Here we report on a rare case of a retrochiasmic craniopharyngioma that required a two stage surgical resection to achieve near total resection. The pterional-orbital approach was chosen for initial resection, given the small size of the sinus corridor on imaging, but due to fear of damaging local structures complete resection was not achieved. The patient returned to the operating room 12 days following the first surgery for a combined neurosurgery-otolaryngology approach for endonasal endoscopic transsphenoidal trans tuberculum sella resection of remaining tumor using stereotactic CT guidance. This resulted in near total resection of the mass. This case illustrates the benefits of multistage resection of difficult to access brain tumors. In the case of craniopharyngiomas, the best approach is dictated by location of the tumor in relation to the sella turcica and optic chiasm. In the case of craniopharyngiomas with complex location, as in this case, often more than one surgical approach is required for near total resection while minimizing risks of each individual approach.
Pterioneal-orbital approach, Transsphenoidal approach, Retrochiasmic, Craniopharyngioma
Craniopharyngiomas are rare tumors arising from the sella turcica, with an overall incidence of 0.17 per 100,000 person years, that are thought to originate from epithelial remnants of Rathke's pouch [1]. They are histologically benign tumors that present slowly with symptoms that usuallyinclude nausea, vomiting, or headache from increased intracranial pressure and endocrine and visual disturbance from mass effect against the pituitary and optic chiasm [2]. Most craniopharyngiomas are suprasellar and located anterior to the optic chiasm. Retrochiasmatic tumors lie behind the optic chiasm and can extend into the third ventricle and along the brainstem, posing a unique difficulty in surgical resection. To attempt to achieve total resection with lower complication rate, several different approaches have been developed including pterional-orbital, transsphenoidal, sub-temporal, and trans-petrosal. This case report describes the near total resection of a retrochiasmatic craniopharyngioma by a two staged surgery utilizing a pterional-orbital and transsphenoidal approach.
