To study and compare the association between estimated GFR with cystatin-C and serum creatinine and the lipid profile in chronic kidney disease.
Chronic kidney disease (CKD) is frequently complicated by the coexistence of cardiovascular (CV) events, making it essential to identify CV risk in CKD. Serum cystatin-C is an upcoming renal biomarker, which is used to measure estimated glomerular filtration rate (eGFR) by the CKD-EPI formula.
This cross-sectional study, comprising of 120 CKD patients, attempted to determine, which of the two equations for estimating GFR, either by serum cystatin-C or by serum creatinine, is better related with lipid profile which is widely portrayed as a cardiovascular risk factor. The parameters evaluated included lipid profile, serum creatinine and serum cystatin-C among others. Staging was done by both the equations (MDRD equation by creatinine and CKD-EPI equation by cystatin-C) and compared, and both the eGFRs were correlated with the lipid profile.
eGFR estimation by cystatin-C was found to relate inversely and significantly with lipid profile which included-TC, TG, LDL, VLDL (r = -0.19, -0.23, -0.18, -0.23; p < 0.05 respectively) and lipid ratios TC/HDL, LDL/HDL (r = -0.26, -0.24; p < 0.01 respectively). Lipid profile except HDL was found to correlate negatively and significantly with eGFR estimation by serum cystatin-C (p < 0.05). Lipid ratios- TC/HDL and LDL/HDL were also found to correlate inversely and significantly (p < 0.01). However, eGFR using serum creatinine failed to offer a similar significant relation.
Serum cystatin-C based eGFR was found to be better correlated with the lipid profile, when compared with eGFR estimation using serum creatinine. Hence, the correlation between cystatin-C based eGFR and lipids might indicate that this eGFR methodology may be a better marker of cardiovascular risk as lipids are a well known traditional risk factor for cardiovascular disease.!
Cystatin C, Renal insufficiency, Estimated glomerular filtration rate, MDRD equation, CKD-EPI equation, Cardio-renal disease, Cardiovascular risk, Lipid profile
Chronic kidney disease (CKD) is a world-wide health problem whose burden continues to increase. CKD encompasses a spectrum of different pathophysiologic processes, associated with abnormal kidney function and a progressive decline in glomerular filtration rate (GFR). The National Kidney Foundation had provided a classification for chronic kidney diseases, which has since evolved through time. This staging of chronic kidney disease, as delineated by the Kidney Dialysis Outcomes Quality Initiative (KDOQI), depends on the estimated glomerular filtration rate (eGFR) [1].
CKD is defined using eGFR as the presence of evidence of kidney damage with an abnormal GFR for at least 3 months or by a GFR below '60 ml/min/1.73 m2, body surface area [2]. Serum creatinine is the most commonly used marker for eGFR using the Cockcroft-Gault formula or the MDRD (Modification of Diet in Renal Disease) [3]. However, creatinine is an unstable entity and has wide variance. Even though it is still most widely used in practice, newer markers are under study, with cystatin-C being a popular entity [4]. Cystatin-C is a recent biomarker which has been noted to be a better marker than creatinine in certain studies [5]. It is a 13 kDa basic protein of the cysteine proteinase inhibitor super family and is synthesized by all nucleated cells at a constant rate with relatively lesser factors affecting it than serum creatinine; making it a more reliable biomarker [6]. According to multiple studies, production of cystatin-C remains unaltered by inflammatory processes, muscle mass, age or gender [7-9].
Cystatin-C has been found to have a link to cardiovascular factors as well as in metabolic syndrome, which throws light into its deeper relation with the pathology of these disorders as also the multiple advantages it possesses over other markers as a clinical tool and not only as a plain renal maker [10-14]. Higher cystatin-C levels were found to be associated with greater cardiovascular disease (CVD) mortality and morbidity, probably due to an involvement with endothelial damage [15].
Cystatin-C was found to be elevated in patients with CVD risk factors without the evidence of CKD which makes cystatin-C a potential independent biomarker of CVD [16,17]. Cardiovascular disease is an important cause of morbidity and mortality in all stages of CKD. CVD events in CKD patients commonly include ischemic vascular disease, cardiac failure, hypertension and left ventricular hypertrophy [18]. While the reverse-CKD being a high-risk factor for development or deterioration of cardiovascular conditions also stands true [19]. Cystatin-C was found to detect even a slight decline in renal function, while serum creatinine exhibited no such quality [20].
