• The main purpose of this study is to assess the prevalence of elder abuse in Portugal, more specifically in a central hospital in Coimbra and its impact on victims' health. The analysis of the results concludes that 36% of the participants report experiencing at least one indicator of abuse. There is a relation between the number of abuse indicators and the female gender, low educational level, depressive symptoms, increased functional dependence and health status.
• It is crucial to alert the medical community, other health professionals and the society to the impact of elder abuse, in order to revert it.
Mistreatment in the elderly people represents an increasing problem in today's society, making it crucial to understand its true impact. This study aims to evaluate the signs of mistreatment in a population of elderly people admitted to the Internal Medicine A services of Centro Hospitalar e Universitário de Coimbra (CHUC) and relate them with risk factors.
The data was obtained through a questionnaire, with the participation of 100 elderly people hospitalized in CHUC. The questionnaire was divided into 5 sections, allowing the collection of sociodemographic and health data, information on emotional status (Geriatric Depression Scale) and functional status (Katz Index) and the prevalence of abuse indicators with the Question to Elicit Elder Abuse (QEEA) instrument.
The analysis of the results concludes that 36% of the participants report at least one indicator of abuse. Emotional abuse (29%) and neglect (24%) are more frequently detected, followed by financial abuse (12%) and physical abuse (5%). When relating the indicators of mistreatment with the other variables, it is concluded that there is an association between the number of mistreatment indicators and female gender, low educational level, depressive symptoms and increased functional dependence.
This study is alerting us to the high number of elderly people with signals of mistreatment in CHUC, a central Hospital in Coimbra, Portugal. It is important that the medical community and other health professionals become aware of the issue in order to develop policies capable of minimizing this situation.
Aged, Elder abuse
Nowadays, we are struggling with a demographic explosion due to increasing lifespan, which results in a growth of the elderly population. For this reason, there were a higher number of elderly people vulnerable to mistreatment [1]. Elder abuse represents an increasing problem in our society [1,2], making it crucial to understand its true impact in order to create appropriate intervention strategies. In Portugal, the percentage of individuals over the age of 65-years-old increased from 18.7% to 20.7% between 2010 and 2015 and it is estimated that it will continue to grow within the next few years [3].
According to the World Health Organization (WHO), elder abuse can be defined as a single, or repeated act, or lack of appropriate action, occurring within any relationship where there is an expectation of trust which causes harm or distress to an older person [4]. Elder abuse can take various forms such as financial, physical, psychological and sexual. It can also be the result of intentional or unintentional neglect. The most prevalent type of abuse is psychological abuse, followed by neglect and financial abuse [4-6]. Reading a recent study, financed by WHO, we can conclude that 15.7% of the elderly are victims of abuse, even though the wide variation according to different parts of the globe [1]. A study realized by Dong, et al., concluded that less than 4% of elder abuse situations are signalized to competent authorities which means that there is still high number of victims non identified [7].
In Portugal, according to the Portuguese Association for Victim Support (APAV), crimes against people aged 65 years and above have been more reported, rising every year. In 2000 there were reported 290 cases, evolving to 1261 cases in 2012, which means an increase of 179% in 12 years. The majority were committed by spouses, children, other relatives and neighbours and 73% of victims were women [8,9]. One of the bigger studies at a national level in Portugal, performed by Ricardo Jorge Institute, between 2011 and 2014, revealed that 12.3% of the Portuguese elderly are victims of at least one kind of abuse. The physical and financial abuse was the more reported, strongly related with oldest age, increasing in functional dependence and poor levels of schooling [10]. According to Marques, et al., the prevalence of elder abuse in a rural area in Portugal is about 70% [11].
In scientific literature, a high number of risk factors are described, and they can be related with the victim itself, with the abusers or with the community environment [12]. A higher number of diseases and comorbidities are associated with higher levels of depression, functional dependence and burden of work to caregivers, constituting a situation that can promote the occurrence of mistreatments [13,14]. According to Dong, et al., dementia is a risk factor with considerable impact, mainly to suffer of psychological abuse, with a estimated prevalence between 27.9% and 63.2% [15]. The household also represents a risk factor, since 46% of abusers are family members and 37% healthcare workers from Elder institutions [13]. The elderly population is also at higher risk when they share house with the caregiver, especially if there is a financial dependence, history of alcohol and drugs abuse or mental illness [13,16,17].
