Background: Immobility during hospitalization may lead to poor patient outcomes including extended length of stay (LOS). The practice site experienced extended LOS in elderly patients and lacked a nurse-led multidisciplinary mobility program to optimize the mobility of patients aged 65 and older. The purpose of this quality-improvement project was to determine if the Mobilization of Vulnerable Elders (MOVE) protocol improved length of stay (LOS) and mobility among older adult patients.
Methods: Quantitative, quasi-experimental quality improvement project was conducted on sample of 234 elderly patients. Faye Abdellah's twenty-one nursing problems theory and Ian Graham's Knowledge-to-Action cycle provided the scientific underpinnings for this project. Instruments utilized in this project were the MOVE protocol and the Early Mobilization Assessment Algorithm.
Results: A Mann-Whitney U was utilized to compare LOS among 234 patients; n = 126 in the pre-implementation group and n = 108 in the post-implementation group, U = 7,615, z = 1.6, p = 0.112, with a small effect size r = 0.11. However, implementation of the MOVE protocol indicated clinical significance evidence by 301 days (n = 94) in which a patient achieved three mobilizations in a 24-hour period.
Conclusions: Results did not demonstrate statistical significance; however, the MOVE protocol promoted patient mobility. Therefore, the findings suggest that continued utilization of the MOVE protocol may enforce the need for mobility to improve LOS. Replication of the project is needed in larger settings and over a longer period of time.
Elderly patients are at substantial risk of functional decline, adverse health outcomes, and prolonged hospital stays due to unnecessary immobilization during hospitalization [1]. Patients, age 65 and older, spend most of their hospital stay in bed instead of walking or being out of bed (OOB) [2]. As a result, muscle loss, venous thromboembolism, pressure injuries, orthostatic hypotension, loss of concentration and motivation, depression, and delirium occur because of immobility [3-7]. It is reported that elderly patients are primarily immobile during a hospital stay, spending 66 to 117 minutes walking or standing [2]. This finding results in an extended length of stay (LOS) [8]. Hospitals recognize immobility as a detriment and are integrating evidence-based practices (EBP).
The standard practice of the project site relied heavily on nursing practice to mobilize all patients. However, rising patient acuity, resource shortages, and more recently, the Coronavirus (COVID-19) pandemic during the time of prolonged LOS significantly impacted the ability of nurses to mobilize patients consistently. As a result, elderly patients remain in bed for extended periods, which caused prolonged LOS, pressure injuries, falls, and hospital-acquired pneumonia at this project site. Therefore, there was a calling for a multidisciplinary early mobility initiative to improve patient mobilization and decrease LOS.
In 2018, the MOVE protocol was implemented in Ontario, Canada, at 14 different hospitals and utilized a quantitative quasi-experimental design to evaluate the primary outcomes of LOS and mobility frequency [9]. The population size was 12,490 patients, mean age of 80.0, with the entire population being cared for on inpatient medical units [9]. After comparing pre- and post-implementation groups, findings indicated a significant increase in the number of patients out of bed by 10.56%, 95% CI [4.94, 16.18]; (p < 0.001) and reduction in the median LOS by 3.45 days, 95% CI [-11, -1.2]; (p = 0.015) [9].
The MOVE protocol had been utilized in different studies and had demonstrated validity and reliability [9-11]. Therefore, the purpose of this quantitative, quasi-experimental, quality-improvement project was to determine if Mobilization of Vulnerable Elders (MOVE) protocol improved LOS among older adult patients. The following hypotheses were proposed:
(1) Length of stay would decrease in elderly patients that received treatment with the MOVE protocol;
(2) Mobility levels would improve in elderly patients that received treatment with the MOVE protocol.
This quality improvement project implemented a quasi-experimental design aimed to determine the impact of the MOVE protocol on elderly patient LOS and mobility. This strategy was an appropriate method for answering clinical questions because this approach established two groups and determined if there was a substantial effect on a participant group after an intervention or change had been instituted.
