Introduction: The spread of SARS-CoV-2 has triggered discussions on various forms of presentation of the COVID-19 and its possible sequelae. In particular, manifestations, including olfactory dysfunctions and neuropsychiatric manifestations, such as sleep disorders and anxiety.
Objective: Characterize the main forms of clinical presentation and possible otorhinolaryngological and neuropsychic sequelae in patients with olfactory disorders in mild flu syndromes during the SARS-CoV-2 pandemic, in Manaus, Amazonas state, Brazil. Method: Descriptive, qualitative-quantitative, observational study of 205 participants with mild flu-like symptoms and conditions secondary to COVID-19.
Results: A total of 185 participants were assessed. Myalgia, fever, and cough were the main reported flu-like symptoms. Of these symptoms, anosmia was identified as the main olfactory dysfunction and was concomitant with the flu condition in the majority of patients. The average number of days with anosmia was higher than the other olfactory disorders; among neuropsychiatric symptoms, patients in contact with the virus evolved unfavorably with severe sleep difficulty and anxiety and headache was a repeatedly associated symptom.
Conclusion: In mild flu syndrome secondary to COVID-19, olfactory dysfunction was mostly sudden, and anosmia was the most prevalent dysfunction, which evolved with a higher average of days when compared to other olfactory dysfunctions. The use of oral or topical medications did not interfere in the evolution of the disease, and patients with olfactory dysfunction presented more structural and inflammatory nasal changes as compared to normal mild flu syndrome. Additionally, an important impact on sleep quality in patients with a positive COVID-19 serological test was observed.
Coronavirus infections, Smell disorders, Sleep disorders, Mental health
The spread of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), with the unprecedented initial report in China in December 2019 and subsequent worldwide dissemination in a few months, has brought to light several forms of presentation of coronavirus disease 2019 (COVID-19), including pulmonary, otolaryngological, neurological and social and mental health-related symptoms. On March 11, 2020, the World Health Organization (WHO) confirmed the COVID-19 global pandemic [1]. In Brazil, the first case was reported in February 2020 in the city of Sao Paulo [2], and up until the beginning of July 2021, the country has recorded more than 18 million confirmed cases and approximately 518.000 deaths [3]. In addition, the state of Amazonas has reported an alarming number of infected patients, with the identification of a new variant, VOC P.1 [4].
Although multiple organ dysfunction syndrome, which is triggered by the involvement of severe acute respiratory syndrome (SARS), is a cause for public health concern, most COVID-19 patients develop the mild form, which does not present an inherent risk to life, but may culminate in sequelae requiring multi-professional support.
Specifically, the main symptoms caused by the SARS-CoV-2 virus include fever, dry cough, and dyspnea [5,6] in the initial phase. On the other hand, in later stages, it is common to have persistence of clinical symptoms, such as fatigue, headache, joint pain, and olfactory disorders, which may be present in 80% of COVID-19 patients [7].
Given this context, secondary syndromes related to SARS-CoV-2 are also present in non-severe patients [8]. In fact, a previous study has reported the existence of “post-COVID” manifestations [7], including olfactory dysfunction and neuropsychiatric manifestations such as sleep disorders and anxiety [9].
Therefore, this study aimed to characterize the main forms of clinical presentation and possible otorhinolaryngological and neuropsychic sequelae in patients with olfactory disorders in mild flu syndromes, during the SARS-CoV-2 pandemic in the state of Amazonas, from July to November 2020.
Data were analyzed on the clinical epidemiological presentation, the main symptoms related to COVID19, the development and evolution of olfactory dysfunction, types of olfactory dysfunction, length of symptom presentation, use of medications, associated symptoms, the relationship between the olfactory dysfunction and neuropsychic pictures and the endoscopic otorhinolaryngologic findings.
This was a descriptive, qualitative-quantitative, observational study, which was based on the description of mild flu-like syndrome patients and their respective main symptoms in the city of Manaus, Amazonas, Brazil, from June to December, 2020.