Recent investigation demonstrated that being a victim of elder abuse have major health consequences, since they have a higher risk of mortality, morbidity, anxiety, depression and necessity to visit emergency services [18-20]. The relation between elder abuse and higher levels of anxiety, depression symptoms and suicide attempt are also identified [21,22]. The quality of life and health issues associated to elder abuse cannot be neglected, so it is important that physicians and other health professionals are aware of this problem. Some studies have reported that a high proportion of elderly victims of physical abuse are conducted to emergency services few hours after the incident and concluded that the abuse passes frequently unnoticed [23].
There is high number of studies about elderly abuse, with great variation of results according to the socio-demographic characteristics. In Portugal there is still a lack of information regarding this theme. The purpose of this study is to analyze the signs and quantify the number of elderly victims of mistreatment institutionalized in a Portuguese central Hospital. Consequently, with the divulgation of the results, another purpose is to alert healthcare professionals to the issue. It is also intended to relate the elder abuse indicators with risk factors and possible consequences to obtain information that can contribute to define intervention strategies.
The data was collected through a questionnaire, with the participation of 100 elderly people admitted to the Internal Medicine A service of CHUC, a central and university teaching hospital in Portugal, between 15 October and 15 December 2017. There were 256 individuals admitted, during this period in the hospital service. In this study there were included only people over 65 years and excluded those with a bad cognitive performance and without capacity of giving answers due to their medical conditions, so 156 were excluded. The final sample was composed of 42 participants of the male gender and 58 of the female gender. The selection of participants was made in agreement with clinical records.
The participation in the study was anonymous since there were not identification elements in the questionnaire. The questionnaire was divided into 5 sections: Sociodemographic data; information on emotional status through the Geriatric Depression Scale; evaluation of the functional state using the Katz index; prevalence of evidence of abuse with the Question to Elicit Elder Abuse (QEEA) instrument (Cronbach's alpha 0.96) and data on health status. The Katz index and the Yesavage scale are instruments used globally and recommended by the Portuguese Society of Internal Medicine [24,25]. The QEEA was adapted to Portuguese language by Ferreira-Alves and Sousa [26]. The questionnaire was distributed to the participants so they could answer alone without other persons nearby. In cases of illiterate people, the questions were made through an interview made by the researchers.
The QEEA instrument (Appendix 1) is composed by 15 questions with a Yes or No answer. Each question represents an elder abuse indicator, and they are divided into 4 groups, one for each kind of abuse. There are 4 questions related to physical abuse, 5 questions related to emotional abuse, 4 questions related to neglect and 2 questions related to financial abuse. This instrument has a high sensitivity and specificity and can be used as a screening method. Further investigation is needed in cases of positive indicators in order to confirm the elder abuse occurrence.
A Statistical analysis was made with the collected data, employing IBM SPSS Statistics 22.0. First, a descriptive analysis was made in order to characterize the sample. Then a bivariate inferential statistics analysis was made in order to relate abuse indicators with risk factors described in the literature. Nonparametric tests were used since the normality of data was not verified. In order to make possible the generalization of this study results a significance level of 0.05 (p < 0.05) was defined.
In this study we had 42 participants of the male gender and 58 of the female gender, with ages between 65 and 96-years-old (mean: 80.18). Regarding the marital status, 47% were married, 46% widow, 5% single and 2% were divorced. Of the interviewed, 31% lived at urban zones against 69% at rural zones. With regards of the household, 69% have their own home, 16% lived in a relative's house and 15% in nursing home. Only 18% of them lived alone. In order to evaluate social interaction, one question was made about visiting friends and relatives and 56% answered positively. Of the interviewed population, 2% had no one to contact in case of emergency.
Poor levels of education were common: 31% had never attended, with only 2% reaching university level. Financial independence was reported by 75%, while help for medication management was required by 30%.
In Figure 1 we can see the results of the application of Katz Index to evaluate the functional status of the participants. It is important to note that 64% are totally independent and only 3% were totally dependent. The remaining ones presented different levels of partial dependence.
