Foreign body impaction in the head and neck region may result from either a traumatic or an iatrogenic injury. Penetrating neck injuries with impacted foreign bodies are of special concern as the neck contains many vital structures. Hence, early detection and removal of the foreign bodies is imperative to prevent life threatening complications. Here, we report a 50-year-old male patient with a very small sharp metallic foreign body impacted in the soft tissue of the neck. The patient underwent wound exploration under local anaesthesia and the metallic foreign body was removed. We report this case due to its rarity and also to highlight detailed history and clinical examination always needed for better outcome of the patient.
Anterior neck injury, Foreign body, Smallest
A majority of the lacerations cases seen in the emergency department are caused by penetrating sharp metal objects [1]. Sharp foreign bodies when present in the head and neck region pose a challenge, as they may be difficult to locate and remove [2]. Sharp foreign bodies in the neck pose a threat due to the possibility of deeper migration and complications. Metallic foreign bodies can be detected using various modalities like plain radiograpgy, xerography, ultrasonography, computerized tomography and metal detectors [2]. Immediate detection and removal of these foreign bodies, ensures prevention of complications.
A 50-year-old male, welder by profession, presented to the Ear, Nose, throat outpatient department with complaints of constant neck and throat pain for the past 5 days. He gave no history of upper respiratory infection, breathlessness or foreign body ingestion. He had no history of fever or any previous surgeries. Patient was a known case on uncontrolled diabetes mellitus on oral hypoglycaemic drugs.
