Achondroplasia is the most common skeletal dysplasia which can lead to many serious complications. Obstructive sleep apnea is a common complication in achondroplasia that varies in severity levels from mild to life threatening. In this report, we present a case of achondroplasia with vascular malformation compressing the airway which caused obstructive sleep apnea.
Achondroplasia, Vascular malformation, Obstructive sleep apnea
Achondroplasia is an autosomal dominant condition caused by mutations of fibroblast growth factor receptor 3 (FGFR3) gene [1]. It is the most common skeletal dysplasia with a prevalence of approximately 1 in 20,000 live births [1]. The birth incidence is one in 10,000-30,000, and more than 250,000 individuals are affected worldwide [2]. The clinical manifestations of achondroplasia usually present from birth; including disproportionate short stature associated with enlarged head, depressed nasal bridge, short stubby trident hands, lordotic lumbar spine, prominent buttocks and protuberant abdomen [3]. Achondroplasia can lead to multiple life threatening complications including cervicomedullary compression, spinal stenosis, restrictive and obstructive lung disease, otitis media, and tibial bowing [4]. It has been estimated in a study done in Wisconsin that 10-85% of children with achondroplasia require treatment for respiratory problems, most commonly central sleep apnea, restrictive lung disease, and obstructive sleep apnea [5]. To our knowledge, there are no published cases with vascular malformation of the airway. In this report, we present a case of achondroplasia with vascular malformation compressing the airway which caused obstructive sleep apnea with a brief review of the literature.
A 5-year-old male, known case of achondroplasia was referred to otolaryngologist because of severe obstructive sleep apnea based on polysomnography findings.
His first referral to ENT was for snoring and sleep disturbance at the age of 9 months, he had grade 2 tonsillar hypertrophy, underwent fiber-optic scope which showed large adenoid, normal supraglottic area and normal mobile vocal cords.
He underwent adenoidectomy at age of 12 months with mild postoperative improvement. At age of 5 years, he was admitted because of significant sleep apnea. During this admission, he had 2 cardiac arrests due to pulmonary hypertension. He was referred again to ENT because of snoring. He underwent polysomnography which showed severe obstructive sleep apnea. Scope was done at the clinic and showed hypopharyngeal collapse with posterior extension of the tonsils and left vocal cord immobility. Neck CT (Figure 1) was requested to rule out compression over the left recurrent laryngeal nerve and showed vascular malformation (dilated carotid sheath vessels), collapse of the hypopharynx and a total collapse of supraglottic area with patent subglottic region. The option of tracheotomy was offered as the best solution for his recent situation but it was refused by the family.
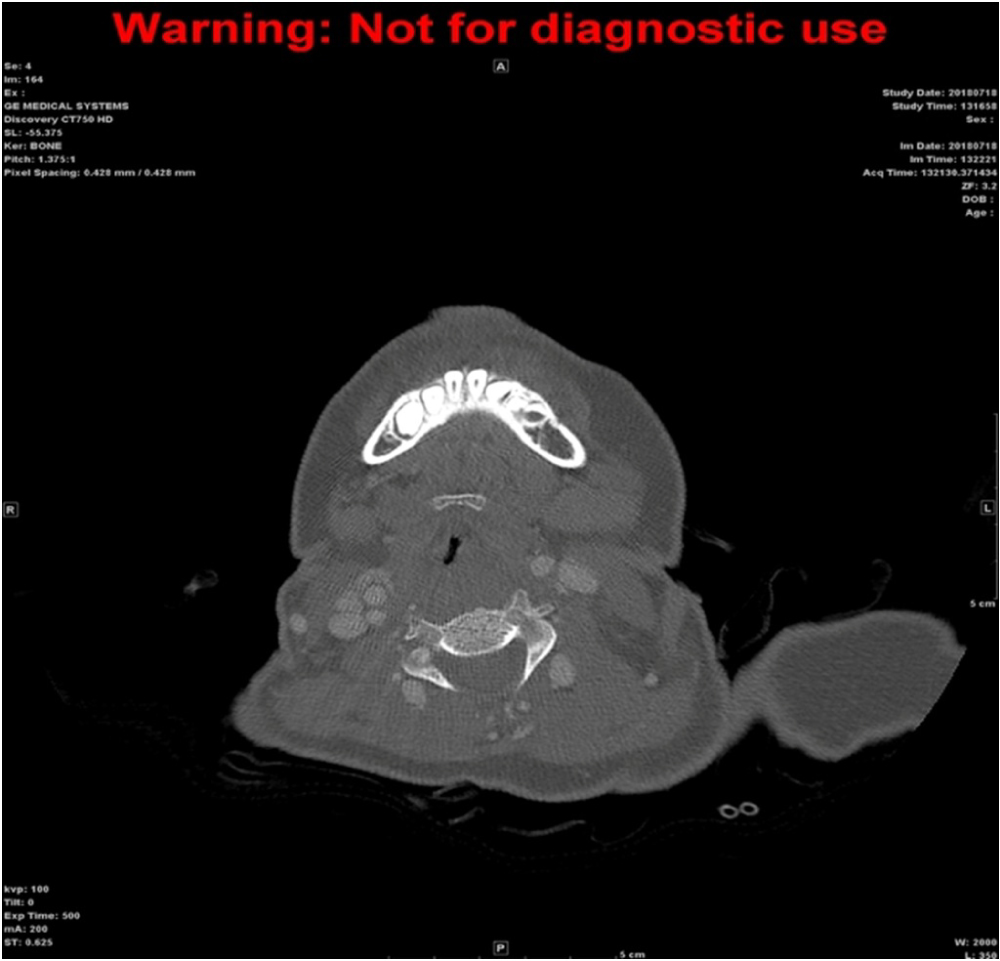 Figure 1: Image shows Airway compression by vascular malformation.
View Figure 1
Figure 1: Image shows Airway compression by vascular malformation.
View Figure 1