A 40-year-old male presented with a one month history of peripheral vision loss and excessive urination. He also reported aone year history of headache, low libido, and loss of energy. Neurologic exam was unremarkable, however the presenting brain magnetic resonance imaging (MRI) demonstrated a sellar/suprasellar mass andlabs found abnormal levels of LH, prolactin, and IGF (Figure 1). Maxillofacial CT imaging with contrast demonstrated a partially cystic, solid, and calcified sellar/suprasellar mass suggestive of craniopharyngioma measuring 4.2 AP × 2.9 CC × 3.2 TV extending anteriorly along the planum sphenoidale and posteriorly causing mass effect/posterior displacement of the third ventricle with extension around the right ICA. The pterional-orbital approach was chosen for initial resection, given the small size of the sinus corridor on imaging andthe patient was scheduled for urgent surgery due to vision deterioration.
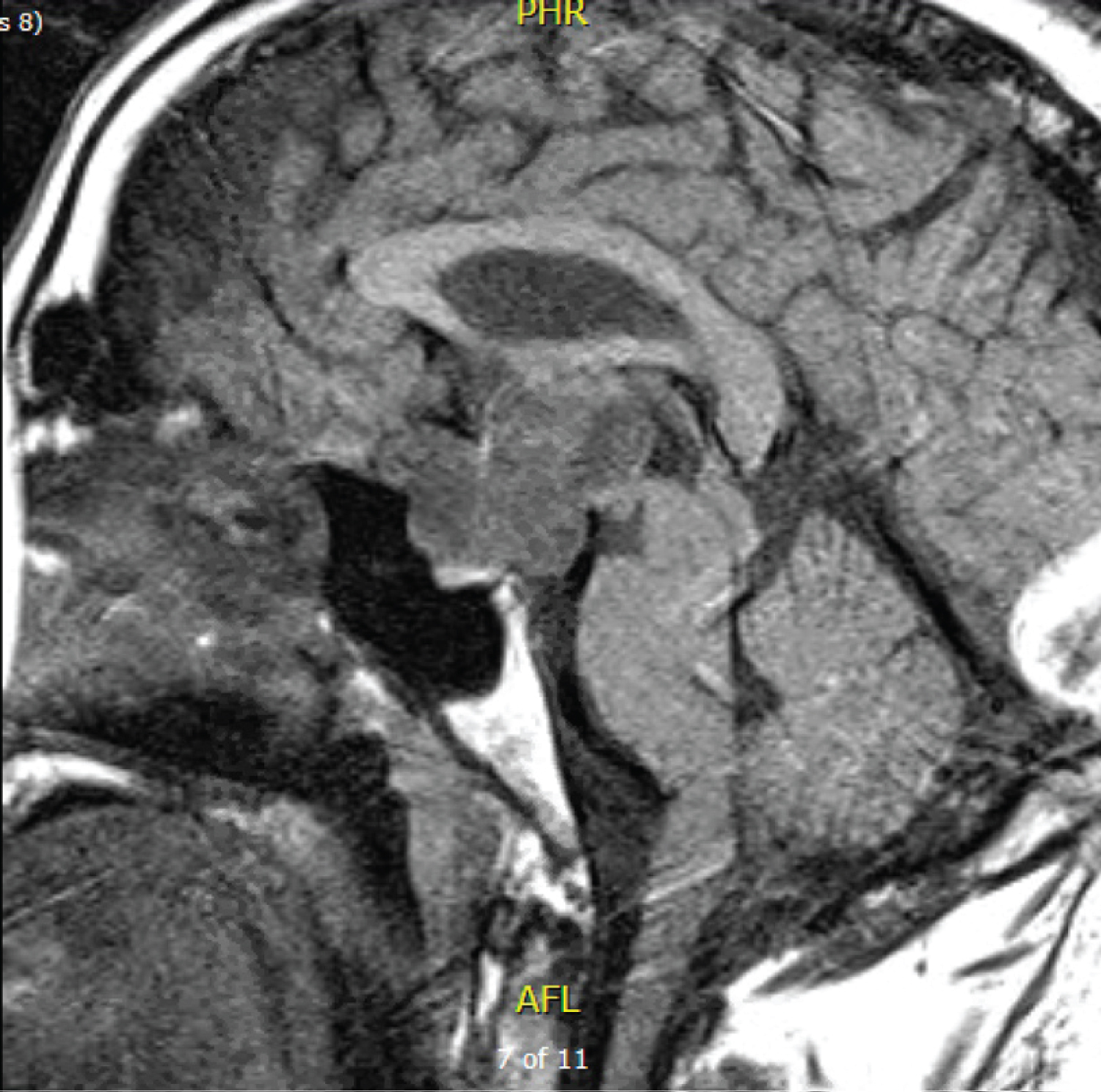 Figure 1: Presurgical MRI demonstrates a partial cystic, solid and calcified suprasellar/sellar enhancing mass.
View Figure 1
Figure 1: Presurgical MRI demonstrates a partial cystic, solid and calcified suprasellar/sellar enhancing mass.
View Figure 1
Evaluation by neurosurgery was preformed and 15 days later, the patient underwent tumor resection via the right pterional-orbital approach with anterior clinoidectomy. The tumor was identified in the capsule in the prechiasmatic space and along the tuberculum sellae and anterior arachnoid dissection was used todissect the tumor off the left optic nerve, left carotid, tuberculum sellae, and pituitary fossa. Anopticocarotid cistern window and oculomotor window were utilized to identify tumor that was lateral to and encasing the carotid artery as well as tumor that was up to the dorsum sella and into the prepontine space. Retraction was used to deliver the tumor into the field until no more tumor could be removed, however part of the tumor remained in the retrochiasmatic space. The anterior cerebral arteries were then identified just above the chiasm with the anterior communicating artery centered on the lamina terminalis, tightly knit with multiple perforators and the lamina terminalis was noted to be consistent with preoperative imaging demonstrating the anterior corpus callosum and the fornix in that tight space. Surgery was not continued to avoid injury to these structures. Post-operative imagining estimated 60-70% tumor removal (Figure 2).