The link of eGFR estimation by serum cystatin-C and the occurrence of CVD among CKD patients have hardly been researched. In this study the association between estimated GFR with cystatin-C and serum creatinine based on lipid profile as a cardio vascular risk factor in chronic kidney disease, were compared. This would also assist in determination of the better estimated GFR parameter, thereby, bringing forth a better biomarker for both diagnosis of chronic kidney disease and for presence of cardiovascular disease.
This was a cross-sectional study which was conducted at the Sri Manakula Vinayagar Medical College and Hospital, Puducherry, South India, with patients drawn from the rural areas in and around Puducherry. Patients aged above 20 years of age presenting to the Nephrology Department (OP and IP), and of both genders who were diagnosed with CKD, and were not part of the exclusion criteria, were assessed after getting informed consent. The exclusion criteria used were for those CKD patients associated with pregnancy, thyroid disorders, steroid therapy, Alzheimer's disease, HIV infection, patients undergoing chemotherapy, smokers and any subject who was diagnosed to have chronic kidney disease but refused to give informed consent. The study consisted of 120 patients. The KDIGO staging, which is used commonly by clinicians, was applied [21].
The sample size was calculated using the overall prevalence of 46% of cardiovascular disease in chronic kidney disease, reported by Levin, et al. [21] and 80% power at 95% confidence interval with a precision of 20% and was found to be 118. And rounding it off, we assumed a sample size of 120 for our study.
After taking informed and written consent, a thorough history was taken, and previous records if any were examined A general clinical examination was done including pulse rate, and Blood Pressure was measured in sitting position, using an Aneroid Sphygmomanometer (duly calibrated) with an average of 3 readings using the JNC-8 Criteria [22].
After taking each patient's permission and taking informed consent, 3 ml of blood was drawn under strict aseptic precautions, for the purpose of investigations and collected in glass test tubes which were duly labelled. Serum separation was done by centrifugation at 2500 rpm for 5 min. All the Investigations like fasting serum glucose, fasting lipid profile, urea, creatinine and serum cystatin-C were done at the fully accredited Laboratory of the Sri Manakula Vinayagar Medical College and Hospital, Madagadipet, Puducherry, India. The parameters studied included serum urea, serum creatinine, fasting serum glucose, glycated haemoglobin (HbA1c) and lipid profile derived from serum- total cholesterol (TC), triglycerides (TG), high density lipoprotein cholesterol (HDL), low density lipoprotein cholesterol (LDL), very low-density lipoprotein cholesterol (VLDL) and haemoglobin. Analysis was done using Roche Cobas Mira plus Automated Chemistry Analyser (made in USA).
The total cholesterol, triglycerides, HDL, serum creatinine and serum urea were estimated by calorimetric method using automated chemical analyser. Friedwald's formula was used to derive LDL. Serum cystatin-C estimation: Measurement of serum cystatin-C was done by using the Quantia-Cystatin-C kit, by Tulip diagnostics and measured by MICROLAB 300 Semi-auto-analyser.
Descriptive data was expressed in proportions (percentages) and mean ± SD. Correlation analysis was done by using Pearson's method. One way analysis of variance (ANOVA) test in SSPS package was done to determine the significance of each group. The ANOVA is an Omnibus test statistic and cannot tell which specific groups were statistically different from each other. Hence the POST HOC test was done to determine which groups differed further from each other. Post hoc analysis was done by applying Dunnett's 2 sided test for comparison within the groups. A p value of < 0.05 was considered significant. Analysis of quantitative and qualitative data: All the data was entered and analyzed using Epilate Manager Software (version 4.2, EpiData Association, Odense, Denmark): SPSS statistical package version 24 (SPSS Inc, Chicago, IL) and Microsoft excel 2010 which was also used to generate graphs and tables.
eGFR by MDRD study equation using serum creatinine [21]:
eGFR = 175 × standard SCr-1.154 × age-0.203 (males)
eGFR = 175 × standard SCr-1.154 × age-0.203 × 0.742 (females)
eGFR by CKD-EPI equation using serum cystatin-C [21]:
CKD-EPI equation adjusted for age, sex:
eGFR = 127.7 × CysC-1.17 × age-0.13 (males)
eGFR = 127.7 × CysC-1.17 × age-0.13 × 0.91 (females)
Based on eGFR, all CKD patients were divided into five stages, as per KDIGO 2012 guidelines.
