Physician assistants (PAs) as medical providers have evolved since 1967 when the occupation was first established. Utilization of PAs has expanded to include procedures in multiple subspecialties. There is controversy over PAs performing in-office procedures but we propose a training paradigm to obtain competency and perform in-office procedures in Otolaryngology outpatient clinics. Consideration for state laws and facility or institution protocols is required prior to starting proctoring. However with appropriate proctorship program, treatment protocols, and annual review program PAs are capable of achieving competency. With appropriate training and patient education many of the concerns for PAs performing in-office procedures can be addressed appropriately. This helps improve access to care, expedite urgent patient needs as well as opening physician's schedules for surgical consultations and follow-ups.
Physician assistant, Procedures, Otolaryngology
The Physician Assistant (PA) profession was established in 1967 by Dr. Eugene Stead of Duke University who created a 2-year education program, similar to physician training during World War II, graduating four Navy Hospital Corpsmen [1]. The profession has grown to a work force of over 140,000 PAs in the United States and has expanded globally with Pas practicing in 15 countries [2]. As the profession has evolved, so has the acceptance of and patient satisfaction with receiving care from a PA. In 2014 a Harris poll reported 93% of patients trust PAs as a medical provider and 93% felt PAs provide excellent medical care [3]. The utilization of Pas has expanded to include PAs performing procedures in multiple subspecialties, including Dermatology, Neurosurgery and Gastroenterology [3]. This evolution has opened the pathway for PAs in Otolaryngology to expand their role with appropriate training, education, and supervision, to receive competency in performing in-office procedures such as flexible laryngoscopy, myringotomy and ventilation tube placement, fine needle aspiration of neck masses, or ultrasound-guided chemodenervation of salivary glands. PAs performing in-office procedures has been a controversial issue but we propose a paradigm to establish safety and efficacy and encourage an appropriate communication between physician and PA. This is an important evolution in the utilization of PAs to improve access to care, assist with expediting urgent patient care needs as well as opening surgeon's schedules for new consults and pertinent follow-ups.
Controversy has sparked with PAs performing in-office procedures for several reasons. First, physicians have argued PAs do not have formal specialized training to perform in-office procedures [4]. Secondly, there is concern for transparency in the PA profession with patients and the differentiation in PA versus physician [4]. Lastly, there is concern for poor outcomes and a higher risk of complications with PAs performing procedures compared to physicians [4]. While these are valid concerns, we propose a paradigm to appropriately train and proctor PAs for in-office procedures while maintaining a partnership with the supervising physician to optimize patient outcomes. Other subspecialties have been able to train and utilize PAs for procedures similarly with published success. Cox, et al. [5] performed a study of complications of pneumothorax following central venous catheters when performed by cardiothoracic surgery and pulmonary critical care team PAs which found no incidence of pneumothorax during the study. They found with appropriate training and supervision PAs could be effective and safe at performing this procedure [5]. Similarly, Gunneson, et al. [6] found that PAs could be trained and effective performing routine parenchymal liver biopsies and note that results obtained by a PA are comparable to those obtained by a physician performing the procedure [6]. These studies help demonstrate PAs are capable of being trained to perform invasive procedures without significant complications with the appropriate training paradigm and supervision.
A PA's scope of practice and ability to perform specialized procedures is largely dependent on the PA, supervising physician, and organization which employs all parties [7,8]. Each state has either individualized regulations on allowed services performed by a PA or requires approval by a regulatory board within the state. Most also require a written agreement between the PA and the supervising physician detailing the PA's scope of practice and prescriptive authority. For the states that do not have written agreements, the PA's scope of practice is typically determined by state law or the state medical board. In addition, most states currently require some level of co-signature of PA documentation as an additional means of supervision.
The oversight and proctorship for obtaining new skills is again dependent on the PA, supervising physician, employer, and state regulations [7,8]. Prior to initiating training, we recommend reviewing state law as well as the employer's permitted privileges for PAs. If allowable, the physician and PA will need to determine appropriate supervision during training to obtain competency congruent with current state regulatory requirements.
To obtain competency at our institution for in-office procedures we developed a specific training paradigm for physician assistants for each procedure. Figure 1 is an example of our training paradigm we developed for US-guided chemodenervation of salivary glands for sialorrhea. This includes completion of a 30-hour ultrasound course inclusive of hands-on training. The PA then observes the supervising physician completing consultations for sialorrhea, administering injections under ultrasound guidance, and during follow-up visits. Subsequently, the PA performs a minimum of 10 procedures under direct supervision. Once competency is acquired, hospital privileges and the written agreement are updated accordingly. Periodic review of outcomes is performed for maintenance of competency. We utilize a treatment protocol when possible to ensure the PA is following the supervising physician's standard of practice. We use an exhaustive review of the literature and patient outcomes to develop the protocols for procedures. After completion of procedures, documentation is completed and co-signature is required and completed after each encounter. Depending on the in-office procedure the paradigm will be augmented to meet the needs of adequate education and proctorship. For example, bilateral myringotomy and ventilation tube placement would require more extensive direct observation of the physician performing the procedure as well as more direct supervision of the PA performing the procedure to achieve competency. On the other hand, flexible laryngoscopy does not require as much direct observation and supervision of the PA prior to achieving competency.
