Oral or nasal foreign bodies are a common hospital problem within otolaryngology with an incidence which most often occurs in the pediatric population [1]. Foreign bodies in adults are fairly uncommon with people aged 50 or older making up less than 10% in one case series [1] with most representing inorganic objects. Foreign bodies of the nose in adults remain rare [1]. Removal is often straightforward and major complications are rare when dealing with nasal foreign bodies [1].
Endovascular coiling complications remain relatively uncommon with only 2.7% of patients experiencing clinically significant morbidity, most commonly either intraoperative or immediately post-operative [2]. Several cases (Table 1) [3,4] have been reported in the literature following endovascular coiling of a traumatic pseudoaneurysm presenting within 6 weeks of coiling. Others have reported this as a late complication 10 years after coiling [5].
Table 1: Summary of reported patients suffering endovascular coil erosions following treatment of pseudoaneurysms of the carotid artery. View Table 1
It is important to recognize that attempts to remove the coil in clinic may potentially result in vessel rupture, bleeding and stroke. This is in contrast with most nasopharyngeal foreign bodies, which can usually be retrieved without serious complication [1]. Treatments for endovascular coil erosion in cases reports of traumatic pseudoaneurysms have involved trimming the extruded coil at the level of the defect while leaving the embedded portions in place [3-5]. This can be applied to endovascular coil erosion in true aneurysms as well and represents a pragmatic approach to treatment. Open surgical removal should only be considered in treatment failure.
Endovascular coil erosion, Nasal foreign body, Nasopharyngeal foreign body, Internal Carotid artery aneurysm
EVC: Endovascular Coiling; CT: Computed Tomography; FoR: Fossa of Rosenmuller; ET: Eustachian Tube
A 72-year-old male presented to a tertiary care academic Otorhinolaryngology clinic with a 1-month history of throat irritation. He reported recently finding a hair like object irritating his uvula that he was able to pull on and partially fracture. His past medical history is relevant for an internal carotid artery aneurysm that required endovascular coiling 6 years prior (Figures 1, Figure 2 and Figure 3). The physical exam was largely normal except for the nasal endoscopy, which demonstrated a thin black filamentous tissue extruding from the left Fossa of Rosenmuller (Figure 4) tracking down into the oropharynx. On contrasted CT imaging (Figure 5), a dilated left internal carotid aneurysm was present with coiling material causing local mass effect and mild narrowing of the nasopharynx and oropharynx (Figure 6).
 Figure 1: Contrasted CT Image, axial cut. Identification of a 3 cm saccular aneurysm of the left internal carotid artery. Calcifications suggestive of chronic disease. There is a lack of soft tissue inflammatory change seen in traumatic etiologies. View Figure 1
Figure 1: Contrasted CT Image, axial cut. Identification of a 3 cm saccular aneurysm of the left internal carotid artery. Calcifications suggestive of chronic disease. There is a lack of soft tissue inflammatory change seen in traumatic etiologies. View Figure 1
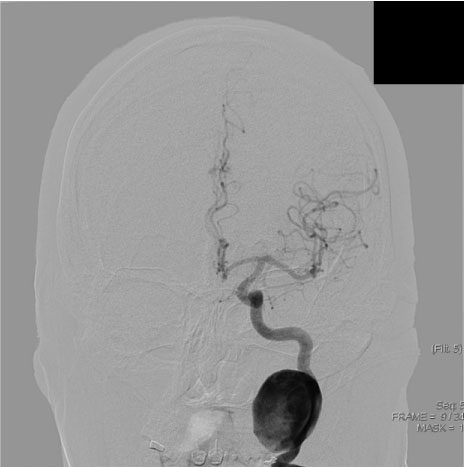 Figure 2: Pre-coiling digital subtraction angiography (DSA) demonstrating a 3.5 by 2.7 cm aneurysm of the cervical segment (C1) of the internal carotid artery. View Figure 2
Figure 2: Pre-coiling digital subtraction angiography (DSA) demonstrating a 3.5 by 2.7 cm aneurysm of the cervical segment (C1) of the internal carotid artery. View Figure 2
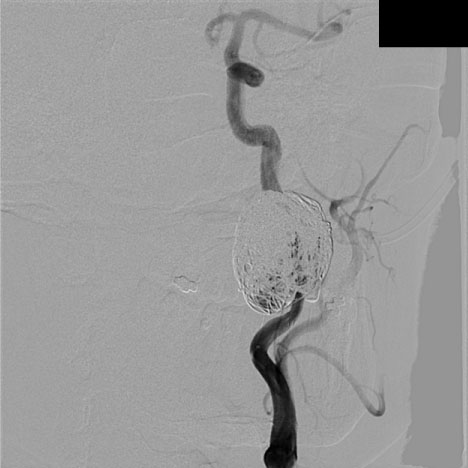 Figure 3: Post-coiling digital subtraction angiography demonstrating occlusion of the aneurysm with minimal residual flow. A total of 22 Penumbra coils were deployed. Following the initial 3 coils, an Enterprise stent was deployed to maintain the patency of the vessel. After deployment of coiling 11 follow up runs were completed demonstrating progressive occlusion of the aneurysm. View Figure 3
Figure 3: Post-coiling digital subtraction angiography demonstrating occlusion of the aneurysm with minimal residual flow. A total of 22 Penumbra coils were deployed. Following the initial 3 coils, an Enterprise stent was deployed to maintain the patency of the vessel. After deployment of coiling 11 follow up runs were completed demonstrating progressive occlusion of the aneurysm. View Figure 3