The participants included in the study were those who were out of the transmission period, over 18 years of age, and who presented with a complaint of sudden olfactory dysfunction during the pandemic. In contrast, patients with neurodegenerative diseases, known chronic nasal disease, previous olfactory dysfunction, bronchial asthma, pneumonia or eosinophilic rhinosinusitis, and those requiring oxygen therapy during the disease period were all excluded from this study.
Data collection was done through a recall questionnaire followed by a subjective olfactory examination at the Otorhinolaryngology Service at The Foundation Hospital Adriano Jorge and included a visual analog scale evaluation using an adapted classification, which was as follows: 0-3 as mild, 3-6 as moderate, and > 6 as severe [10]. Additionally, sleep quality was evaluated using the Mini-Sleep Questionnaire (MSQ), which was adapted to the Brazilian version by Falavigna, et al. [11]. The MSQ is a 70-point questionnaire consisting of 10 questions that address main sleep complaints, such as insomnia, excessive sleepiness (ES), snoring, use of sleeping medications, and sleep fragmentation. For analysis purposes, a score of 10-24 was considered as good quality of sleep, 25-27 as mild sleep difficulty, 28-30 as moderate sleep difficulty, and a score above 30 points was considered as severe sleep difficulty [12]. In addition, the Epworth Sleepiness Scale (ESS) was used to assess drowsiness. This scale is composed of eight items that assess drowsiness in everyday situations, in which a score that is equal to or greater than 11 was considered indicative of excessive sleepiness (ESS) [13]. Furthermore, the intensity of anxiety was subjectively assessed using the Beck Anxiety Inventory (BAI), which is a 63-point questionnaire consisting of 21 questions. For analysis purposes, a score of 0-7 was considered to be a minimum degree of anxiety, 8-15 to be a mild degree, 16-25 to be a moderate degree, and a score of 26-63 was considered to be a severe degree of anxiety [14].
Patients were then objectively assessed by the team using the alcohol test, which was adapted from Davidson and Murphy in 1997. This was performed with a cotton swab soaked in 70% isopropyl alcohol at an initial distance of 30 cm, wherein the material was brought towards the patient's nostrils until it was recognized by the patient. The olfactory threshold was classified according to the recognition distance, for which a distance of 30-20 cm was considered as normal, 19-10 cm as hyposmia, and a distance of less than 10 cm was considered as anosmia [15]. For qualitative testing, four different essences were presented, which is an adaptation of the Quick Smell Identification Test (Q-SIT) proposed by Doty and Jackman in 2005 [16]. Specifically, four different essences (cinnamon, mint, citrus and granulated soluble coffee) were presented, in which each aroma was isolated in a disposable bottle with a lid. The patient was then asked to keep their eyes closed and the bottle was brought to approximately 5 cm from the patient's nostrils. Afterwards, the patient was instructed to smell the essence for 30 seconds, and the test was evaluated based on the number of correct answers. Recognition of two out of three essences was classified as normosmia, one out of three essences as hyposmia, and if none of the essence were recognized, the patient was considered as having anosmia. In addition, the patients underwent a complete otolaryngological clinical examination, including nasal video endoscopy with a 4-mm diameter nasal endoscopy, 0° angulation, and a video system using the GOPRO® HERO 7 PRO HD camera for imaging capture for the database.
Of the 205 initially recruited participants, only 185 completed the study. Among the study participants with mild acute influenza syndrome and olfactory dysfunction, 119 (64.3%) were confirmed to have a SARS-CoV-2 infection (both RT-PCR and serological tests were considered). The COVID-19 test result was positive in 92 (77.3%) patients who underwent the test for confirmation, as shown in Table 1.
Table 1: Clinical presentation of participants. View Table 1
The three main initial symptoms reported for COVID-19 were myalgia (88.8%), fever (79.2%) and cough (74%), and each individual presented with more than one symptom. Of the three, myalgia was the most prevalent symptom on initial presentation, including among the patients with a positive virological test (Table 2).
