Epidermal cyst of the bony external auditory canal in adults is rare. Only nine cases are reported in the literature. They occasionally tend to develop into a malignancy.
We describe a case of epidermoid cyst of the external ear canal. Although the outer ear canal was almost filled by the cyst, no bone erosion was observed. Dimensions of epidermoid cyst was 13 × 10 mm. According to our knowledge, this case is the biggest epidermoid cyst of the bony external ear canal in the literature.
Despite the rarity of coincident malignancy in an epidermoid cyst should be examined histopathologically to exclude malignancy.
Epidermoid cyst, External ear, Cyst
The epidermoid cyst is a common benign disease of the skin. Generally, it arises in hair-bearing areas such as scalp, neck, and extremities [1]. About 7% of them are found in the head and neck region. The most frequent site involved by epidermal cysts in the head and neck region is the neck, cheek, pre-auricular area, and nasal area [2]. The cyst is filled with keratin and lined with stratified squamous epithelium. They may arise from the epidermal rests during the intrauterine period, occlusion of the pilosebaceous unit, traumatic injury, or surgical implantation of epithelial elements, human papillomavirus infection, or ultraviolet exposure [3].
Epidermoid cysts of the external auditory canal (EAC) are extremely rare and generally reported at pediatric patients [4].
The epidermal cyst may be confused with, dermoid cyst, sebaceous cyst, ear polyps, carcinomas, etc. These are very rarely undergone malignant transformation [5]. The histopathological examination should be performed for differential diagnosis. We reported an adult patient with a large epidermoid cyst of the bony EAC. Informed consent was obtained from the patient. Acording to our knowledge only nine cases are reported in the literature and all of them smaller than this case.
A 35-years-old female presented with complaints of decreased hearing and fullness at the left ear. The severity of these symptoms increased gradually for 6 months. On physical examination, the left otoscopy showed a mass that was completely occluding the canal; the tympanic membrane was not visualized. The property of this mass was round, smooth, soft and covered with normal skin. The left tympanic membrane was not evaluated because of mass position at EAC. There was no discharging sinus or pointing abscess (Figure 1). There was no history of trauma, ear surgery, fever, and discharging ear. The right ear was normal.
 Figure 1: This image reveals a spherical mass on the bony portion of the left external auditory canal.
View Figure 1
Figure 1: This image reveals a spherical mass on the bony portion of the left external auditory canal.
View Figure 1
The pure tone audiometer showed conductive hearing loss in the left ear. Air-bone gap averaged over 0.5, 1, 2, and 4 kilohertz (kHz) were obtained. The air-bone gap (ABG) range of pre-operation was 27.5 decibel (dB).
Computed tomography (CT) (SOMOTOM; Siemens, Earangen, Germany) showed a 13 × 10 mm mass presenting as well-defined, low density, poorly enhanced lesion without any bony destruction (Figure 2). There is no case of epidermoid cyst in the bony external ear canal which is larger than the case presented in the literature. The mean size of the epidermoid cyst was 3.50 mm (size range, 2-7 mm) in the bony EAC cases [1].
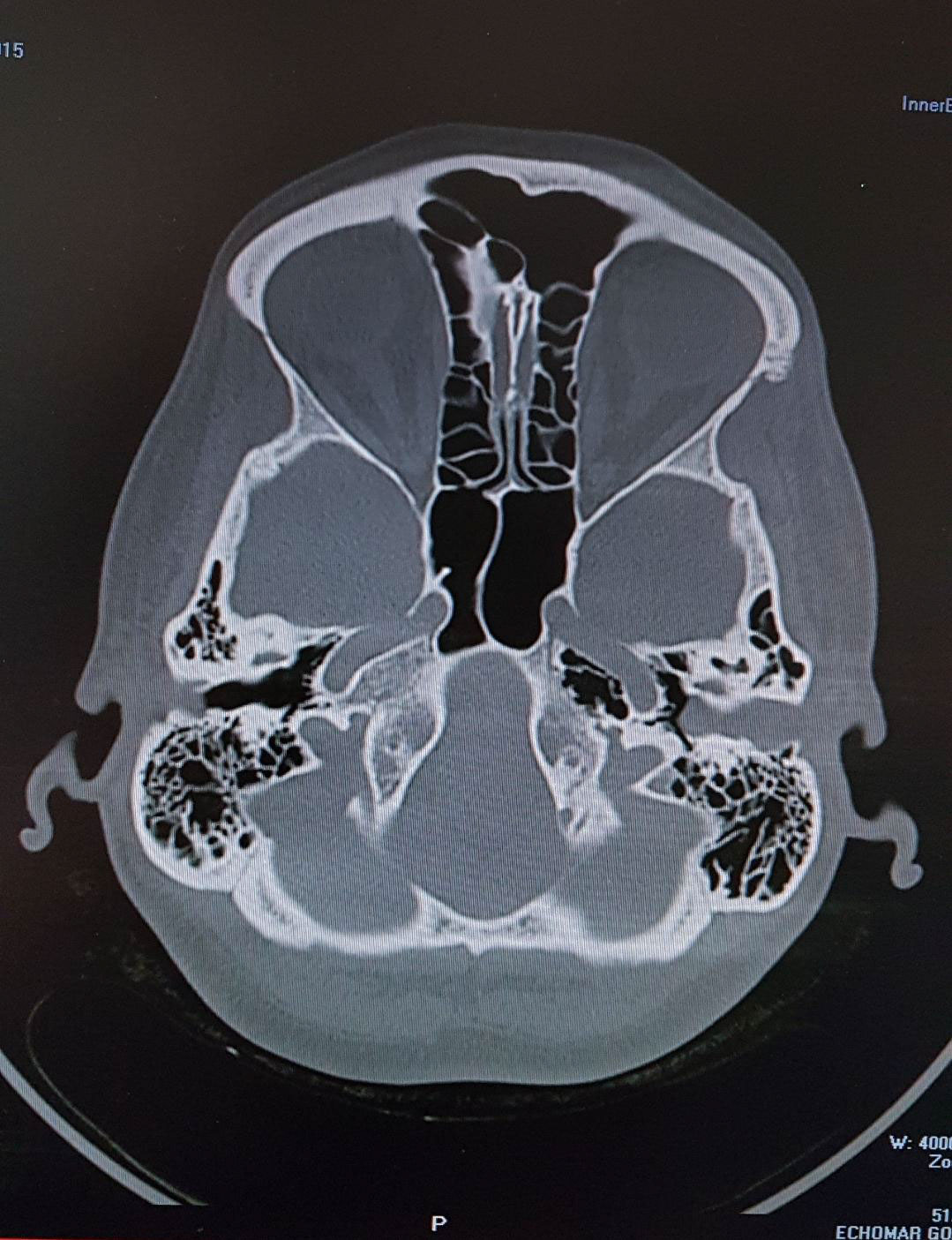 Figure 2: Temporal bone computed tomography image shows a mass on the bony portion of the EAC without bone erosion.
View Figure 2
Figure 2: Temporal bone computed tomography image shows a mass on the bony portion of the EAC without bone erosion.
View Figure 2