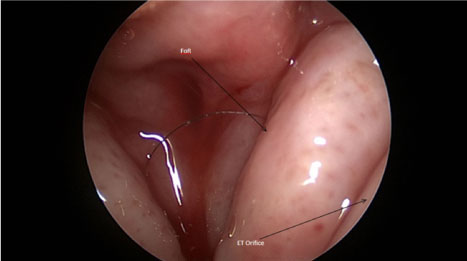 Figure 4: Platinum coil protruding into the nasopharynx from the Fossa of Rosenmuller (FoR) posterior to the eustachian tube (ET) orifice. View Figure 4
Figure 4: Platinum coil protruding into the nasopharynx from the Fossa of Rosenmuller (FoR) posterior to the eustachian tube (ET) orifice. View Figure 4
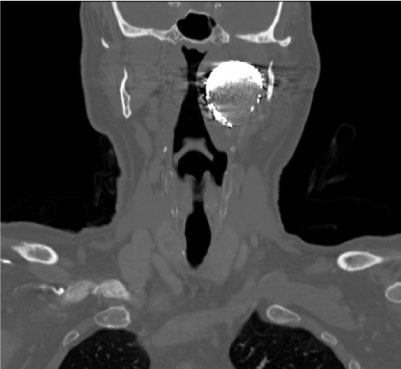 Figure 5: Contrasted CT image, coronal cut. Remonstration of the mass like coiling material. Metal artifact is present and interferes with determination of contrast enhancement of the aneurysm. There is close approximation within the nasopharynx and oropharynx. View Figure 5
Figure 5: Contrasted CT image, coronal cut. Remonstration of the mass like coiling material. Metal artifact is present and interferes with determination of contrast enhancement of the aneurysm. There is close approximation within the nasopharynx and oropharynx. View Figure 5
 Figure 6: 3D rendering of the left ICA aneurysm pre-coiling. View Figure 6
Figure 6: 3D rendering of the left ICA aneurysm pre-coiling. View Figure 6
Vascular surgery was consulted who recommended removal of the extruding filament within the nasopharynx using an endoscopic approach to reduce the potential communication with the internal vasculature. Open removal of the foreign body was reserved as a last resort given the potential significant morbidity associated with such surgery. The patient was taken to the OR. Under general anesthesia he was prepared for sinonasal surgery. Under direct visualization with a nasal endoscope, endoscopic scissors were used to amputate the filament at the mucosal junction. Post-operatively, the patient recovered without complications. Post-operative CT and angiography was ordered but never completed. On follow up examinations up to 9 months, there had been no further recurrence of symptoms, extrusion, or complications.
We present a case of a 72-year-old gentleman with an extruding internal carotid artery aneurysm coil through the Fossa of Rosenmuller. The patient was stable post-operatively and remained complication and progression free 8 months later at time of writing. Other reports involving pseudoaneurysms were found in the literature although no coil erosions in true aneurysms have been described. Conservative therapy with controlled amputation of the extruding filament in the operative room has served as sufficient treatment. Potentially catastrophic events can be avoided with the use of thorough history taking, proper imaging and judicious treatment. Long term follow-up is warranted as recurrence appears to be common (Table 1). The role of non-operative treatment and open excision is yet to be defined.
Additionally, one previously undiscussed aspect of this phenomenon is that the eroded coil served as a continued communication between a weakened aneurysm and the non-sterile nasopharynx. This environment may serve as a channel allowing the seeding of bacterial contaminants into the internal vasculature. No prior reported cases have addressed this concern. Conservative measures in cases such as these fail to address the worrisome infection risk and prophylactic anti-staphylococcal antibiotics are reasonable in the pre-operative and immediate post-operative period. Additional monitoring for prosthetic colonization and failure is likely warranted with one case report regularly following up until 6 months [5]. As endovascular coiling becomes more and more common, only time will tell if the incidence of coil erosion into the aerodigestive tract will increase. To our knowledge, this represents the only documented report within English language literature demonstrating this finding in the nasopharynx from a true aneurysm.
In consideration of the Journal of Otolaryngology and Rhinology reviewing and editing my submission, "Late Endovascular Coil Erosion of the Internal Carotid Artery into the Nasopharynx: Case Report and Review of Literature", the author(s) undersigned transfers, assigns and otherwise conveys all copyright ownership in the event that such work is published.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
All authors have no conflict of interests in the publication of this manuscript. No funding was sought in the publication of this manuscript.
This manuscript has not been submitted to any other scientific journal and the contents have never been published in any part.