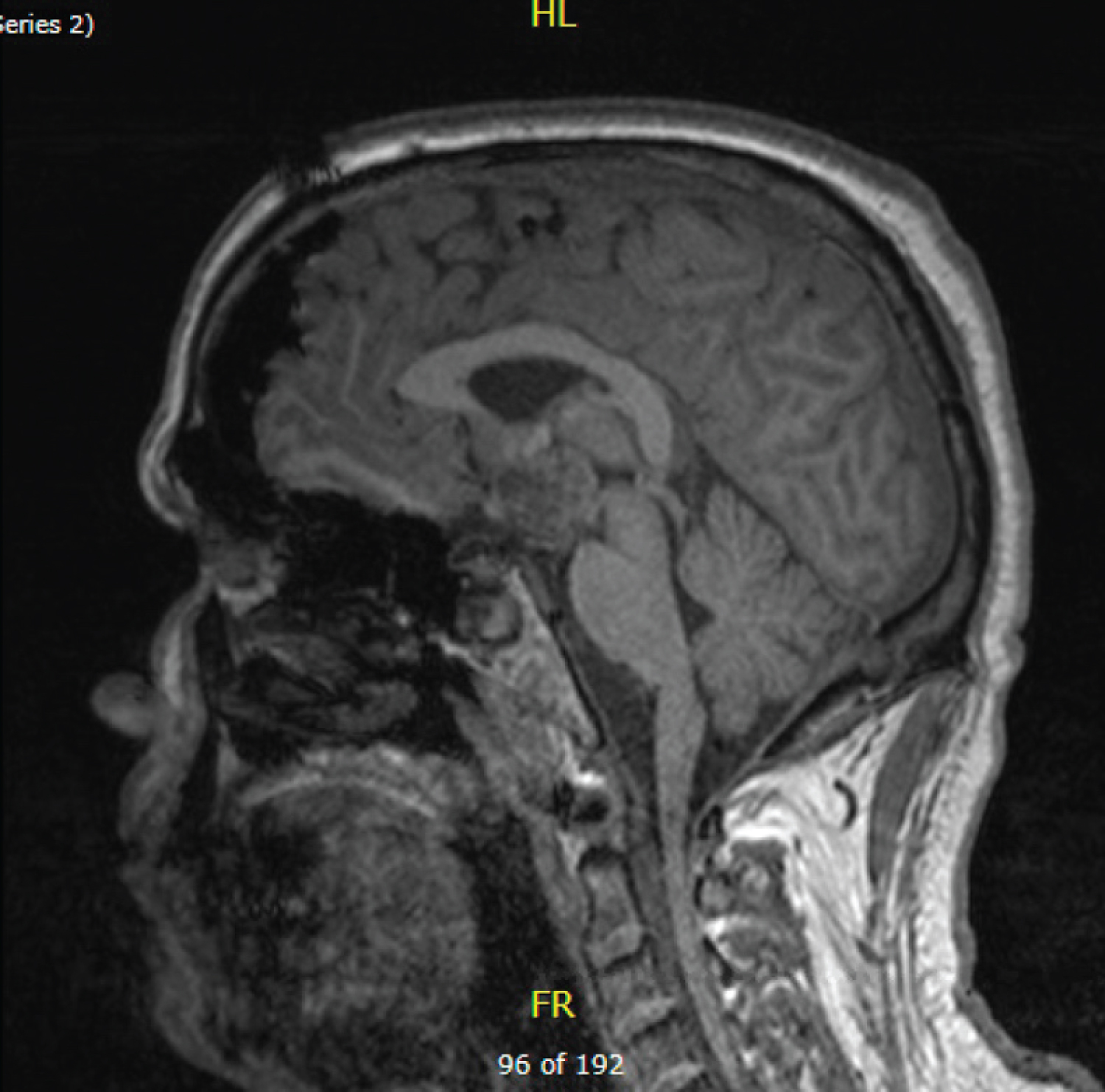 Figure 2: MRI demonstrate postsurgical changes related to right pterional craniotomy for mass resection of a partially calcified sellar/suprasellar mass.