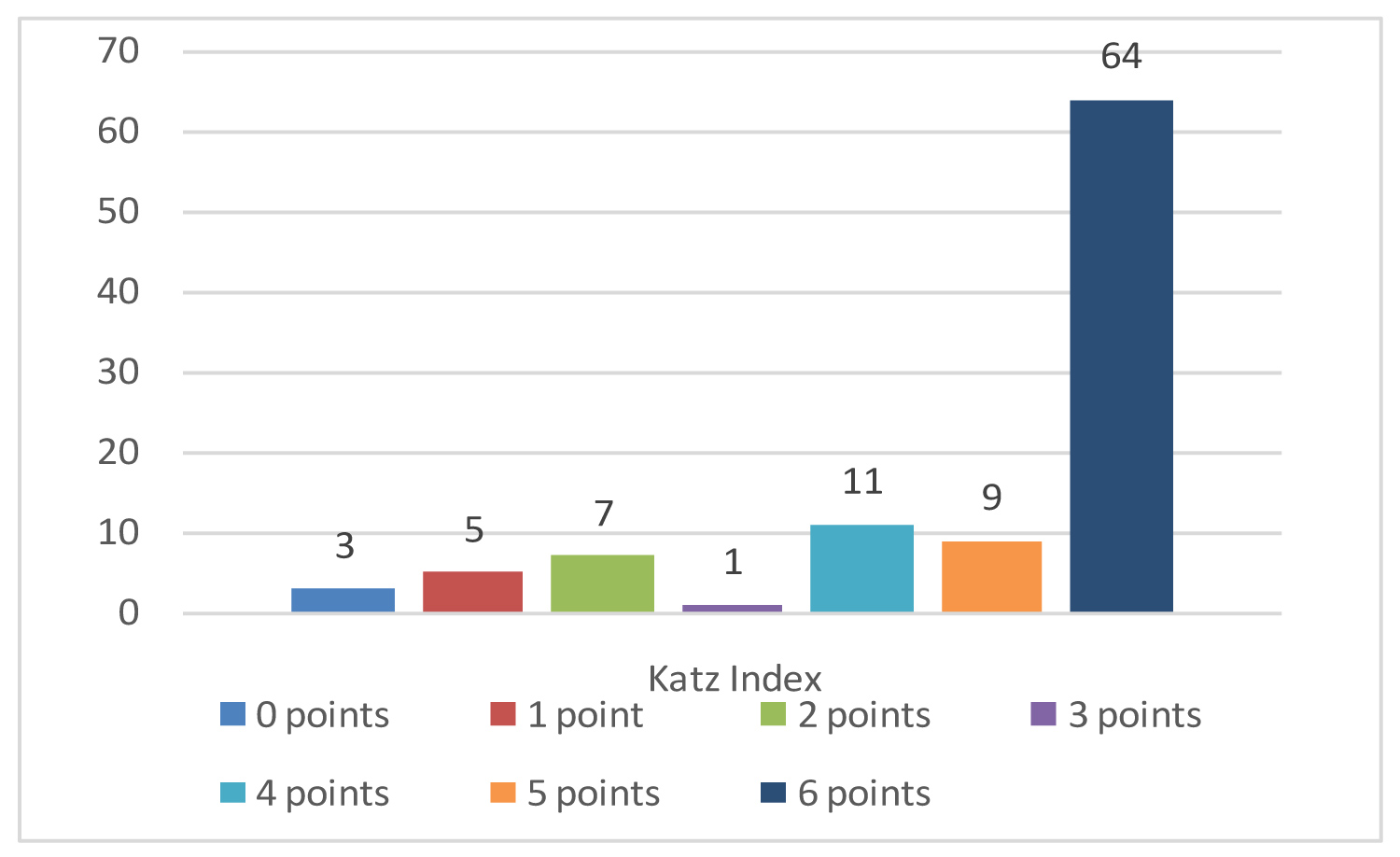 Figure 1: Distribution of the population according to their functional status, using Katz Index.
View Figure 1
Figure 1: Distribution of the population according to their functional status, using Katz Index.
View Figure 1
In terms of depressive symptoms, the instrument chosen was the Geriatric Depression Scale and the results can be analysed in Figure 2. According to the results, 31% of the participants seem to have a depression, of which 5% presented answers compatible with severe depression.