Clinical examination of the throat, nose and ear were found to be normal. Indirect laryngoscopy was normal. On examination of the neck, a small, firm 0.5 × 0.5 cm swelling was found in the midline of the anterior aspect of the neck (Figure 1), which was not warm, erythematous or tender. On further probing into the patient's history, he revealed that he had sustained an injury 8 days back at his workplace while he was welding metal, when the metal shattered on impact and hit his neck. The patient was taken to a local hospital where he was told that he had sustained a small laceration on his neck, for which dressing was done and oral antibiotics prescribed. Patient continued to have neck pain and consulted various hospitals where he was prescribed medications, but with no relief.
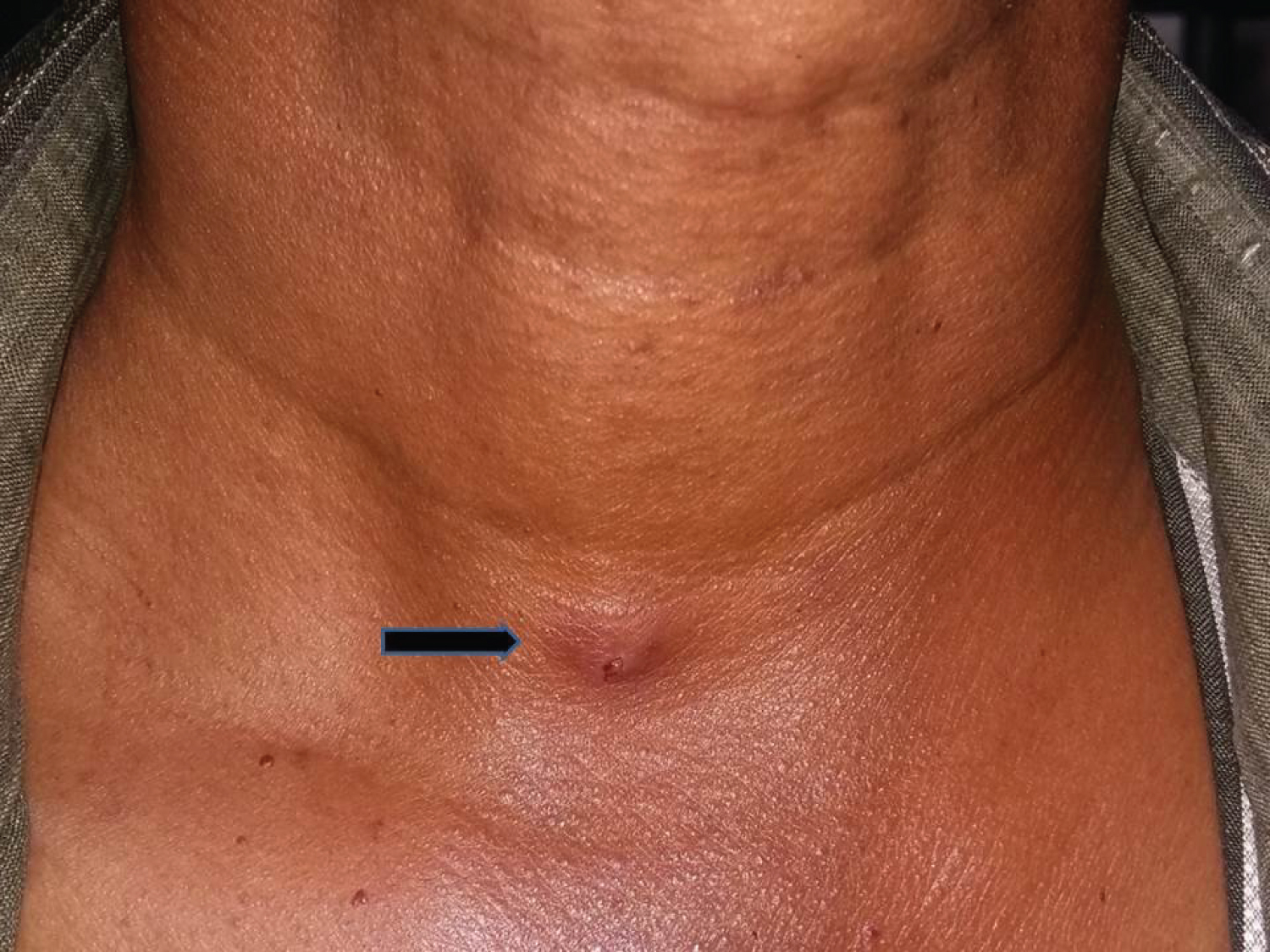 Figure 1: 0.5*0.5 cm swelling in front of the neck.
View Figure 1
Figure 1: 0.5*0.5 cm swelling in front of the neck.
View Figure 1
On investigation with radiograpgh soft tissue neck antero-posterior and lateral view, a radio-opaque foreign body, measuring about 2 mm, was found at the level C6-C7 and 3 mm deep from skin (Figure 2), above the supra-sternal notch. We planned to explore the neck and to remove the foreign body. After the preliminary investigations were done, the patient's wound was explored under local aneasthesia. A horizontal elliptical incision about 3 cm was made around the swelling and subcutaneous tissue was dissected. The superficial