The location of this quality improvement project was a rural Pennsylvania acute care center that had a 22-bed medical-surgical unit. Inclusion criteria were: Patients age 65 and older, admitted to medical-surgical unit under the medical, surgical, or trauma services. The exclusion criteria were: adults less than age 65 and incarcerated individuals.
An adequate sample size was needed to determine an appropriate number for the pre- and post-implementation groups. Using a total population size of 50 patients, a confidence level of 95%, and a margin of error set at 5%, the ideal sample for the pre- and post-implementation groups were 45 patients each to satisfy a significance level of α = 0.05.
The quality improvement project was guided through the scientific underpinnings of Abdellah's Patient-Centered Approach theory and Knowledge-to-Action framework. Abellah's nursing theory illustrates that patients possess a physical need for optimal activity and exercise while hospitalized [12]. This nursing theory focuses on human needs and guiding the care of those who are in positions of medical authority [12]. The Knowledge-to-Action (KTA) cycle served as the change theory to provide nurses and change agents a detailed process of creating knowledge and translating knowledge into evidence-based interventions [13]. The process of knowledge creation started by searching contemporary and relevant literature while refining knowledge until the MOVE protocol was identified. While knowledge creation occurs, the action cycle identified immobility and prolonged LOS as a problem in clinical practice and tailored the MOVE protocol to fill the practice gap [13].
Following IRB approval, the quality improvement project was introduced to the medical-surgical unit's nursing and physical therapy team members. Nurses and physical therapists were provided education regarding the MOVE protocol which included mobilization assessments with the Early Mobilization Assessment Algorithm (Appendix A) one week before implementation. Education included the conduction of a virtual journal club. The educational opportunity enabled the presentation of MOVE protocol studies in a one-hour discussion.
Adjunct to the journal articles, a PowerPoint presentation was developed to guide the education session. The information detailed with the PowerPoint presentation included MOVE protocol materials, including the Early Mobilization Assessment Algorithm.
Additional educational opportunities were presented to reinforce the MOVE protocol and educate nursing staff who were not present for the virtual journal club. Each morning brief provided the nursing staff with education on utilizing the Early Mobility Assessment Algorithm to mobilize elderly patients. Education sessions were held for one-week prior to implementing the MOVE protocol. One-to-one education occurred if a staff member was not present for any education session. A unit roster of nurses was kept, monitoring session attendance. Physical therapy team members received similar education during daily departmental briefs. Education consisted of the MOVE protocol and correct mobility documentation.
Once all staff had been educated on early mobilization and the MOVE protocol, all elderly patients admitted to the medical-surgical unit received early mobilization therapy guided by the MOVE protocol. The admitting nurse or physical therapist completed the initial mobility evaluation and determined the patient's baseline mobility status using the MOVE protocol's Early Mobility Assessment Algorithm. Nurses and physical therapy documented the patient's mobility findings into the EHR. Patients were classified as a Mobility Level A, Mobility Level B, or Mobility Level C. The evaluation was then communicated to the patient's healthcare team. A mobility goal of three mobilizations per day was established as per the original MOVE protocol research [9-11].
The nurses and physical therapists were responsible for implementing progressive mobilization techniques, mobilizing patients from lying in bed to ambulating as tolerated. Prior to each time a patient was mobilized, the nurse or physical therapists would determine the mobilization attempt's safety by conducting the pre-established MOVES assessment. Patients that pass the safety assessment would progress into the mobilization event. The nurse evaluated the patient's ability to mobilize and documented the mobility episode in the EHR. If the patient did not pass the safety screening, the mobilization attempt was terminated and documented. During the mobilization, if the patient demonstrated intolerance, the mobility event was terminated, and the patient was assisted back to their room.
Instruments utilized in this quality improvement project included the MOVE protocol and Early Mobilization Assessment Algorithm. The MOVE protocol is an evidence-based intervention that is integrated into the daily care of elderly patients to improve mobility. The protocol focuses on using a multidisciplinary approach to complete a mobility assessment within 24 hours of the decision to admit, utilizing progressive and scaled mobilization, and mobilizing patients three times a day [9-11]. Integration of the MOVE protocol incorporates the use of the Early Mobilization Assessment Algorithm [9]. The algorithm classifies mobility as a following:
• Mobility Level A -Ambulates with or without assistance,
• Mobility Level B - Transfers from bed to chair,
• Mobility Level C - Confined to the bed.