Middle ear structure is normal in CT examination of the temporal bone. The mass was removed transcanal approach preserving most of the skin covering the external auditory canal. The loss of the skin overlying a cyst was small so that the skin defect was healed spontaneously.
The macroscopic specimen consists of cystic mass with cheesy material. Histologically, this specimen consisted of features of the epidermoid cyst-like presence of cystic lumen lined by stratified squamous epithelium with keratin. Air-bone gap closure was achieved after surgery.
The preferred treatment for epidermoid cysts is the complete removal of the mass as we did in our patients. The patient was followed up during the next 12 months without recurrence of the lesion.
Epidermal cysts are benign neoplasms that are usually present as solitary, painless lesions. Epidermal cysts of the bony EAC are uncommon. Because there are no sebaceous glands and hair follicles at the medial part of bony EAC.
Significant time may be required before the diagnosis of these lesions. Our patient presented with progressive painless ear fullness lasting for about 6 months.
Congenital type of epidermoid cysts may result from the implantation of epidermal rest during the intrauterine period. Traumatic implementation of epidermal tissues can cause traumatic type epidermoid cysts. Idiopathic type may derive from blockage of hair follicles or sebaceous glands [6-9]. In our case, the epidermoid cyst of the external ear canal is thought to be an idiopathic type due to the lack of trauma history and the adult age of the patient.
A dermoid cyst with an epidermoid cyst can be confused with each other due to macroscopic features. Epidermoid cyst consists of keratinous cyst covered by stratified squamous epithelium without adnexal structures but the dermoid cyst contains keratin, sebaceous glands, hair follicles, and adnexal structures within the wall of stratified squamous epithelium [10]. Other lesions that should be considered in the differential diagnosis are lipoma, hemangioma, cholesteatoma sebaceous cyst, ear polyps, and carcinomas. Cholesteatoma destroys the bone through osteoclastic bone resorption and chronic inflammation, whereas the epidermoid cyst seems to erode adjacent bone by pressure necrosis. In our case, although the large size of the cyst, bone necrosis was not observed. Lipomas are benign tumor composed of fatty tissue and can present the same aspect of the epidermoid cysts. Hemangiomas are often present at birth; they are benign tumors of the vascular endothelia, which can develop spontaneously. The differential diagnosis of all these lesions can be made by histopathologic examination.
The preferred treatment for epidermoid cysts is the complete removal of the mass as we did in our case. Recurrence is rare. Complete removal of the mass is important because, in the literature, rare cases of malignant transformation of the epidermoid cyst have been reported.
Despite the rarity of coincident malignancy in an epidermoid cyst, rapidly changing in size, inflamed or painful should be examined histopathologically to exclude malignancy. Malignant transformation takes time and rate of an epidermal cyst into cutaneous squamous cell carcinoma range from 0.011 to 0.045% [5].
An epidermal cyst should be considered when evaluating any tumor of the external auditory canal. It is important to remove it completely because of the low possibility of malignant transformation.
The authors have no conflict of interests.
None.
This work received no external funding.
The authors have no funding financial relationships or conflict of interest to report. The authors received no financial support for the research, authorship, and/orpublication of this article.