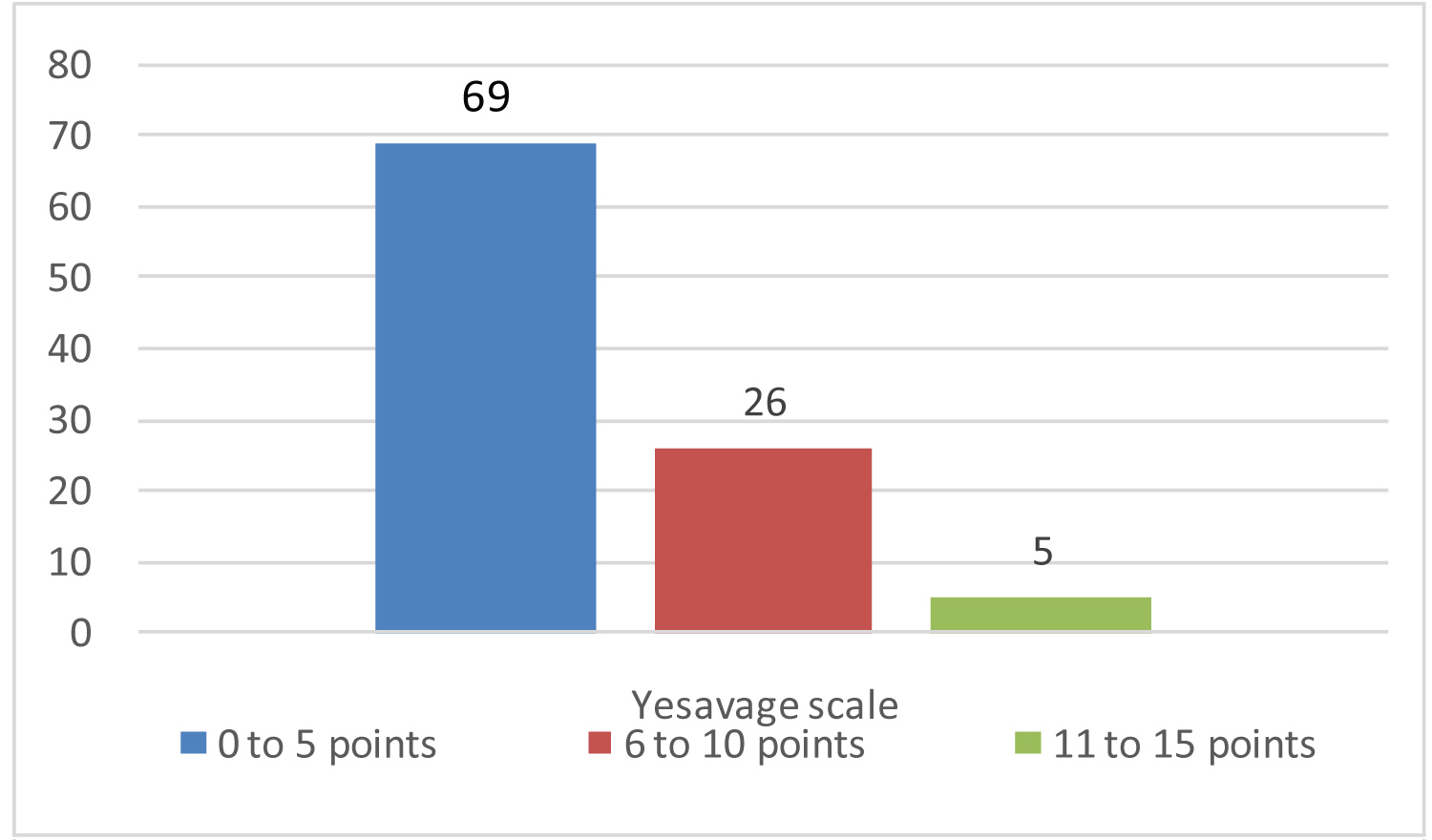 Figure 2: Distribution of the population according to their symptoms of depression, using Yesavage Scale.
View Figure 2
Figure 2: Distribution of the population according to their symptoms of depression, using Yesavage Scale.
View Figure 2
The results of the QEEA (Appendix 1) with the number of indicators of Elder abuse categorised by type of abuse can be found in Table 1 and Table 2.
Table 1: Distribution of the population according to the type of abuse indicators. View Table 1
Table 2: Distribution of the population according to the total number of abuse indicators. View Table 2
It is worth mentioning the high number of elder with at least 1 abuse indicator 36%, and the maximum of abuse indicators in the same individual is 8. The prevalence of elderly abuse in the studied population is higher than expected, since its incidence is estimated to be 15.7% globally, according to the WHO [4,9]. Comparing with other studies realized in Portugal, our results are higher than the one realized by Ricardo Jorge Institute where a prevalence of 12.6% was found [10]. The most prevalent types of abuse were the emotional abuse with 29% and neglect with 24% followed by financial abuse and finally physical abuse. These results are in accordance with the scientific literature, since the most prevalent type of abuse reported are the emotional abuse and neglect [1,7-11].