The reliability of this instrument is good with a high interrater agreement score (kappa 0.83) [9-11].
The data source for this project is the EHR. Using EHRs have been confirmed to be a reliable source of information, evidence by an intraclass correlation coefficient of 0.85 [14]. An EHR serves as a platform to collect documentation from nurses, physical therapists, and nursing assistants regarding patient mobility.
The project site's IRB authorized conduction of this quality improvement project. Written consent was not required due to mobility being an expected part of treatment. However, patient and family education were completed by the nurse and physical therapist on progressive mobilization and mobility goals.
For this quantitative quasi-experimental project, data was extracted from four weeks pre and four weeks post-implementation of the MOVE protocol. The project data was evaluated for integrity and underwent cleaning prior to being imported into Statistical Package for Social Sciences (SPSS), version 24 for analysis. The independent ordinal categorical variable was the MOVE protocol, while the dependent variable was length of stay (LOS). Length of stay was considered a ratio variable because it had an absolute zero, and a ratio can be formed between values.
After reviewing data entries for errors, descriptive statistics were produced for all variables. Gender, principal diagnosis, and the levels of mobility were described using counts and percentages, while mean and standard deviation (SD) were used for LOS and age. Categorical variables were analyzed using Pearson's Chi-square test, while the Mann-Whitney U test was employed for continuous variables. All statistical comparisons were pre- versus post-implementation of the MOVE protocol. A p-value of less than 0.05 was required for statistical significance.
The pre-implementation group consisted of 126 patients, were predominately female (n = 73, 57.9%; males, n = 53, 42.1%), and ranged in age from 65 to 97 years, with an average of 77.25 years (SD = 8.16). Among this sample, the most common diagnosis was a fracture (n = 37, 29.4%), followed by sepsis/infection (n = 22, 17.5%), and osteoarthritis (n = 19, 15.1%). Table 1 reveals age distribution among the groups.
Table 1: Age distribution. View Table 1
The post-implementation group included 106 patients with a slight majority of females (n = 55, 50.9%; males, n = 53, 49.1%). These patients ranged in age from 65 to 98 years, with an average of 76.16 years (SD = 8.28). The most common diagnosis for this group was also a fracture (n = 27, 25%) followed by osteoarthritis (n = 17, 15.7%) and sepsis/infection (n = 13, 12%). Table 2 presents counts and frequencies of participant gender and primary diagnosis for pre- and post-implementation groups.
Table 2: Gender and primary diagnosis counts and percentages. View Table 2
Pre- and post-implementation groups were homogeneous on gender, chi-square p-value = 0.283 with no cells having had an expected value < 5. Since age was homoscedastic (Levene's Test p-value = 0.848) but non-normal (Shapiro-Wilkes p-value = 0.001 & < 0.0005 for pre & post, respectively), the Mann-Whitney U test was employed and revealed no statistically significant difference on age between project groups (p-value = 0.271). Both the shape and range of the age distribution were similar between project groups. No outliers were identified for either group. Figure 1 illustrates the distribution of the age variable across the groups.