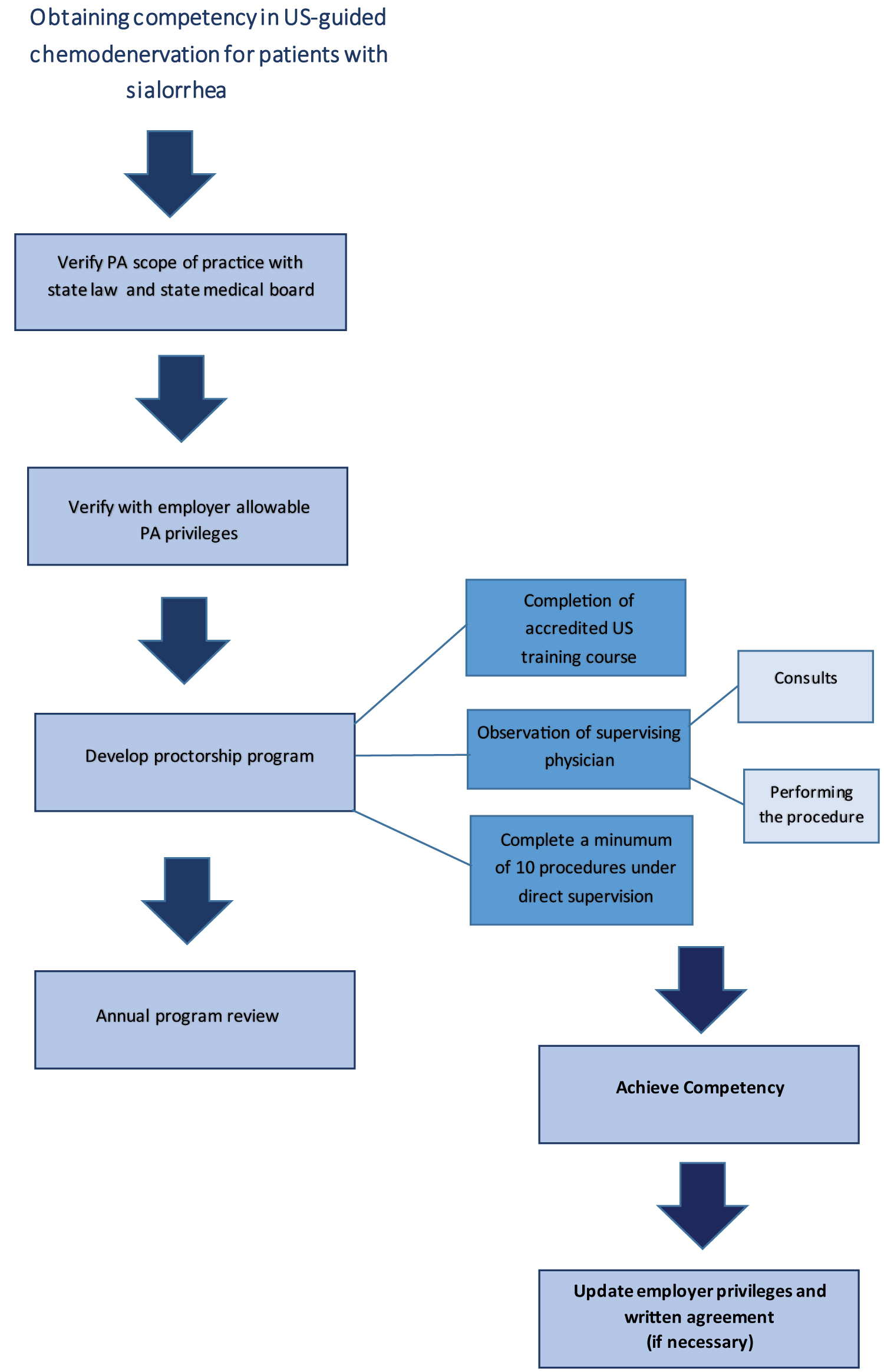 Figure 1: Obtaining physician assistant competency in ultrasound guided chemodenervation for patients with sialorrhea.
Figure 1: Obtaining physician assistant competency in ultrasound guided chemodenervation for patients with sialorrhea.
US: Ultrasound.
View Figure 1
For billing purposes, the Centers for Medicare and Medicaid Services (CMS) maintain a policy that PA services are paid at 85% of what a physician is paid under the Medicare Physician Fee Schedule [9]. Private insurances cover the procedural costs similarly, but some will reimburse 100% for PA services [9]. The PA should maintain billing under his/her National Provider Identifier for the procedures [9]. Under the CMS rules, the physician does not need to evaluate or treat any new or established patient nor does the physician have to be onsite during the procedure when performed by a PA unless required by state law or facility protocols [9]. The supervising physician should be available by a reliable means such as telephone in case immediate consultation is necessary [9]. If the facility or physicians wish to obtain 100% reimbursement for the procedure then guidelines for a shared/split visit or incident to billing must be followed [9]. However, in performing shared/split visits this eliminates the opportunity to utilize the physician in other ways in return for only an additional gain of 15% reimbursement. In our institution we ensure prior to transitioning care to a PA that the patient is educated on the difference of the profession and the patient is agreeable to having a procedure completed by a PA prior to scheduling. The patient always maintains the right to continue seeing the physician for care.
In summary, the PA's role in office-based procedures in Otolaryngology has expanded and can help improve access to care and open physician schedules for consults and follow-ups. Consideration of state and facility protocols is necessary to ensure compliance with regulations. Competency can be achieved with continuing education and a supervised training program while maintaining good patient satisfaction. Although other subspecialties have demonstrated effectiveness and safety with PAs performing in-office procedures, we do recommend further study into effectiveness and safety outcomes of PAs performing in-office procedures in Otolaryngology to further confirm the utilization of PAs is safe and effective compared to surgeons.
None.
Authors report no financial ties or conflict of interest.
None.
Tiffany Heikel: Drafting of the manuscript; Administrative, technical, or material support; Jessyka G. Lighthall: Critical revision of the manuscript for important intellectual; Administrative, technical, or material support.