Table 2: Other presenting otorhinolaryngological symptoms among participants. View Table 2
On average, patients was 7.2 days (range: 0-158 days) onset to olfactory dysfunction. In those with olfactory dysfunction, the mean time of the clinical persistence was reported to be 29.6 days (range: 0-152 days) (Table 1). The appearance of olfactory symptoms was concomitant with the general clinical (fever, myalgia, headache) picture in 58.7% of the participants. An improvement in olfactory dysfunction symptoms until the date of interview was described in 86.8% of the participants. Initially, this olfactory disorder was classified as anosmia, hyposmia, phantosmia, dysosmia and cacosmia. Among them, anosmia was the most prevalent, and was described by 135 (81.8%) of the participants (Figure 1). When associated with another olfactory disorder, there was a predominance of anosmia and cacosmia, as cited by 18 (10.9%) of the participants.
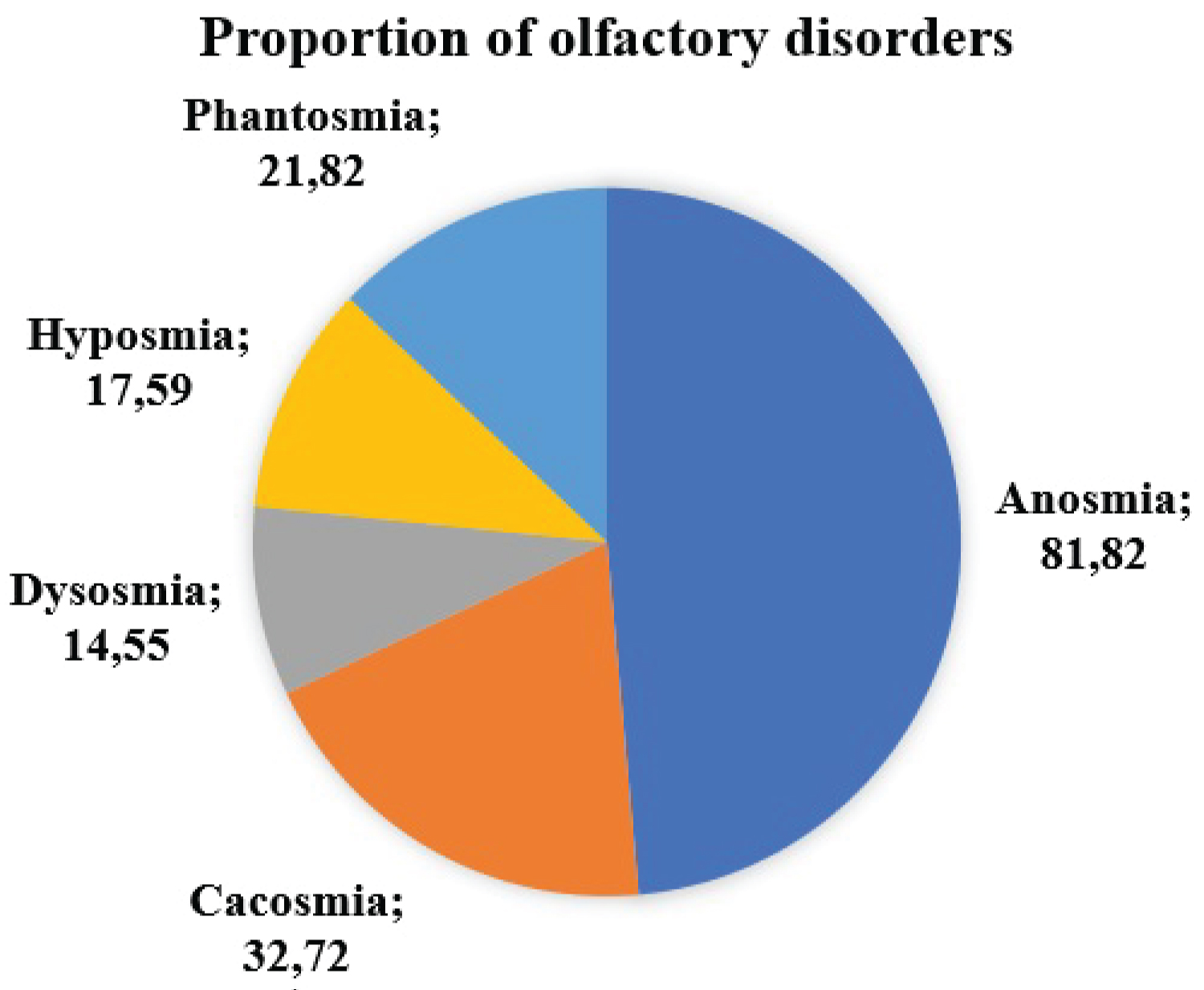 Figure 1: Classification of olfactory disorders.
