TAR syndrome is a genetic disorder characterized by a lack of radial bone in the forearm and a lack of blood platelets. Thrombocytopenia prevents normal blood clotting and causes bleeding easily and often bleeds from the nose. The TAR syndrome is caused by the mutation of the RBM8A gene, which is based on the long arm of chromosome 1, which is based on 1q21.1.
TAR syndrome, RBM8A gene, Blood disorder, Genetic mutations
TAR syndrome is a genetic disorder characterized by a lack of radial bone in the forearm and a lack of blood platelets. Thrombocytopenia or deficiency of blood platelets are commonly present at birth, and over time, these blood cells also decrease. In some cases, platelet levels are normal in people with TAR syndrome Figure 1 [1].
 Figure 1: Images of infants with TAR syndrome associated with skeletal dysfunction in the radial bone of the forearm. View Figure 1
Figure 1: Images of infants with TAR syndrome associated with skeletal dysfunction in the radial bone of the forearm. View Figure 1
Thrombocytopenia prevents normal blood clotting and causes bleeding easily and often bleeds from the nose. Severe hemorrhage may occur in the brain and other organs, especially in the first year of life, in people with TAR syndrome. This bleeding may damage the brain and lead to mental disability in patients with TAR syndrome Figure 2 [1,2].
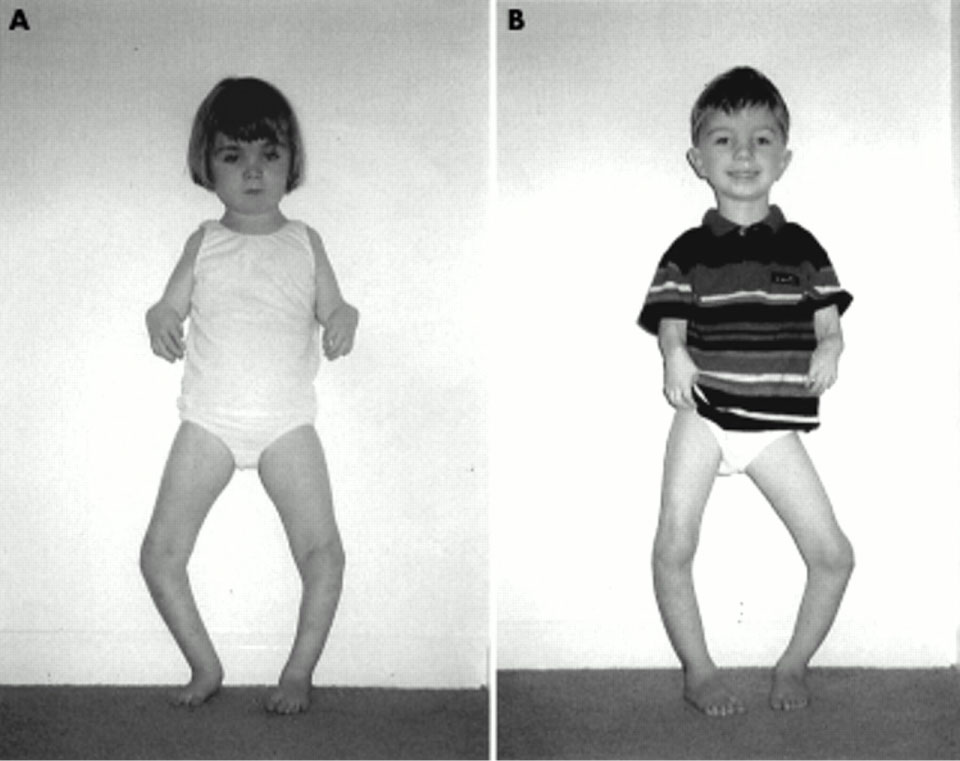 Figure 2: Other images of children with TAR syndrome associated with skeletal disorders. View Figure 2
Figure 2: Other images of children with TAR syndrome associated with skeletal disorders. View Figure 2
The severity of skeletal disorders associated with TAR syndrome varies among those with this syndrome. The radial bone of the forearm may affect both the hands of the affected TAR syndrome and lead to poor development of these bones. In addition, other skeletal disorders, such as swaying of fingers and toes (cinnabar or fingers), or penile curvature, skeletal disorders on the hands, arms and legs may also occur in the TAR syndrome [1,2].