fascia and platysma were bluntly dissected and a metal shard, measuring around 2 mm, was visualized and removed (Figure 3). The granuloma which had formed around the foreign body was dissected and removed (Figure 4). The wound was sutured by subcuticular sutures. Post-operative period was uneventful. The post-operative X-ray soft tissue neck antero-posterior and lateral view showed no foreign body.
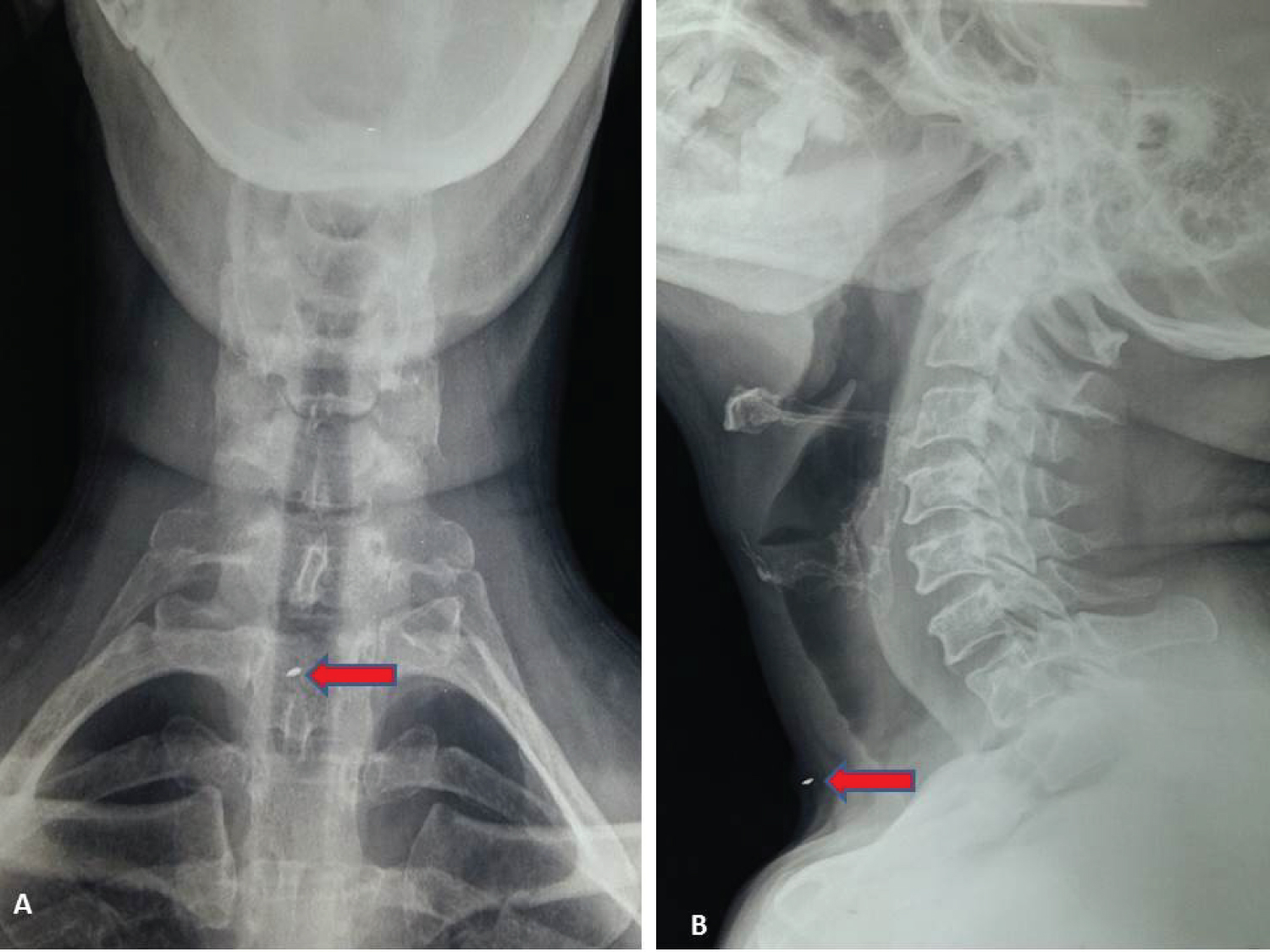 Figure 2: Radigraph Neck (A: AP view, B: Lateral view) showing small radio opaque foreign body.
View Figure 2
Figure 2: Radigraph Neck (A: AP view, B: Lateral view) showing small radio opaque foreign body.
View Figure 2
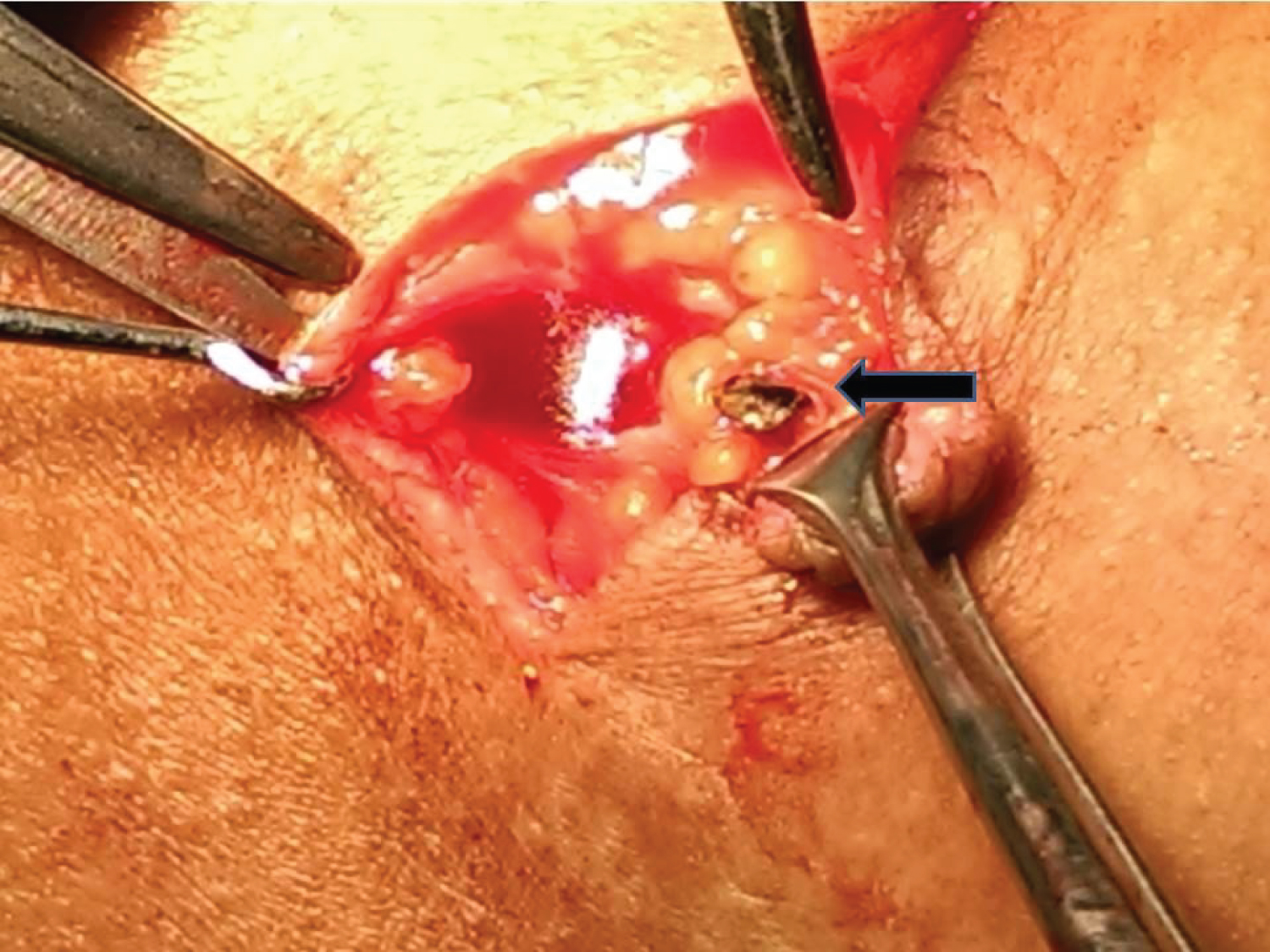 Figure 3: Intraoperative image showing metal foreign body.
View Figure 3
Figure 3: Intraoperative image showing metal foreign body.
View Figure 3
 Figure 4: Metal Foreign body along with granulation tissue is removed.
View Figure 4
Figure 4: Metal Foreign body along with granulation tissue is removed.
View Figure 4
About 5-10% of all trauma cases are penetrating neck injuries [3]. It is imperative to diagnose and treat penetrating neck injuries due to the presence of vital structures which are divided into the following four groups [3]: (i) Airway: Trachea, larynx. Lungs (ii) Vascular structures: The carotid, jugular, innominate and aortic arch vessels (iii) Gastrointestinal structures: Pharynx, oesophagus (iv) Neural structures: Cranial nerves, peripheral nerves, brachial plexus, spinal cord. The impacted foreign bodies can injure any of the above vital structures. Hersman, et al. [4] reported in a retrospective study that the overall mortality rate in penetrating neck injuries is 9%.
Generally, diagnosis of an impacted foreign body following a penetrating neck injury is obvious from the history and clinical examination. However, identification of the foreign body is difficult if the foreign body is small or thin or in patients with multiple injuries of the neck. Precise location of the foreign body needs to be determined to ensure its complication free removal [5]. A detailed clinical examination to assess the wound size and severity should be carried out and vascular injury should always be ruled out. Radiological investigations like plain radiographs and ultrasonography of the neck, can help in detecting radio-opaque foreign bodies and provide an insight to the location and size of the foreign body. CT and MRI scans help in detecting the foreign bodies and their relation to the adjacent structures, which in turn helps to plan the surgical management. MRI scans are very useful in detecting non-metallic foreign bodies [6]. Removal of impacted foreign bodies in the neck follows meticulous surgical exploration of the laceration site. A thorough knowledge of the anatomy of the neck region and recent management protocols are necessary to successfully remove foreign bodies in the neck region [7]. In our case, foreign body size was very small and so led to missed diagnosis initially.
Foreign bodies in the neck due to penetrating injuries are dangerous and life threatening. Early diagnosis and detection by clinical examination and radiography is essential. Immediate removal of the foreign bodies by surgical exploration of the wound can prevent complications.