View Figure 1
Figure 1: Classification of olfactory disorders.
View Figure 1
Although there was a significant positive association between the alcohol test and Q-SIT (χ2 = 11.5, p-value = 0.02), the mean number of days with anosmia for the alcohol test results showed no significant difference (χ2 = 5.8, p-value = 0.05) (Figure 2). However, there was a significant difference between the mean number of days with anosmia for the Q-SIT results (χ2 = 9.6, p-value = 0.008) (Figure 3). Furthermore, the mean number of days with olfactory dysfunction was significantly higher for patients with anosmia (p-value = 0.04).
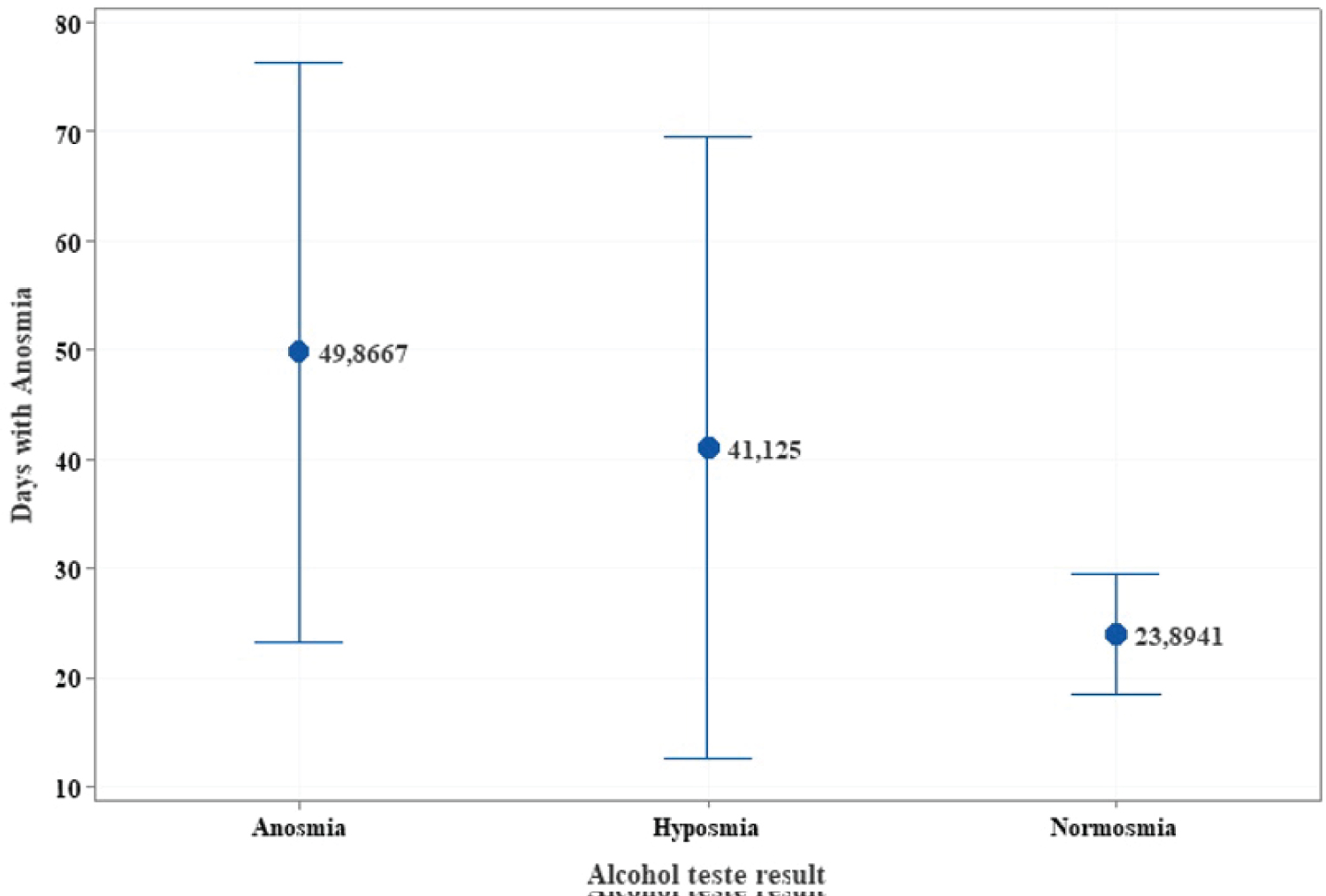 Figure 2: Confidence interval for mean days with anosmia based on the alcohol test result.