Other features that can occur in the TAR syndrome include heart abnormalities, kidneys, abnormal maxillary jaw (micrognatia), prominent forearm, and low-level and unusual ears. It should be noted that about half of people with TAR syndrome have an allergic reaction to cow's milk that may worsen thrombocytopenia in the syndrome Figure 3 [1,2].
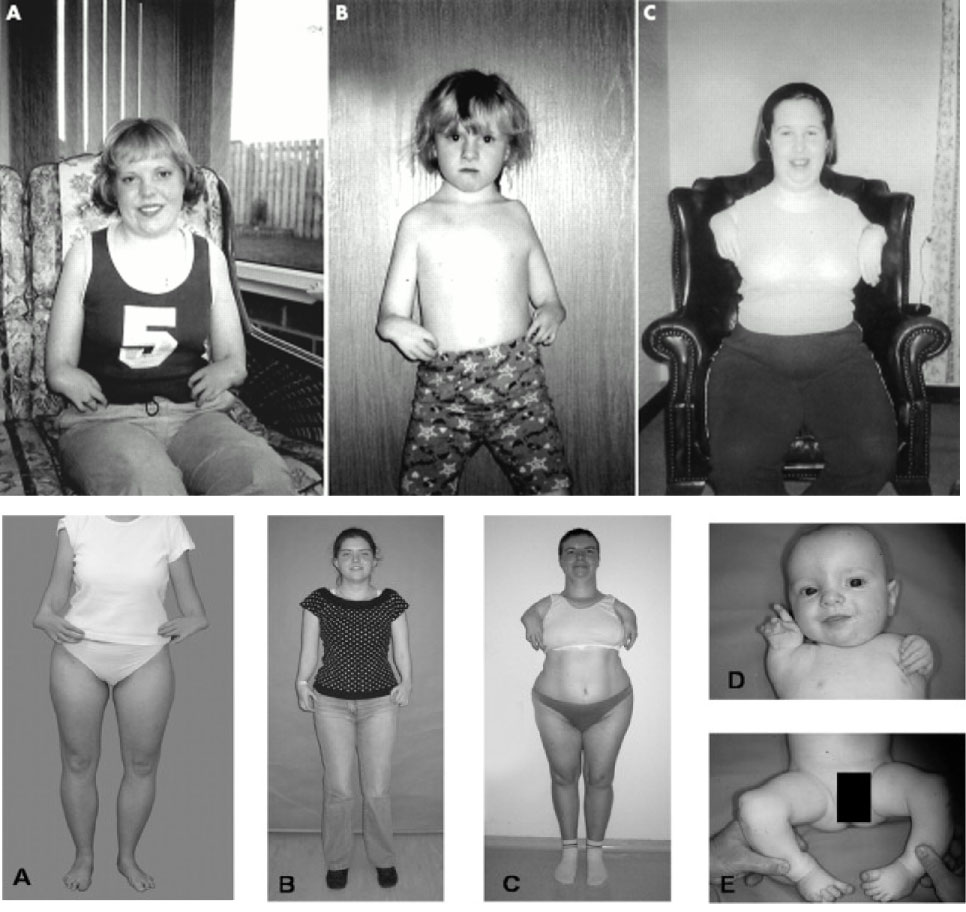 Figure 3: Another view of patients with TAR syndrome associated with skeletal disorders in the radial bone of the forearm. View Figure 3
Figure 3: Another view of patients with TAR syndrome associated with skeletal disorders in the radial bone of the forearm. View Figure 3
The TAR syndrome is caused by the mutation of the RBM8A gene, which is based on the long arm of chromosome 1, which is based on 1q21.1. The gene provides instructions for protein synthesis called Protein 8A, an RNA binding motif that is involved in several important cellular functions and the production of other proteins. The mutation in the RBM8A gene, which is a type of mutation, eliminates at least 200 kilobytes of DNA building blocks from the long arm of chromosome 1 in the q21.1 region, which also led to a decrease or no production of 8A protein, the binding motif of the RNA To be It seems that the decrease in protein 8A causes problems in the growth of specific tissues, but it is not yet known whether the decrease or non-production of this protein, as it develops, causes specific signs and symptoms of TAR syndrome Figure 4 [1-3].
