrease in phosphorus after transplantation is related to the fact that these patients have better renal function than those who maintained normal levels of phosphorus or hyperphosphatemia, so this may be a good biomarker for predicting adequate kidney function in early kidney transplantation.
Weaknesses of the study: we consider that the study population is small, it was not possible to measure basal levels of iPTH to detect hyperparathyroidism because due to lack of medical supplies.
There is no interest conflict on the part of the authors in the preparation of this article.
Not applicable.
DMB, MJC, MCO and ALB conceived and designed the study. DMB performed the analyses. ENR and CFC contributed to data acquisition and interpretation. ALB and MJC wrote the manuscript with the help MCV. All authors contributed to the discussion, review, and approval of the final manuscript.