This study was reviewed by the research committee and was cleared by the Institutional Ethics Board of the Sri Manakula Vinayagar Medical College and Hospital, Madagadipet, Puducherry, India, and the clearances were obtained prior to the commencement of the study.
The total number of subjects studied was 120. The age of the subjects ranged from 27-90 years, with an average of 56.30 ± 12.38 years. Out of the 120 subjects, 84 subjects were male while 36 were female. 34.2% (41) of patients were undergoing hemodialysis for duration of 0-24 months with an average of 2.72 ± 5.57 months.
The duration of CKD in this population ranged from 0-72 months with an average of 8.63 ± 14.83 months. 34.2% (41) of patients were undergoing hemodialysis for a duration of 0-24 months with an average of 2.72 ± 5.57 months.
The presence of diabetes alone, was found in 10 (8%) patients, hypertension only was found in 34 (28%) patients, while both hypertension and diabetes were found in 33 (28%) subjects. No diabetes or hypertension was present in 43 patients (35.8%) as shown in Figure 1. The mean cystatin values were higher in the males as compared with the females and were higher for the older groups of people.
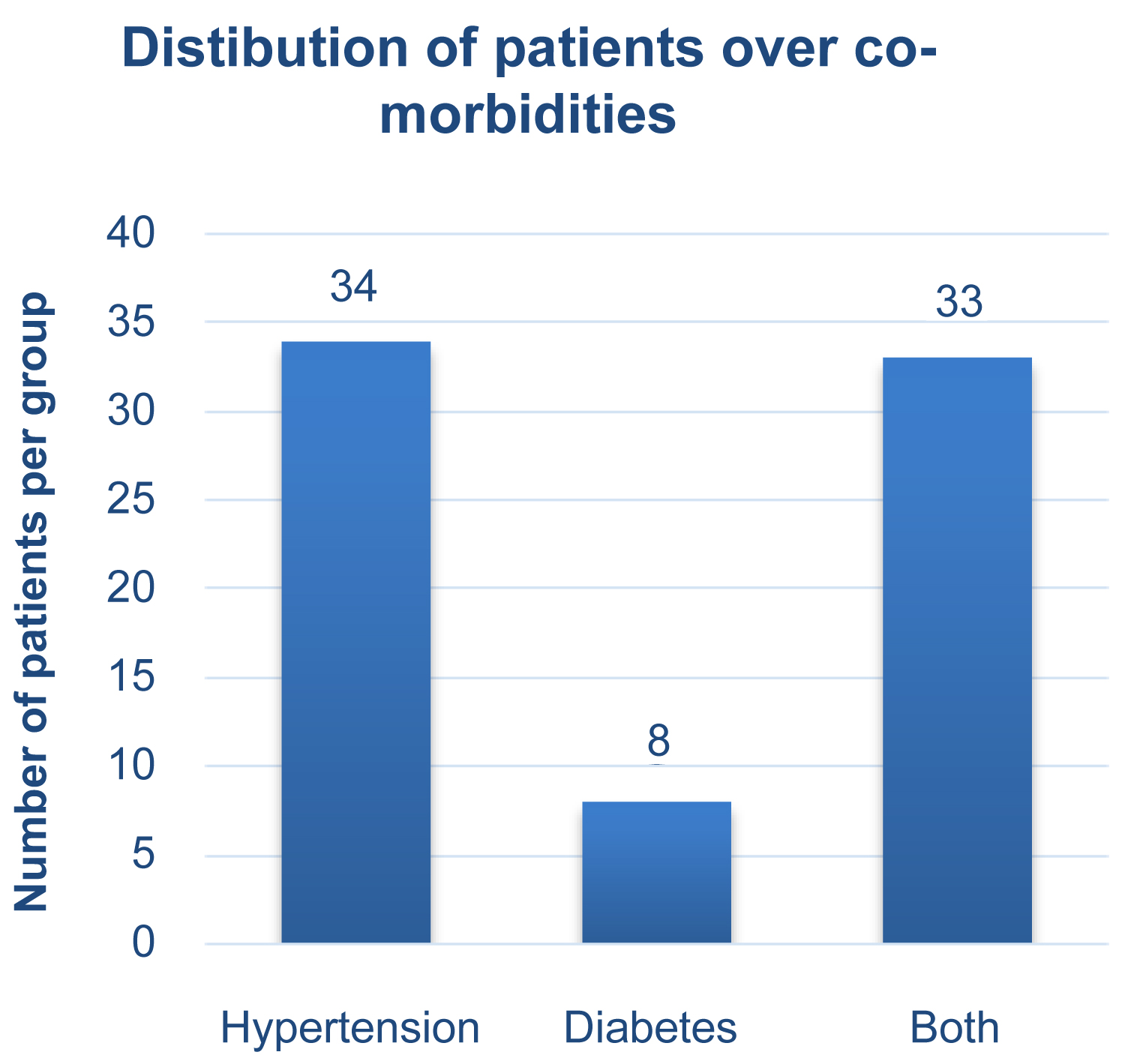 Figure 1: Distribution of patients over co-morbidities.
View Figure 1
Figure 1: Distribution of patients over co-morbidities.
View Figure 1
For each patient, estimated GFR was calculated by both MDRD formula, using serum creatinine and CKD-EPI formula using serum cystatin-C. The patients were distributed according to the latest KDIGO guidelines and were categorized over stages 1, 2, 3a, 3b, 4 and 5. Stage 1 patients were not a part of this study due to lack of subjects in that stage.
Table 1 provides the mean ± SD for serum creatinine and serum cystatin-C of the study population and the eGFR using both these parameters.
Table 1: Patients in each CKD stage and their eGFR by MDRD and CKD-EPI equations. View Table 1
It was noted that the use of CKD-EPI equation showed a higher number of patients in advanced stages, as compared to the staging by the MDRD equation. Where only 57 patients were considered as stage 5 by MDRD equation, a much higher number, 71 were part of stage 5 according to CKD-EPI equation. Similar findings were noted in all stages, as mentioned in the table.