 Figure 4: Schematic view of chromosome no. 1 in which the RBM8A gene is located in the long arm of this chromosome as 1q21.1. View Figure 4
Figure 4: Schematic view of chromosome no. 1 in which the RBM8A gene is located in the long arm of this chromosome as 1q21.1. View Figure 4
TAR syndrome follows an autosomal recessive pattern in 75% of cases. Therefore, in order to produce this syndrome, two versions of the mutated gene RBM8A (one parent and one mother) are needed, and the chance of having a child with TAR syndrome in an autosomal recessive state is 25% for each pregnancy. About 25% of cases of TAR syndrome are due to new mutations and no family history [1-3].
TAR syndrome is a rare genetic disorder, with an incidence of around 1 in 100,000 live births worldwide [1-4].
TAR syndrome is diagnosed based on the clinical and physical findings of the patients and some pathological tests. The most accurate method for detecting this syndrome is the molecular genetic test for the RBM8A gene in order to investigate the presence of possible mutations or molecular cytogenetic techniques such as in situ fluorescence hybridization technique (FISH) to investigate the presence of a small mutation in the long arm of chromosome 1 as 1q21. 1 is Prenatal diagnosis is also possible by using the PGD technique and amniocentesis fluid or by sampling the embryo's chorionic pelvis Figure 5 [1-5].
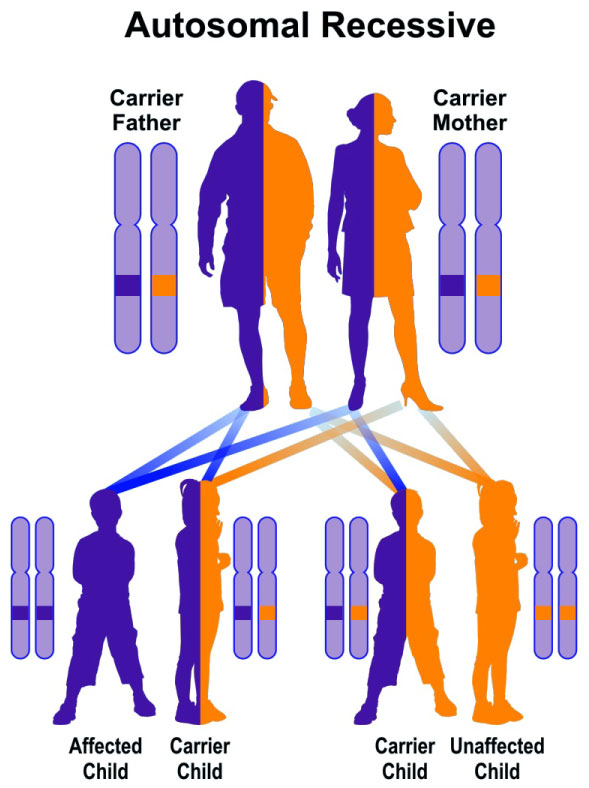 Figure 5: schematic view of an autosomal recessive hereditary pattern that follows the TAR syndrome. View Figure 5
Figure 5: schematic view of an autosomal recessive hereditary pattern that follows the TAR syndrome. View Figure 5
The TAR syndrome treatment and management strategy is symptomatic and supportive. Treatment may be done by a team of experts, including pediatricians, hematologists, orthopedic surgeons, and other healthcare professionals. There is no definite treatment for this syndrome and all clinical measures are needed to reduce the suffering of the sufferers. Genetic counseling is also important for all parents who want a healthy baby Figure 6 and Figure 7 [1,6-8].