In Table 3, we can see the results of Mann-Whitney-U test used to relate abuse indicators with the gender. Analysing the results, we can conclude that individuals of the female gender are more susceptible to be victims of elder abuse, more specifically emotional abuse. In our population it seems that female gender individuals were more susceptible to neglect, physical and financial abuse, although we cannot make any generalization due to the significance level (p > 0.05). We can conclude that the female gender is a risk factor to be a victim of elderly abuse, as expected by the results of Lachs, et al. [5].
Table 3: Results of the Mann-Whitney U test used to relate gender with abuse indicators. View Table 3
The results of Kruskal-Wallis test used to relate level of schooling with elder abuse indicators can be seen in Table 4. We only found statistically significant differences when it comes to emotional abuse (p < 0.05). According to these results, it can be concluded that elderly people with poor levels of education are at greatest risk of suffering emotional abuse. This association is in agreement with a recent study made in Portugal [10].
Table 4: Results of Kruskal-wallis test used to relate schooling level with elder abuse indicators. View Table 4
In order to relate elder abuse indicators with the results of Katz Index and Yesavage Scale, the test chosen was the Spearman Correlation. The results are presented in Table 5. Analysing the results of the correlation with Katz Index, we can note that individuals with higher dependence presents higher emotional abuse and total abuse indicators. This relation is expectable, since Dong, Simon and Evans demonstrated that the functional dependence is one of the most important risk factors to be a victim of abuse by caregivers [20].
Table 5: Results of Spearmen correlation used to relate abuse indicators with functional status and depressive symptoms. View Table 5
As for the correlation with Yesavage scale results, an association can be found with all the type of indicators and total abuse indicators. Then, we can deduce that depressive symptoms are strongly related with all types of elder abuse, since they are simultaneously a factor risk and a consequence, as it was verified in previous studies [13,16]. It is important to remember that higher levels of suicide ideation was found in victims of elderly abuse in previous studies [21,22].
There were not found any statistically significant differences between abuse indicators and the remaining variables as zone of residency, type of household and marital status.
The main purpose of this investigation was to quantify the potential victims of elder abuse in a population of hospitalized elders. We can conclude that 36% of the participants have submitted at least one indicator of abuse with a maximum of 8 indicators on the same person. Emotional abuse (29%) and negligence (24%) were more frequently detected, followed by financial abuse (12%) and physical abuse (5%). The numbers obtained are higher than expected, according with previous studies, but it is important to remember that some of these individuals may not be victims of abuse, since the QEEA is only a screening tool. Investigations with a multidisciplinary team may be realised in order to confirm the abuse and take necessary measures to protect the victim. However, a large number of potential victims were found, some of them with two or more indicators, which reinforces the probability of abuse occurrence.
When relating the indicators of mistreatment with the other variables, it was determined that there is a strong association between the total of mistreatment indicators and individuals of the female gender, low educational level, depressive symptoms and increased functional dependence. No evidence was found of connection between abuse indicators and the remaining variables probably due to the methodology of the study and to the size of the sample.
This study has some limitations, as previously said, the QEEA instrument is a good screening method but it involves a confirmation of the abuse situation. The confirmation could not be made, once the anonymity of the participants had to be assured due to ethical issues. Another limitation is related to the population, with a small size and a higher number of women due to the inclusion criteria, once there were more women hospitalized during the realization of the study. The study was realized only at one hospital, so the results obtained are limited to a geographical area of Portugal, and has some particularities related to the health status since it was a hospitalized population. Finally, the fact that elderly with cognitive impairment were excluded in order to can be a limitation since it can be a risk factor for being a victim.
With the divulgation of the data obtained we hope to sensitize physicians and other healthcare professionals to the issue, not only family doctors but also the ones that work in emergency services and hospitals. We recommend the application of QEEA as a screening method, especially in elders with risk factors since its utilization is easy and quick.
We are assisting to the ageing of population and structural changes in communities, with an increase of elder abuse over the globe. As recommended by the United Nations, policies must be developed in order to minimize its consequences and to reverse the situation.
On behalf of all authors, the corresponding author states that there is no conflict of interest.