View Figure 2
Figure 2: Confidence interval for mean days with anosmia based on the alcohol test result.
View Figure 2
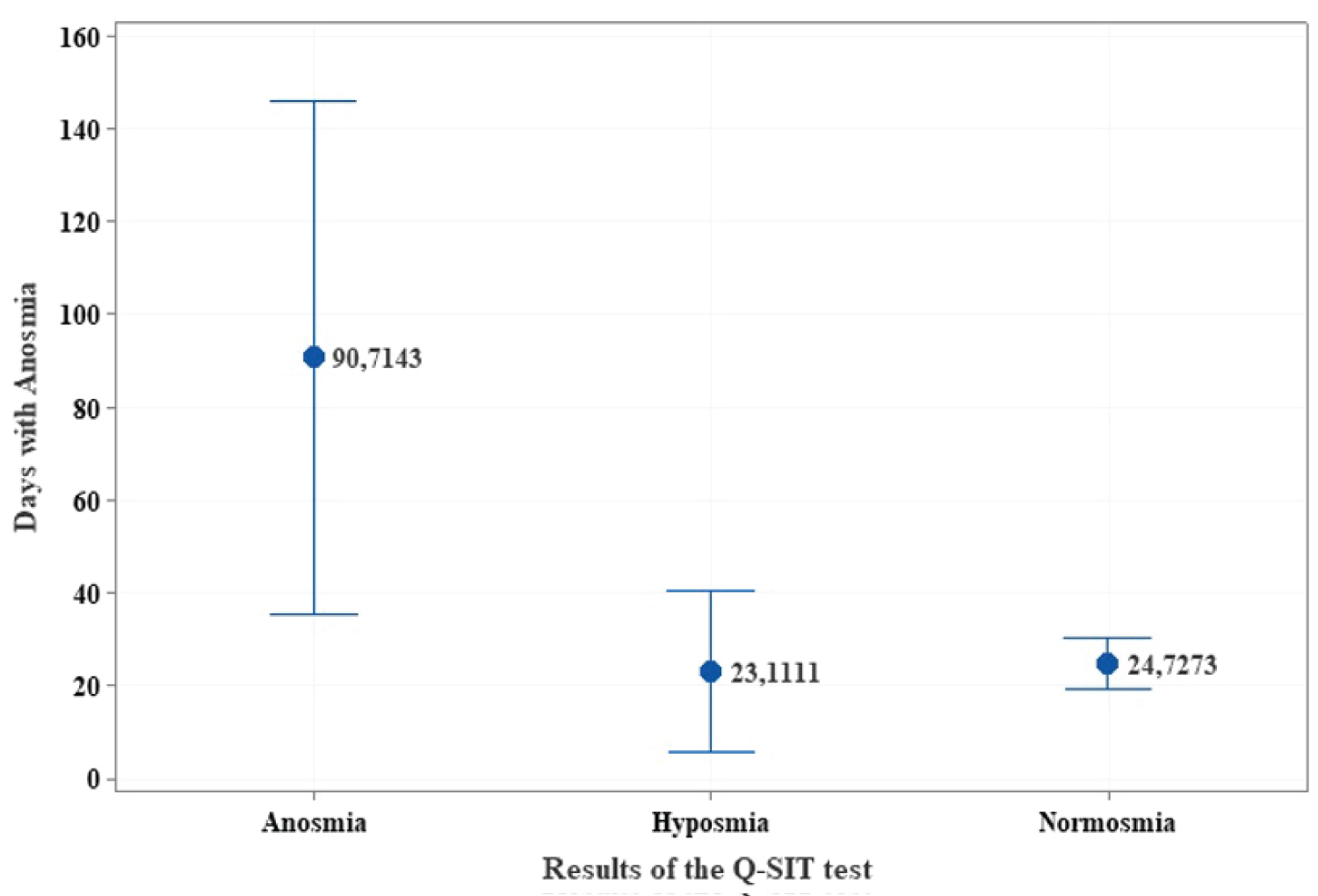 Figure 3: Confidence intervals for the average days with anosmia based on the Q-SIT test.
