Purpose: To evaluate the initial implementation effectiveness of an ambulatory blood pressure monitoring (ABPM) protocol based on provider perception through survey and assesses its fidelity, adoption, and impact in an academic outpatient clinic.
Methods: A prospective study was conducted. A protocol was created to implement an ABPM device for use in patients who qualified in the clinic. Providers and staff were educated on the workflow steps and the importance of utilizing ABPM to detect and manage hypertension (HTN). Surveys were distributed before implementation of the protocol and two months after the initial implementation date. The primary outcome was a change in the composite provider survey score.
Results: Thirty-two pre-surveys and 13 post-surveys were collected. The majority of pre-survey and post-survey responses were completed by post-graduate year three resident physicians (28% vs. 36% respectively). Eighty-five percent and 92% of providers had zero to five years of experience for pre-survey and post-survey responses, respectively. Following the ABPM protocol implementation, the composite provider score increased from a pre-survey score of 25 to a post-survey score of 32 (p = 0.0024).
Conclusion: Education is a critical component in creating a new service, and the support of all clinic providers and the staff was vital in a successful implementation. With proper dissemination and education, provider perception of ABPM was positive, and the tool's interest grew.
Ambulatory blood pressure monitoring, Hypertension
ABPM: Ambulatory blood pressure monitoring; BP: Blood pressure; CVD: Cardiovascular disease; HTN: Hypertension
Cardiovascular disease (CVD) is the leading cause of death for adults in the United States (U.S.), accounting for one in four deaths [1]. Hypertension (HTN) is a significant risk factor for CVD and increases stroke and myocardial infarction risk. It is estimated that 45.6% of U.S. adults have HTN, and for patients taking antihypertensive medications, over half (53.4%) are above their goal blood pressure (BP) [2]. Control of high BP is an area of focused interest for many institutions and is a quality measure evaluated by the Centers for Medicare and Medicaid Services [3].
Clinic BP measurements have been the main stay for diagnosing and assessing HTN for decades. However, discrepancies may arise in patients with masked HTN, defined as normal BP in an office setting with elevated out-of-office BP readings, or white coat HTN, defined as elevated BP readings but normal readings when measured outside the office [4]. Use of ambulatory blood pressure monitoring (ABPM) is reasonable to screen for the presence of white coat HTN or masked HTN [4]. The current national guideline for hypertension recommends incorporating ABPM into the routine care of patients' HTN, particularly for cases of suspected white coat and masked HTN, questions have arisen on how to best implement this service [4].
Several studies have demonstrated the clinical impact of ABPM, though its use is relatively infrequent [5]. In a study evaluating theoretical barriers to implementing ABPM in a clinic, several themes were identified, including environmental context and resources, beliefs about capability and consequences, cognitive skills, and knowledge [6]. Studies outlining ABPM protocols have been published. However, none have evaluated the effectiveness of their protocols in their respective practice settings [7,8].
The purpose of this study is to evaluate the implementation of an ABPM protocol through a survey of provider perception and to assess fidelity, adoption, and impact of an ABPM protocol in an academic outpatient clinic.
A prospective cohort study was conducted from January 2020 to March 2020, in the TTUHSC Department of Family and Community Medicine Clinic in Amarillo, TX. Providers included faculty physicians, resident physicians, and nurse practitioners, and willingness to participate was addressed via the completion of the study survey. Study personnel were excluded from participation in the study. The TTUHSC Institutional Review Board approved this study as exempt research.
First, educational in-services reviewing the proposed ABPM protocol were presented to faculty physicians, resident physicians, nurse practitioners, and administrative staff during two sessions. At that time, pre-surveys assessing provider opinions on ABPM utility, personal knowledge, and resources were distributed. Subsequently, nurse training in-services were provided to review the proposed workflow and educate nurses on using the ABPM device. Following two months of implementation, identical post-surveys were individually distributed to providers.