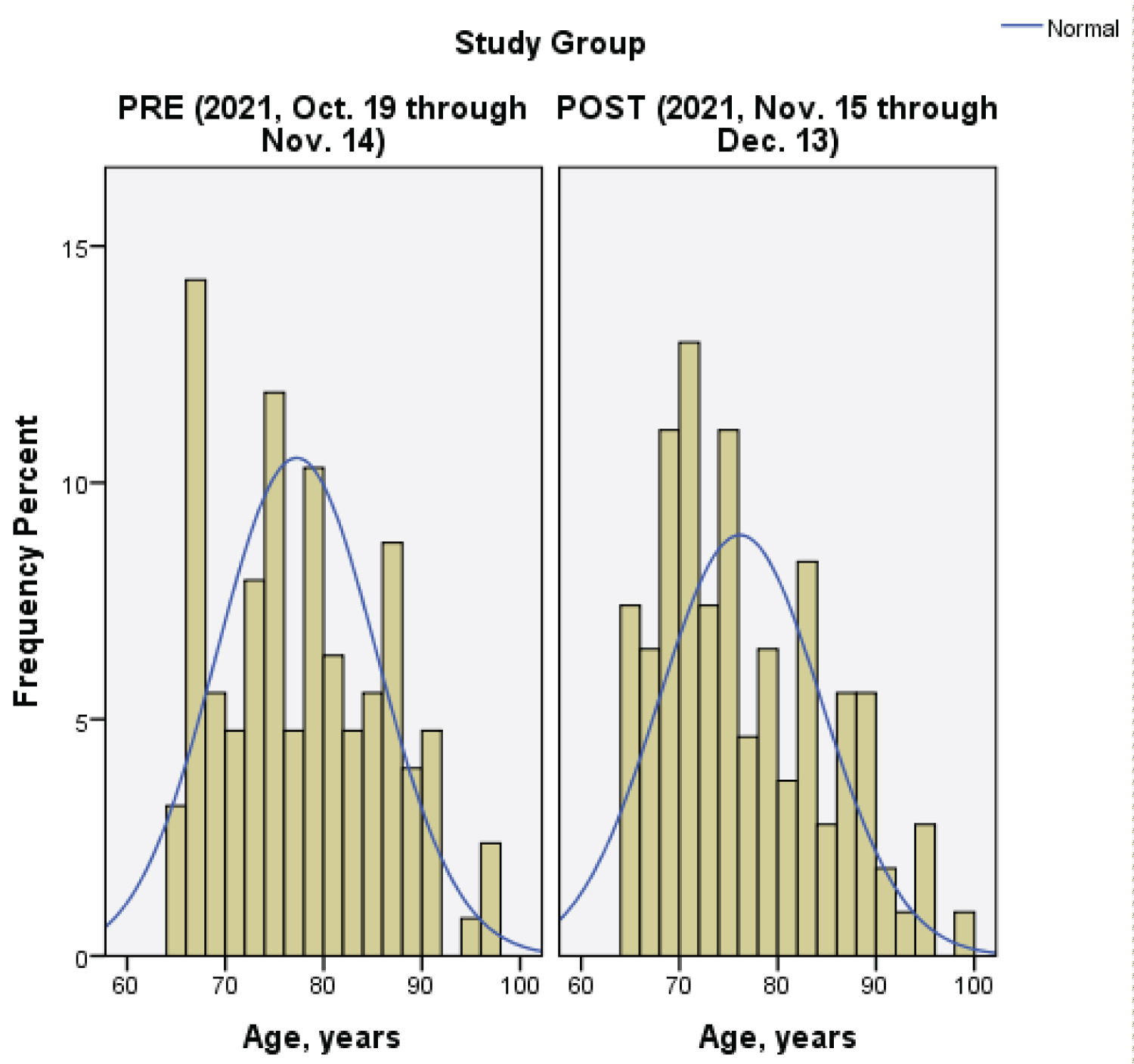 Figure 1: Histograms of age by project group.
Figure 1: Histograms of age by project group.
Note: The histogram depicted data distribution of the percentage of elderly patient age.
View Figure 1
Length of stay was also homoscedastic (Levene's Test p-value = 0.477) and non-normal (Shapiro-Wilkes p-value = < 0.0005 for pre- and post-implementation). A positive skew of similar shape and magnitude was observed for both groups (skewness = 4.031 and 2.299 for pre- and post-implementation, respectively). A similar number of minor outliers were identified for both groups, three for the pre-implementation group and four for the post-implementation group. The pre-implementation group had three more major outliers than the post group (4 vs. 1, respectively). Very nearly 94% of patients in each group had a LOS of ≤ 10 days, with the remaining data points ranging from 12 to 38 days, thus producing positively skewed non-normal distributions for both groups.