Table 2 depicts serum creatinine, serum cystatin-C and lipid profile of the study population. Both FBS and HbA1c were also found to be elevated at an average. Lipid profile showed mild elevations as well.
Table 2: Concentration of renal markers, glycemic status and lipid levels. View Table 2
As can be seen in Table 3, our findings showed that a significantly negative correlation exists between total cholesterol, triglycerides, low density lipoprotein and very low-density lipoproteins and eGFR estimation by cystatin-C, while the ratios TC/HDL and LDL/HDL showed a highly significant inverse relation with eGFR estimation by cystatin-C. Meanwhile, eGFR estimation by serum creatinine did not reveal a significant correlation with these parameters.
Table 3: Correlation between lipid profile and eGFR by cystatin-C and creatinine. View Table 3
Table 4 depicts the duration of disease and the duration of dialysis in patients under hemodialysis correlated negatively and significantly with both eGFRs. Hemoglobin levels are also shown in the tables which were found to have a significant positive correlation with both eGFRs, conforming to the fact that with deteriorating GFR, anemia sets in.
Table 4: Correlation between other factors and eGFRs by both equations. View Table 4
CKD is a chronic, non-communicable condition presenting with a wide variety of signs and symptoms. The staging of CKD requires laboratory measurement of traditional renal markers like serum creatinine. Serum cystatin-C is also a marker of glomerular filtration rate and can be used for staging of CKD. This study attempted to evaluate which of the two aforementioned renal markers correlates better with the lipid profile in CKD patients at different stages.
The values of serum creatinine and serum cystatin C were found to be elevated, as would be expected in the CKD patients. Total cholesterol, LDL cholesterol and VLDL cholesterol was observed to be within desirable limits, on an average. Elevated levels of triglycerides and the lipoprotein ratios of TC/HDL and LDL/HDL were found. Another important finding was HDL concentrations being lower than the reference range. A significant negative correlation between eGFR (as calculated by serum cystatin C) and lipid parameters was found with the exclusion of HDL. The atherogenic indices also showed significant negative correlation with eGFR estimation by serum cystatin C. However, the same significant correlation was not exhibited by eGFR estimation by serum creatinine.