View Figure 3
Figure 3: Confidence intervals for the average days with anosmia based on the Q-SIT test.
View Figure 3
The most common oral medications for general symptoms among the included patients were reported to be azithromycin (50.9%) and ivermectin (31%), while the most common symptomatic medication was dipyrone (or similar), which was used by 49 (28.6%) patients. The use of non-pharmacological medications was also reported, with garlic and lemon being the most prevalent (45.6%). Additionally, the most cited topical treatments for olfactory dysfunction were nasal corticosteroids, naphazoline, Vick Vaporub®, and saline 0.9%.
Notably, some participants presented symptoms associated with olfactory dysfunction, with taste alteration (ageusia) in 109 (59.2%) of the 184 patients. Moreover, another 49 patients reported hypogeusia, and 14% of the sample stated that they did not develop alterations in taste.
Regarding the olfactory assessment in the laboratory-confirmed sample for SARS-CoV-2 infection, these patients were predominantly characterized as having normal sensitivity to olfactory stimulation in 77.6% of patients for the objective test and 76.6% of patients for qualitative test (Table 3).
Table 3: Objective and qualitative classification of olfactory dysfunction among COVID-19-positive and negative participants. View Table 3
No significant difference was detected between patients who tested negative or positive for COVID-19 with regard to categories of sleep and anxiety. However, there was a noted high frequency of patients with severe sleep difficulty and anxiety (Table 4). Change in sleep quality as assessed by the MSQ indicated that 77.4% of those with a positive viral infection test described severe sleep difficulty; though this was described in only 22.6% of those with a negative test, and no statistical significance was determined. Similarly, the BAI revealed that severe anxiety was described by 76.6% of the patients with a positive viral infection test and only 23.4% of those with a negative test, also showing no statistical significance (Table 4).
Table 4: Changes in quality of life, excessive sleepiness, and anxiety among COVID-19-positive and negative participants. View Table 4
Correlation analyses also found that the variables MSQ, ESS, and BAI presented a positive and significant correlation (Figure 4).
 Figure 4: Pearson's correlation between the variables of Mini-Sleep Questionnaire (MSQ), Beck Anxiety Inventory (BAI), and Epworth Sleepiness Scale (ESS).
View Figure 4
Figure 4: Pearson's correlation between the variables of Mini-Sleep Questionnaire (MSQ), Beck Anxiety Inventory (BAI), and Epworth Sleepiness Scale (ESS).
View Figure 4
As for endoscopic findings, the presence of signs suggestive of rhinopathy were present in 41 patients, of which a total of 30 (73.2%) were positive for SARS-Cov-2 (Figure 5).