Given non-normality with similarly shaped distributions, the Mann-Whitney U test was employed and revealed no statistically significant difference on LOS between the pre- and post-implementation groups (U = 7,615, z = 1.6, p-value = 0.112, with a small effect size r = 0.11). The mean rank of the post-implementation group was larger (125.01) than the pre-implementation group (111.06). Furthermore, the median LOS was also more in the post (Mdn = 4.9 days) than pre (Mdn = 4.3 days) (Figure 2).
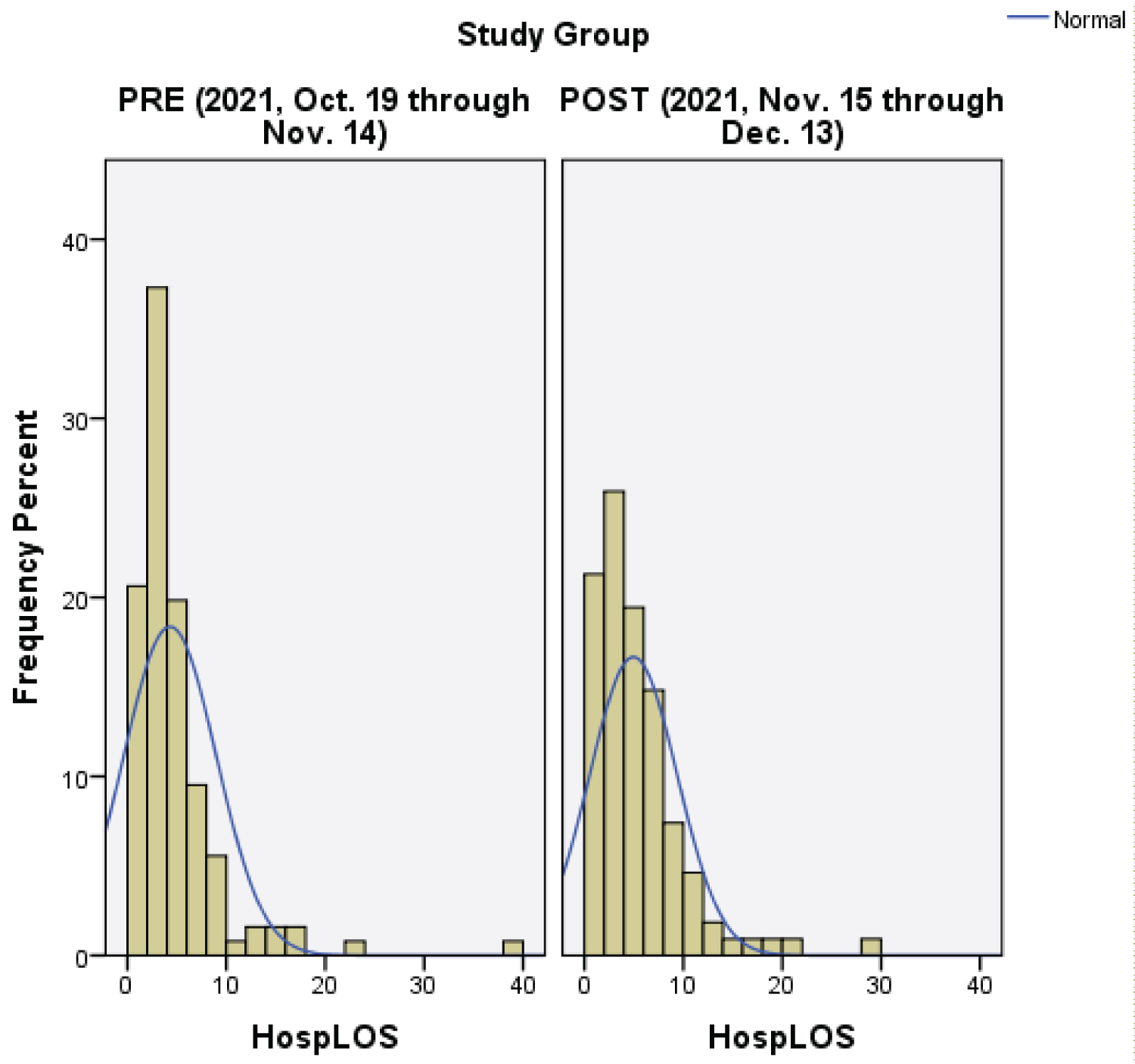 Figure 2: Histograms of length of stay by project group.