It is well established that the presence of CKD in CVD patients and vice versa, aggravate each other with progressing age [23]. In this study, the lipid profile served as a marker of CV risk. While the mean of TC, LDL and VLDL were normal, (TC: 179.5 ± 57.75 mg/dl; LDL: 116.32 ± 49.17 mg/dl; VLDL: 24.72 ± 13.33 mg/dl), their levels exceeded the highest quartiles of the reference ranges [7]. With regards to TG and lipoprotein ratios or atherogenic indices, the mean was raised (TG: 123 ± 61 mg/dl, TC/HDL: 4.77 ± 1.65, LDL/HDL: 3.11 ± 1.40), when compared to reference ranges [7,8]. HDL was below the lower limit of the reference given by NCEP-ATP (HDL: 38.47 ± 7.04 mg/dl) [24]. Pennell, et al. found increased prevalence of dyslipidemia in CKD patients, (characterized by elevated TG, VLDL and reduced HDL, along with a relatively lesser rise in LDL and TC levels) particularly in end stage disease [25]. A study by Lowrie indicated that serum cholesterol levels might be lower in renal disease due to malnutrition, while also implying that lower cholesterol values can be indicative of CV risk [26]. Wanner, et al. observed that while the relation between lipids and CVD is well established in the general population, the same cannot be said for patients with CKD. The reason for this was suggested to be the diverging results of retrospective observational trials, and the many confounding factors involved [27].
In this study, the lipid values tended to be on the higher side with HDL being below the reference range. Our study supports the finding that lipids are elevated in CKD which are known markers of CV risk.
Our study found lipid profile (TC, TG, LDL, VLDL) excepting HDL to be significantly and negatively correlated with eGFR by serum cystatin-C (p < 0.05), using the CKD-EPI formula. Even the ratios; TC/HDL, LDL/HDL were found to correlate inversely and significantly (p < 0.01). Similar significant negative correlation was not seen between eGFR by creatinine (MDRD formula) and lipid indices.
Cystatin-C has been found to be a better predictor of mortality and adverse CV events than serum creatinine [28-31]. The ‘Heart and Soul Study' reasoned that this could be due to the role of inflammation [32]. Multiple studies have found that serum cystatin-C remains unaffected by muscle mass, gets completely reabsorbed, and is secreted at a constant rate in almost all cells of the body [5,33-35]. These features make it a near ideal renal marker. Shlipak, et al. confirmed that cystatin-C has a linear association with GFR, even in patients of pre-clinical kidney disease (GFR: 60-90 ml/min/1.732) [36]. However, not all studies have given us the same understanding, Menon, et al. stated that eGFR is not sensitive enough to reflect the connection between mild renal impairment and CV risk [37]. Recent studies and many of the researchers however support the use of serum cystatin-C as a GFR marker, because it can serve as a more stable renal marker, a predictor of CV risk and also many other conditions like metabolic syndrome, insulin resistance among others. This study, in support of serum cystatin C, finds that eGFR calculated by serum cystatin-C relates inversely and significantly well with lipid profile with the exception of HDL cholesterol.
The importance of this study would be its role as a pilot study in studying an upcoming renal biomarker namely Cystatin C in relation to CKD and its consequent morbidity. It has been suggested that no single biomarker may be perfectly predictive but looking at combinations like in our study will better help in the risk stratification [6] and to study how they impact on morbidity and mortality as we have tried to compare the two biomarkers in our paper. The analysis was robust.