View Figure 2
Figure 2: MRI demonstrate postsurgical changes related to right pterional craniotomy for mass resection of a partially calcified sellar/suprasellar mass.
View Figure 2
The patient returned to the operating room 12 days following the first surgeryfor a combined neurosurgery-otolaryngology approach for endonasal endoscopic transsphenoidal trans tuberculum sella resection of remaining tumor using stereotactic CT guidance. Right sided total ethmoidectomy and sphenoidectomy were performed followed by posterior septectomy on the contralateral side withthe posterior of the bony septum removed. Craniotomy was performed from the clival recess up to the tuberculum sella exposing the carotid arteries. Dural incisions were made horizontally below and above the superior cavernous sinus. Compression of the pituitary gland allowed for a trajectory into the subchiasmatic and retrochiasmatic space. The tumor was then dissected off the walls of the hypothalamus and retrochiasmatic region. Tumor was debulked until the approach was within the 3rd ventricle. The right lateral portion of the tumor was completely dissected off the glial wall of the hypothalamus and the left lateral wall of the floor of the hypothalamus was dissected off to the area just above the left posterior communicating artery and the inferior lateral wall of the hypothalamus. Nearly 95% of tumor in this region was removed. The area was irrigated and the approach was closed using dura pair autograft and nasoseptal flap.
Postoperative imaging demonstrated near total resection of the mass (Figure 3). Following surgery, the patient developed panhypopituitarism and was reliant on hormone replacement.
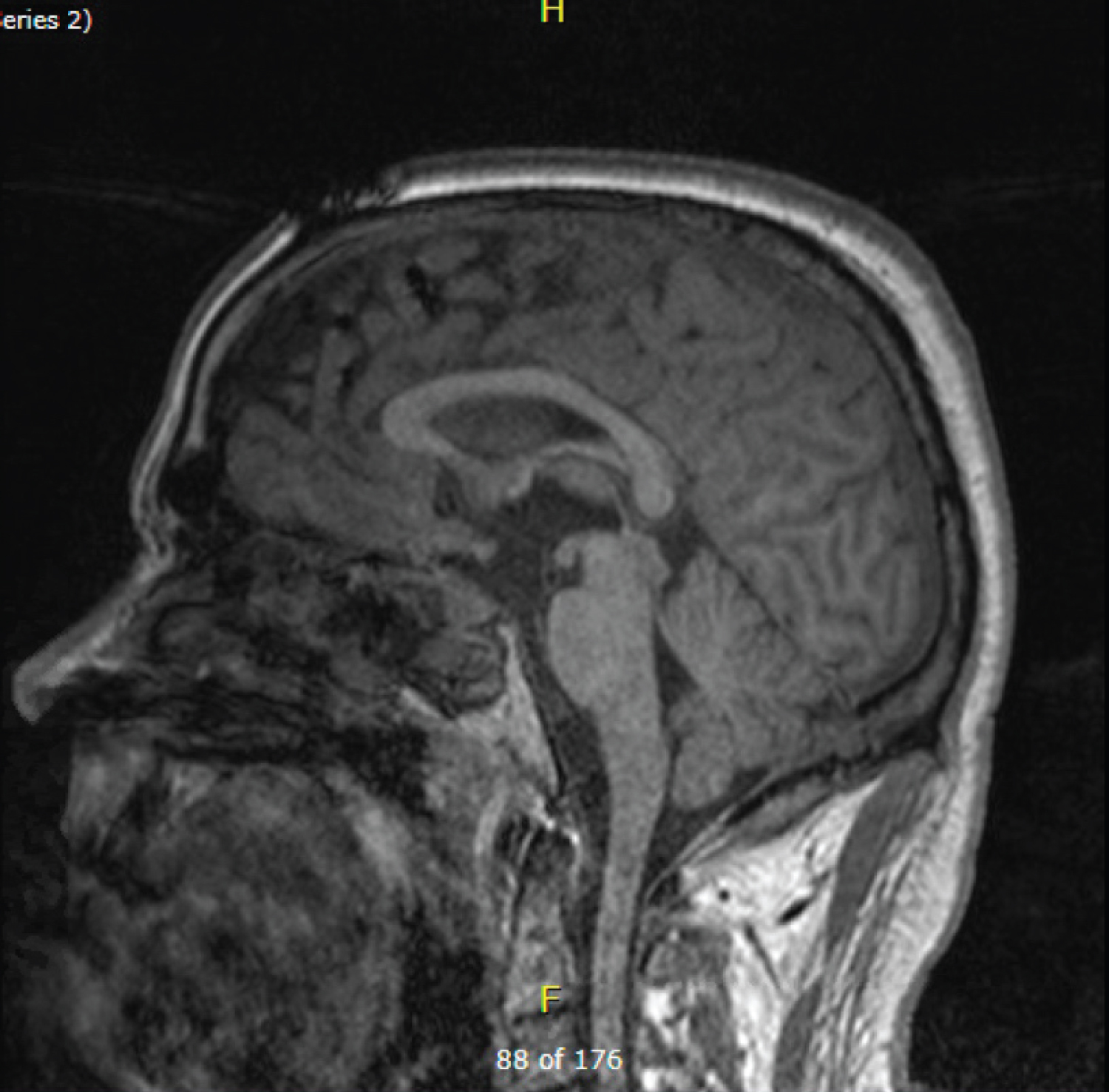 Figure 3: MRI demonstrates post-surgical changes related to right pterional craniotomy and transsphenoidal resection of a craniopharyngioma.
View Figure 3
Figure 3: MRI demonstrates post-surgical changes related to right pterional craniotomy and transsphenoidal resection of a craniopharyngioma.
View Figure 3
The retrochiasmatic region is one of the most difficult areas to approach surgically, which has led to a much higher reoccurrence rate as compared to craniopharyngiomas in other locations as well as increased surgical morbidity and mortality [3].