The ABPM protocol implemented in the TTUHSC Family Medicine clinic is nurse-driven and was developed with the clinic's workflow in mind. Documents were provided to assist in executing the protocol, including a workflow diagram (Figure 1). First, providers identified candidates for ABPM. A guidance document reviewing the inclusion and exclusion criteria for ABPM candidacy was provided. Inclusion criteria included suspected white coat HTN, masked HTN, or resistant HTN, and residence in Amarillo or Canyon, TX. Exclusion criteria included inability to return the machine within 48 hours or unwillingness to wear the ABPM monitor for 24 consecutive hours. Also, reimbursement information was provided on the guidance sheet.
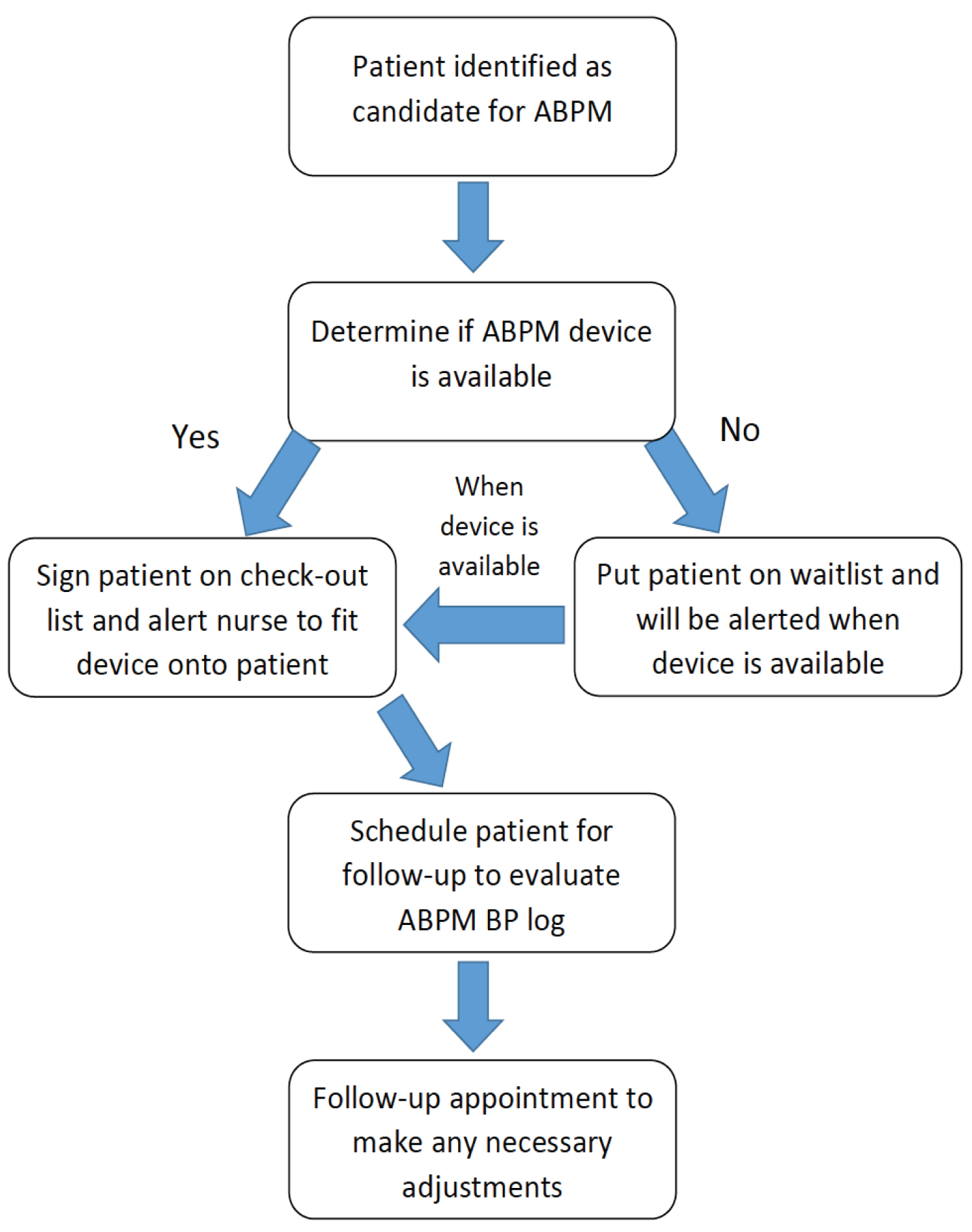 Figure 1: Ambulatory blood pressure monitoring workflow.