Figure 2: Histograms of length of stay by project group.
Note: The histogram illustrated data distribution of the percentage of days elderly patients were hospitalized on a medical-surgical nursing unit.
View Figure 2
Mobility among the pre- and post-implementation groups was measured to determine if the MOVE protocol had an impact. Daily mobility statuses were determined by nurses and physical therapists according to the MOVE protocol's Early Mobilization Assessment Algorithm [9]. A total of three mobility levels were utilized for this quality improvement project. Patients that ambulated, with or without assistance, were classified as a Mobility level A. Mobility level B meant patients were able to transfer from a bed to a chair. Participants that remained in bed were identified as a Mobility level C. Table 3 presents the mobility findings.
Table 3: Mobility level frequency (days) of the pre- and post-implementation groups. View Table 3
Pre-implementation group documentation illustrated that Mobility level A (n = 281, 52.9%) was the most prevalent, followed by Mobility Level C (n = 126, 23.7%) and Mobility Level B (n = 11, 2.1%). A total of 113 patient days (21.3%) were found to have missing documentation. The level of mobility most documented for the post-implementation group was Mobility level A (n = 234, 49.1%), followed by Mobility level C (n = 131, 27.5%) and Mobility level B (n = 2, 0.4%). Days with missing documentation totaled 110 patient days (23.1%). Elderly patients in the pre-implementation group experienced more days with Level A mobilization events (n = 281) compared to the post-implementation group (n = 234). Days that a patient achieved three mobilizations on a single day were measured. The pre-implementation group achieved 348 days among 115 patients, which was more than the post-implementation group, 301 days for 94 patients. Furthermore, the pre-implementation group achieved 1,043 mobilizations, while the post-implementation group had 903 mobilization events. This result indicates that the pre-implementation group had higher counts and frequencies of mobility than the post-implementation group.
Prolonged LOS due to immobility is an ongoing problem among elderly patients. The project site experienced an ongoing trend of lengthy hospitalization in older patient populations.
Therefore, this quality improvement project aimed to improve elderly patient LOS by implementing the MOVE protocol.
The results from this quality improvement project were different from the original research of the MOVE protocol. The median LOS for the pre-implementation group (Mdn = 4.30) was shorter than for the post-implementation group (Mdn = 4.94). Mobility was expected to improve in the post-implementation group. Prior original MOVE protocol research indicated increased elderly patient mobilization frequency [9]. This quality improvement project did not experience this outcome. Elderly patients mobilized with or without assistance three times daily were fewer in the post-implementation group (n = 903) than the comparative group (n = 1,043). There were a considerable number of days in which mobilization documentation was missing from the patient's EHR. This variable could have led to different results.
The pre- and post-implementation group contained higher volumes of patients that were admitted due fractures and osteoarthritis. These physical conditions are directly linked to mobility challenges because of structural changes to bone and cartilage. Also, pain is also common among with these diagnoses which will affect elderly patient mobility. Other patient factors, such as comorbidities, prior health history, baseline mobility status, and hospitalization complications can be attributed to mobility and length of stay obstacles.
A significant challenge affecting hospitals across the globe is the ongoing COVID-19 pandemic. This public health issue created barriers that hindered inpatient care. Nurses and physical therapists were restricted in their ability to care for patients because of limited PPE. Patient care was clustered in effort to prevent transmission between patients and staff. Limited staff contributed to results that were observed. External and travel nurses substituted for nurses that left the organization.
Elderly discharge planning was impacted during this project. Due to COVID-19, external facilities required patients to have a negative COVID-19 Polymerase Chain Reaction (PCR) test. This requirement resulted in patients staying the hospital extra days because of pending tests. Patients that tested positive had to remain in the facility for an extra 10 days and remain asymptomatic per CDC guidelines. Overall, the COVID-19 pandemic has adversely affected staffing and consequently LOS in many institutions in general. Implementation of this protocol in a single institution and on a single unit may have also been adversely affected.