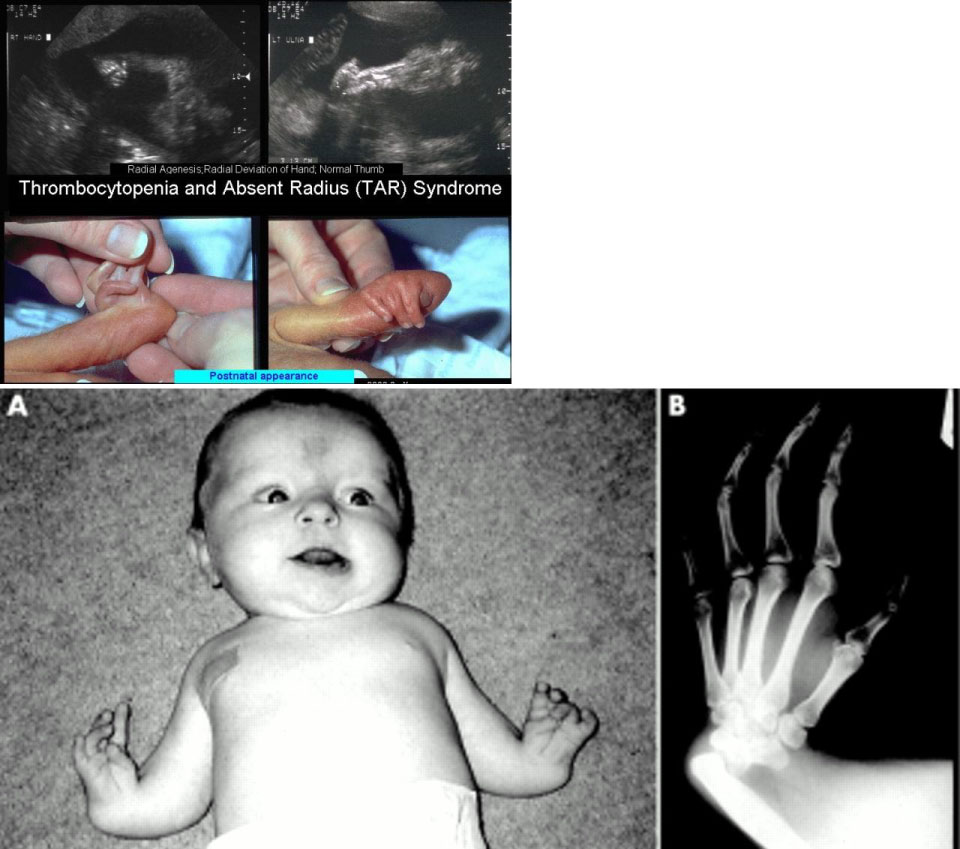 Figure 6: An overview of TAR syndrome disorders. View Figure 6
Figure 6: An overview of TAR syndrome disorders. View Figure 6
 Figure 7: Radiology image of a fetus with TAR syndrome associated with radial bone defect in the forearm. View Figure 7
Figure 7: Radiology image of a fetus with TAR syndrome associated with radial bone defect in the forearm. View Figure 7
TAR syndrome is a genetic disorder characterized by a lack of radial bone in the forearm and a lack of blood platelets. Thrombocytopenia prevents normal blood clotting and causes bleeding easily and often bleeds from the nose. The TAR syndrome is caused by the mutation of the RBM8A gene, which is based on the long arm of chromosome 1, which is based on 1q21.1. There is no definite treatment for this syndrome and all clinical measures are needed to reduce the suffering of the sufferers. In the near future, gene therapy techniques will be used to improve the health of these patients 1-8. This is a scientific advocacy article that aims to provide the reader with the scientific content of TAR syndrome in a very specialized way.