View Figure 1
Figure 1: Ambulatory blood pressure monitoring workflow.
View Figure 1
Upon identification of an ABPM candidate, the provider requested a nurse's assistance to fit the ABPM monitor, provided written and verbal information on the device and ABPM monitoring, and completed administrative paperwork and instructions necessary for device checkout and return. After the patient wore the device for 24 hours and returned it to the clinic, a nurse downloaded an ABPM report for the provider to review. Providers then follow-up with the patient regarding any necessary changes.
The primary outcome was the change in provider composite survey score before and after implementing the ABPM protocol. A survey was created with eleven items based on implementation science domains, including familiarity and appropriateness of setting (Table 1). Items were rated based on a Likert-scale (1 = strongly disagree; 5 = strongly agree), and statements were worded in a manner that correlated a positive response with a higher number score. In addition to scaled responses, an open section in which participants could write comments or questions was included at the end of the survey. Anonymous paper surveys were distributed and collected at the beginning and end of the study period. Secondary outcomes included factors to assess fidelity and adoption of the protocol. These factors included the number of complete 24-hour ABPM reports, length of time the ABPM device was in patient's possession, number of patients signing acknowledgment form, number and percentage of providers utilizing the ABPM machine, and number of medication changes following ABPM report. Patient characteristics, including diagnosis relevant to ABPM use, payer status, and HBPM, were also assessed. Secondary outcomes and patient characteristics were collected through a review of an ABPM device tracking record.
Table 1: Survey respondent demographics. View Table 1
A power analysis for a paired sample t-test was conducted to determine a sufficient sample size using an alpha of 0.05, a power of 0.80, a medium effect size (d = 0.5), and two tails. Based on the assumptions above, the desired sample size was 35 survey participants.
The primary outcome was assessed using descriptive statistics and analyzed using the Wilcoxon Rank Sum test. Subgroup analyses were performed using the Wilcoxon Rank Sum test for individual item analysis and Fisher's exact test for differences between groups based on provider status and years of experience. Descriptive statistics were used to assess secondary outcomes and patient characteristics. Statistical analyses were performed using Stata version 16 software (College Station, TX).
Thirty-two pre-surveys and 13 post-surveys were collected. Demographics of pre- and post-survey respondents are shown in Table 1.
A positive change in total provider survey score was demonstrated before and after ABPM protocol implementation (median composite Score 25 vs. 32; p = 0.0024; Table 2). Upon individual analysis of survey items, all statements except for perception of ABPM "as a standard BP measurement method," a "widely used tool in practice," and "having enough time and resources available" demonstrated a statically significant positive change in provider perception. Years of experience (median 0-5 years of experience for pre-surveys vs. 0-5 years of experience) and provider status (e.g., faculty, resident year, nurse practitioner) did not have a significant impact on the post-survey scores (p = 0.524 and p = 0.807, respectively).
Table 2: Survey items and primary outcome results. View Table 2
A few providers wrote comments expressing their predictions and questions on the protocol. Summarized concerns described in pre-survey comments included availability of resources and time, patient compliance, lack of education for providers and patients, and insurance reimbursement. Suggestions on successful implementation strategies included education, experience with use, training, and staff participation. Post-survey comments noted patient compliance, availability of the ABPM device, time, and prioritization of patients as barriers to utilizing the device. Suggested changes included more provider education and purchasing additional ABPM devices.
Six out of 38 (16%) eligible providers in the clinic utilized the ABPM device for their patients, and 8 patients completed ABPM testing per the project protocol. Two providers requested the device for two patients, while the four remaining providers each requested the device for one patient. Eight documented patients utilized the machine. One patient's chart did not contain any active encounters, and data regarding diagnosis, home blood pressure monitoring, and medications changes could not be collected. All patients utilized home blood pressure monitoring (HBPM) and had a history of HTN or elevated BP. Patients followed instructions and returned the ABPM device within 48 hours, except one patient returned the device in 52 hours. All patients except one completed the 24-hour monitoring and signed an acknowledgment form.