The clinical significance of this project is noteworthy. This project combined the expertise of two healthcare disciplines to target an ongoing problem affecting elderly patients on a specific nursing unit. The adoption of the MOVE protocol provided a means for nursing and physical therapy services to communicate and achieve patient needs. Elderly patients are vulnerable to the effects of immobility, and efforts to improve mobility and functional status are necessary. This project suggested that the MOVE protocol maybe a worthy tool to enhance interdisciplinary collaboration and patient experience.
Elderly patients received a thorough mobility assessment from both nursing and physical therapy which led to more individualized care. A key finding from this project was that a portion of elderly patients were mobilized three times a day after the integration of the MOVE protocol. This finding was illustrated by the levels of mobility that were documented during each patient hospitalization. The implementation group experienced a total of 301 times in which the mobility goal of being mobilized three times within a single 24-hour period was achieved. Therefore, these patients that achieved a higher a degree of mobility were more likely to avoid the harmful effects of immobility. Also, the findings suggest that continued utilization of the MOVE protocol may enforce the need for mobility to improve LOS.
This quality improvement project is the first known initiative to implement the MOVE protocol within the United States. MOVE projects have been previously conducted in several Canadian health systems. Also, this adaption of the MOVE protocol is the first to facilitate mobilization care within an elderly trauma population.
This quality improvement project focused on prolonged elderly LOS and the absence of a multidisciplinary approach to early mobility. The findings suggest that continued utilization of the MOVE protocol may enforce the need for mobility to improve LOS. The MOVE protocol might have had greater efficacy if there were no staffing difficulties within the project site on the designated nursing unit. In addition, had there not been higher volumes of patients to available nurses, nurses may have had more opportunities to assist patients with progressive mobilization or documents correctly. Overall, under non-pandemic circumstances, the project results could have been different and indicated a more precise answer to the proposed clinical question. Moreover, the MOVE program was implemented on a single medical-surgical nursing unit. Implementing the MOVE protocol on the remainder nursing units at the project site can potentially improve the results.
This quality improvement project contained limitations which impacted the results. The project was limited by using a single nursing unit within a single project site. This setting reduced the total population size from which it can be sampled. The timeframe of the project adhered to four weeks of MOVE protocol implementation which reduced the number of patients that were able to receive the MOVE protocol. Another limitation centered on data retrieval from an EHR. The data collected imposed the risk of the healthcare team incorrectly documenting data or the information being collected incorrectly. Lastly, inability to control for external variables such as lack of patient cooperation, presence of delirium, high patient acuity, and the COVID-19 pandemic affect early mobilization delivery and practice.
The first recommendation involves expanding the quality improvement project to the remainder of the nursing units at the project site. Integrating the MOVE protocol throughout the project site creates the opportunity to improve patient care outcomes. All elderly patients admitted to the project site would receive a standardized mobility assessment and have opportunities to participate in daily mobilizations. This quality improvement project was implemented for a short timeframe. The lack of statistical significance suggests it could be recommended to engage the quality improvement project over a longer duration. A short implementation phase resulted in a small sample size. Lengthening future quality improvement projects allow for larger sample sizes. Together, these recommendations would broaden and diversify the population to which the MOVE protocol would be applied.
Early mobilizations practices are essential for maintaining elderly patient mobility. It is recommended that healthcare facilities institute a formal mobility program. Standardized mobility programs offer nurses and other healthcare professionals the ability to ensure quality care is administered to patients. This project and literature illustrate that programs like the MOVE protocol produce positive outcomes and improve patient health [9]. Overall, the healthcare team and patients would benefit from having a program that addresses the mobility needs of patients.
The IRB of the project site approved completion of this quality improvement project.
Authorization was granted by Alekhya Johnson from the Regional Geriatric Program of Toronto.
This quality improvement project did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
We thank Thomas Simunich of Conemaugh Memorial Medical Center – Duke Life Point whose work made this project possible.
None.
All authors had equal contribution to towards this manuscript.