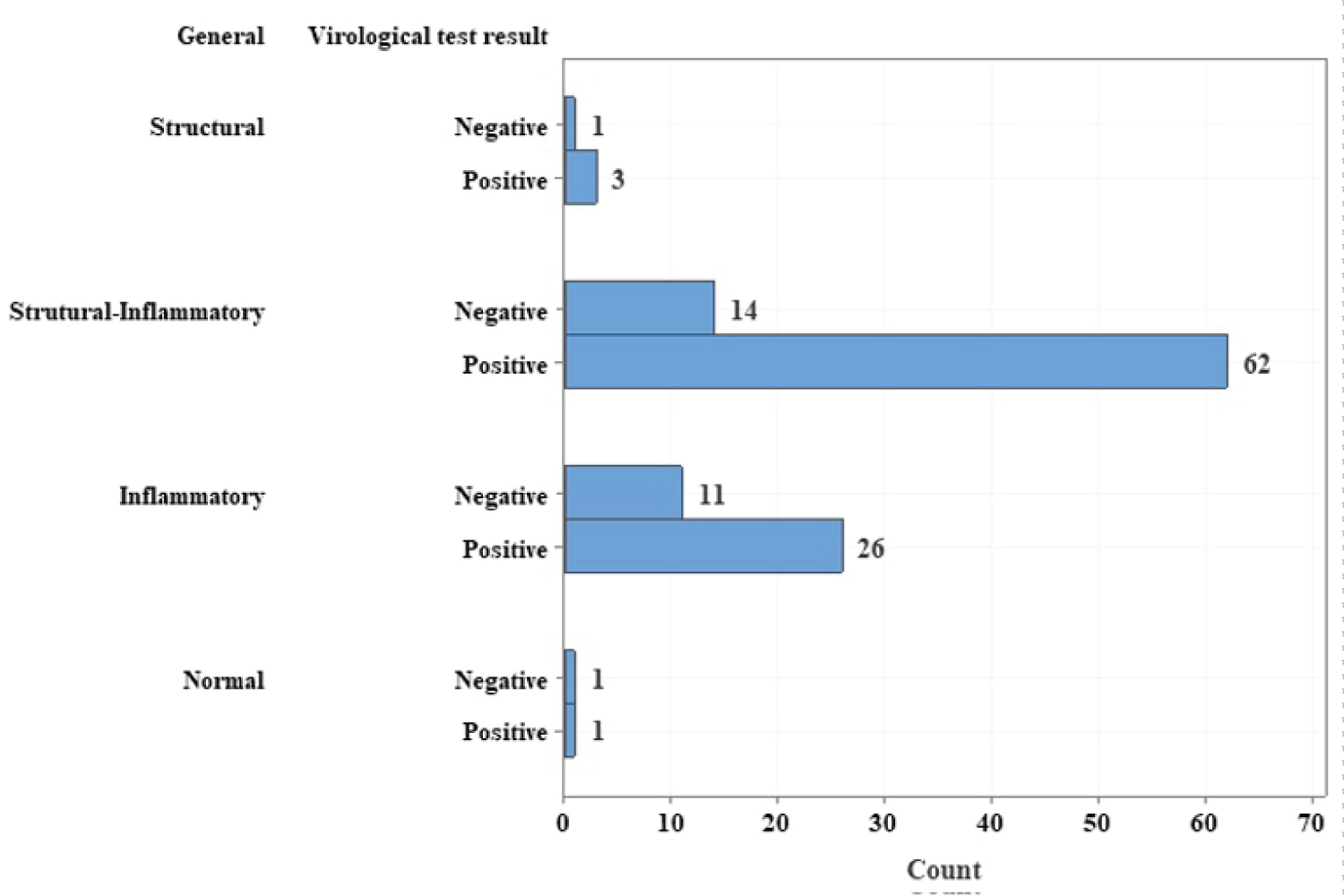 Figure 5: Nasal endoscopic evaluation findings.
View Figure 5
Figure 5: Nasal endoscopic evaluation findings.
View Figure 5
This study reported the prevalence and clinical characteristics of mild acute respiratory syndrome patients, with greater attention focused on severe conditions during the COVID-19 pandemic in a specialized otorhinolaryngology service in the capital of the Amazonas state. During the study, improvement in olfactory dysfunction caused by SARS-CoV-2, the changes caused by its diagnosis, the quality of sleep among patients, and their subjective level of anxiety were followed, without the aim of monitoring them.