However, the limitations of this study include a relatively small sample size and the absence of comparison of both the equations with measured GFR. As follow-up was not done, cardiovascular events could not be evaluated in individual patients. The cardiovascular risk was evaluated based only on the lipid profile. The unavailability of IDMS (isotope dilution mass spectrophotometry) as a uniform method to estimate serum creatinine in an Indian setting is also a limitation in this study. The exact role of eGFR by creatinine and cystatin-C in predicting the risk of morbidity and mortality in cardiac patients with CKD was not established. Also, patients in the early stages were very few. The other limitations to be kept in mind are the higher cost of Cystatin c based tests and lack of ready availability of this biomarker. Other factors like BMI were not included, as this study was just an initial pilot study to study only the link between the lipid profile and the two equations to extimate eGFR by the serum creatinine and cystatin-c method. Moreover the BMI (body mass index) studied in other studies showed a non-linear relationship with both creatinine based and cystatin based equations thus showing an elevated eGFR for persons with a BMI exceeding 30 kg/m2. Owing to this a bias could occur between the estimated cardiovascular risk from decreased GFR in obese persons in longitudinal studies [38]. Hence BMI was not looked at in this study. Traditional risk factors like smoking could not be studied in detail as there were only two smokers in the group.
The Cardiovascular risk was also calculated by using the Heart Risk Calculator [39,40] and data for both males and females is shown in the Figure 2A, Figure 2B, Figure 3A and Figure 3B. It shows the 10 year risk and also the life time risk for both males and females using mean values in the calculator. It showed that the 10-year ASCVD risk in males was 3.6% and the life time risk in males was 5%. The 10-year ASCVD risk in females was 1.2% and the corresponding lifetime risk in females was 8%. Women are probably more protected in the 10 year phase, estrogens may be exerting a strong anti-oxidant effect/action in the micro-environment, providing more potent protection to the female gender [41,42]. And as the higher cystatin values were associated with males and with older age hence the values of cystatin based GFR estimation may hold more relevance in the elderly males.
 Figure 2a: Lifetime risk of cardiovascular diseases for males [39].
View Figure 2a
Figure 2a: Lifetime risk of cardiovascular diseases for males [39].
View Figure 2a
 Figure 2b: Lifetime risk of cardiovascular diseases for males [39].
View Figure 2b
Figure 2b: Lifetime risk of cardiovascular diseases for males [39].
View Figure 2b
 Figure 3a: Lifetime risk of cardiovascular diseases for females [39].
View Figure 3a
Figure 3a: Lifetime risk of cardiovascular diseases for females [39].
View Figure 3a
 Figure 3b: Lifetime risk of cardiovascular diseases for females [39].
View Figure 3b
Figure 3b: Lifetime risk of cardiovascular diseases for females [39].
View Figure 3b
In order to establish the importance and relevance of this biomarker Cystatin C, more research needs to be done after including earlier stages of renal disease and also including the follow up of these patients. The results of this study can be generalized to the Rural Pondicherry area in South India as this study was done in a part of rural industrialized setting of Pondicherry and is a representative sample of that population.
The study population of this cross-sectional study were mostly distributed in 4th and 5th stages of CKD by both MDRD equation and CKD-EPI equation. The cystatin C based eGFR showed significant correlation with serum lipids and CVD lipid indices which were not seen with creatinine based e-GFR. The implications of our research suggest that in future, serum cystatin C may steadily overtake serum creatinine as the most commonly used and a more effective and stable renal biomarker.
We thank the management of Sri Manakula Vinayagar Medical College and Hospital for permitting us to conduct this study and for funding us through the institutional research fund. We thank the Department of community medicine for giving us technical support and for helping us with the necessary statistical support.
Dr. P Ravikumar helped with the concept, planning of study, literature review, editing, writing and review of the manuscript. Dr. Mitali helped with the planning of the study, data collection, literature review, writing, review of the manuscript and proof reading. Dr. Asmathullah helped with the planning of the study, review of the manuscript, editing of the manuscript and proof reading.
The authors have no financial conflicts of interest to declare!
No animals were used for the study. All the due rights for humans were preserved in this study.
Not applicable.
The Strobe Tool guidelines and methodology were followed. P.S. The Strobe Tool for cross sectional studies was applied in the critical appraisal of this paper!
All available data can be obtained by contacting the corresponding author. All of the individual participant data collected during the study is available, after de-identification, beginning 3-months and ending 5-years following article publication.
Funding was from our institutional (Sri Manakula Vinayagar medical college and Hospital, Pondicherry) intramural grant.
The authors declare no conflict of interest, financial or otherwise. The results presented in this paper have not been published in whole or in part, except in abstract format.