Overall, the proposed ABPM protocol was well received by clinic providers and staff. Furthermore, upon exposure to an ABPM protocol, provider perceptions of the device were positive. While an initial protocol was introduced, changes were made during the months in which it was implemented as questions, and unpredicted scenarios arose. The changes included guidance on prioritizing patients utilizing the device, a cleaning procedure for the device, and resources on ABPM for nurses. Although education was provided during meetings on the procedure, additional training was still requested for users to become familiar with the process. Once acquainted with the device and procedure, a few providers and nurses became "champions" utilizing ABPM for patients.
In the initial month of implementation, the usage rate was steady, though lower than anticipated. Later in the implementation period, a dedicated education session on out-of-office blood pressures was presented to faculty physicians, which appeared to spark interest in the ABPM machine once again. The demand for the device increased considerably following the lecture. While interest grew anecdotally, the device's actual use did not always follow, which may be partially due to the availability of only one device in the clinic.
Our study demonstrated several strengths. An outpatient teaching clinic was an ideal setting to implement a new service, given the practice's academic nature. The openness of the clinic providers and staff also allowed for easier adoption of the protocol. In addition to the clinic's open-mindedness, staff were involved in the protocol's execution and played a significant role in the modifications of the protocol. During the in-services, thoughtful questions arose, which led to changes to improve workflow and meet the clinic's needs.
The study has several limitations. First, regarding pre-surveys, a few providers completed the survey as the education on the ABPM protocol was provided, which could have influenced results. Notably, the knowledge and familiarity statements could have been affected by the training provided; although, both of these items showed statistically significant improvement. Overall, the protocol was adopted reasonably well, and its steps followed appropriately. However, a few data points were missed due to a lack of documentation, which affected the adoption and fidelity of the protocol. One of the inclusion criteria was the patient's definitive ability to return the device, which implies good fidelity of the protocol. While this criterion may have affected secondary results, it was necessary given the high cost of the device and the large number of patients living in rural areas, which could affect their reliability to return the device within 48 hours. If devices become more affordable and concern for their losses less significant, the service could be provided to a larger patient population. A small group of providers utilized the device, although all were exposed to the proposed workflow. Therefore, only a small number of patients were equipped with the device.
The most significant limitation of the study was the low overall subjects being able to use the device due to the coronavirus pandemic's impact on clinic services. At the pandemic's height, in-person chronic care management visits were severely curtailed, and the clinic transitioned to a telehealth platform. As a result, in-person visits and the ability to fit and utilize the ABPM monitor were not feasible. Also, due to social distancing recommendations, in-person group meetings were canceled, which affected how surveys were collected. Distributing and collecting surveys is difficult, and with the coronavirus pandemic, the collection of surveys became more difficult as priorities changed for providers. Another limitation of our study was the lack of a tracking method for surveys that could have otherwise assessed the change in individual provider scores.
As clinic operations resume normal functions, revisions will be made to implement the ABPM protocol to adapt it to fit clinic needs. The purchase of additional devices was also a popular request by providers in the clinic, which may assist in bridging providers' interest and increasing the actual use of an ABPM device. Following more data on ABPM use in the clinic, examining costs and clinical outcomes would be possible.
Education is a critical component in creating a new service, and the support of all clinic providers and the staff was vital in a successful implementation. With proper dissemination and education, provider perception of ABPM was positive, and the tool's interest grew. Future studies should consider a multicenter design to recruit more providers and develop a tracking method for surveys to evaluate change in individual provider perception prior to and after implementation. Studies may also consider evaluating patients' perceptions of ABPM as the patients' participation is necessary for successful use. With additional studies to identify the best protocol framework, more healthcare centers may consider using ABPM and the underutilized tool will become standardized practice in managing patients' BP.
The authors would like to thank Ronald Hall, Pharm.D., M.C.S.C., for assisting with statistical analyses.