Obstructive sleep apnea is common in achondroplastic patients because they are prone to have small airways, midface hypoplasia, oromotor hypotonia and lymphatic ring hypertrophy [5]. Achondroplasia is complicated by sleep apnea due to many pathologies, and could be divided into central and peripheral pathologies. Central pathologies include cervicomedullary compression and narrowed foramen magnum, whereas peripheral pathologies include adenotonsillar hypertrophy [4]. Typically, polysomnography is done in cases with obstructive sleep apnea (OSA) to differentiate central, peripheral, mixed apnea and hypopnea [6]. However, In our patient, he has severe obstructive sleep apnea, central causes were ruled out after sleep study despite having narrowing of foramen magnum. He has multilevel obstruction with grade 3 tonsils causing narrowing at the oropharyngeal level and hypo-pharyngeal collapse.
Neuroimaging using computed tomography (CT) or magnetic resonance imaging (MRI) should be done to assess craniocervical junction for any stenosis and polysomnography for central apnea as soon as the patient is diagnosed with achondroplasia [7].
Interestingly, our patient has a vascular malformation of the airway that has caused hypopharyngeal collapse which was first noticed when a scope was done for him and confirmed by neck CT. Vascular malformation of the airways was not reported in any literature; however, there are 3 cases reported of achondroplastic patients with vascular malformations of the brain which lead to death, diagnosis was achieved on autopsy [8]. This finding along with our patient have necessitated the report that vascular malformations although rare but can lead to devastating outcome.
On the other hand, achondroplasia is commonly known to affect upper respiratory airways caused by disease process including combination of hypotonia, small nasal cavities and midface hypoplasia [9]. In one study done by Tasker, et al. had patients with achondroplasia were divided into 3 groups based on respiratory difficulties. The first group had adenotosillar hypertrophy and midface hypoplasia, OSA mostly resolved post adenotonsillectomy. In the second group, OSA did not resolve after the surgery; however, these patients did not require supplemental oxygen. The third group, which is the most severe form, did not benefit from adenotonsillecomy and required supplemental oxygen [9]. Study did not mention if any participant was investigated for airway vascular malformation, this could assert to the rarity of this diagnostic practice.
Achondroplasie is considered the most common genetic form of dwarfism [9]. Obstructive sleep apnea is common in achondroplastic patients [5]. Vascular malformations of the airway is rare but can increase morbidity and mortality ; therefore, proper assessment for such patient with fiber-optic scope to evaluate the airway from the nose till the glottic area is mandatory even if the tonsils were hypertrophied in oral examination. This case study findings assert to the significance of ruling out multilevel obstruction and proceed with the imaging process if needed before taking patient to theater.
Consent to publish the case report was not obtained. This report does not contain any personal information that could lead to the identification of the patient.
No funding or grant support.
All authors attest that they meet the current ICMJE criteria for Authorship.
The following authors have no financial disclosures: A. Albelali, R. Alkanhal, W. Alshiha and J. Alshammari.