In the case presented, the pterioneal approach was initially chosen due to the small size of the sinus corridor seen on preoperative imaging. This approachallows for large exposure range, clear vision of the midbrain andaccess to the posterior chiasmatic space through the lamina terminalis [4]. Limitations of this approach include that once the lamina terminalis is entered, this approach is limited by the oblique look at the optic chiasm with lack of visualization of the ipsilateral wall of the third ventricle and hypothalamus. During the surgery, the anterior communicating artery was noted to be flush against the lamina terminals with many perforators, leading the surgeon to deem the risk of hemorrhage with entrance of the lamina terminalis too high and the surgery was ended. A transsphenoidal approach was then selected to complete resection.
Though the transsphenoidal approach traditionally was used for tumors located within the sella turcica, with the advent of endoscopic technique, this approach has been broadened to include lesions outside of the sella turcica. Via removal of the tuberculum selae and planum sphenoidale allows for direct dissection of tumor from the optic chiasm, third ventricle, hypothalamus, and pituitary stalk [3]. This approach has been shown to have equal or better degree of resection than transcranial routes, however it has been linked to higher rates of post-operative pituitary dysfunction and CSF leak. Other limitations of this technique are a non-pneumatized sphenoid sinus, as this causes absence of typical landmarks. Depending on the location of the tumor, total resection can also be limited. Studies have demonstrated a gross total resection rate of suprasellar craniopharyngiomas from 62.5% to 72% with CSF leak rate of 8.8% to 19% [5,6]. However, after the approach in initial surgery was unamenable to resection of the retrochiasmatic portion of the tumor, despite the small sinus corridor, the transsphenoidal approach was indicated due to superior visualization of the optic chiasm and 3rd ventricle. Ultimately this approach led to the resection of the majority of the tumor.
This case illustrates the benefits of multistage resection of difficult to access brain tumors. In the case of craniopharyngiomas, the best approach is dictated by location of the tumor in relation to the sella turcica and optic chiasm. In the case of craniopharyngiomas with complex location, as in this case, often more than one surgical approach is required for near total resection while minimizing risks of each individual approach. This must be weighed by the risk of undergoing surgery twice with two different access points to the chiasmatic region.
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
None.