The study showed that the proportion of women with mild respiratory syndrome and olfactory dysfunction at some point in the course of the disease was significantly higher than that of men. This was also reported by Kosugi, et al. (2020) in the evaluation of sudden olfactory dysfunction in Brazil during the pandemic, wherein olfactory dysfunction was present in approximately 60% of the women evaluated [17]. This result may be motivated by the fact that women seek more medical care at the initial presentation of symptoms, or perhaps women may actually have some protective factor in relation to COVID-19 severity, since this study only selected patients with mild cases.
The mean age of the participants in this study was 42.5 years (18-90 years), which was consistent with data released in a report by the Center for Disease Control and Prevention (CDC) in June 2020, stating that COVID-19 leads to severe outcomes in older patients with underlying health problems [18]. Therefore, the age of patients with mild symptoms is expected to be lower.
Of the 185 participants who completed the assessment, 119 had a confirmatory laboratory test for COVID-19; however, this may be related to the fact that other flu-like syndromes may have been the cause of general symptoms and olfactory dysfunction. Despite this, it is worth mentioning that at the time of evaluation, access to serological diagnosis or RT-PCR was restricted only to severe cases, and as the population of this study was based on mild cases, this would not be evident. Moreover, according to a report published by the Oswaldo Cruz Foundation (FIOCRUZ) in November 2020, there was a substantial decrease in the involvement of other respiratory viruses in cases of SARS in the main Brazilian capitals, whereas SARS-CoV-2 was reported to be responsible for 97.7% of the confirmed laboratory results [19].
Regarding the initial symptoms among the patients, the most common were myalgia, fever, and cough. An important Chinese study on patients presenting mild symptoms, published at the beginning of the pandemic, reported that the main symptom was nasal congestion (61.5%), which was followed by cough (46.3%), while myalgia and headache were present in only 23% of the included patients [5]. This same study also cited headache as one of the most prevalent manifestations among individuals [5]. Similarly, in the present study, we also observed that headache was one of the most frequent complaints among COVID-19 patients (61%) as compared to those without viral infection (p = 0.04). In a previous study conducted in Brazil, Rocha-Filho and Magalhaes (2020) also reported that headache occurred in more than 60% of patients infected with SARS-CoV-2 [20].
The development of olfactory dysfunction in this sample from the general symptom onset to the perception of olfactory dysfunction varied widely (0-158 days); however, 58.7% mentioned that the appearance of olfactory symptoms occurred concomitantly and abruptly with the general clinical picture, with none of the participants reporting that olfactory dysfunction appeared before the general symptoms. In contrast to our findings, a previous study by Lechien, et al. reported that 11.8% of their sample had olfactory dysfunction prior to the onset of general or other otorhinolaryngological symptoms [21].
In the subjective evaluation of olfactory disorder diagnosis, anosmia, although more prevalent, may have been overestimated when compared to the other characteristics, possibly relating to some degree of bias. To some degree, this would explain the disagreement between the objective and subjective tests, since some patients reported dysfunction, but also had a normal objective test result. These data are in agreement with two previous studies described by Kosugi, et al. [17] and Hopkins, et al. [22], in which 76.9% and 83.4%, respectively, of olfactory dysfunction cases related to COVID-19 were reported to be anosmia. In the present study, among participants who had concomitant olfactory dysfunctions, the most commonly reported was anosmia with cacosmia, which was cited by 18 (10.9%) patients. However, these data should be analyzed with caution since the different types of symptoms may have arisen in different stages of the disease.
The mean time of the clinical presentation of olfactory dysfunction was reported to be 29.6 days (0-152 days), with complete or partial recovery of symptoms. One study published in June 2020 showed that the average recovery in COVID-19 patients with olfactory dysfunction was 15 days (4-27 days) after the onset of symptoms [23], and one of the pioneering studies of this subject reported that in their sample, 72.6% of the patients recovered olfactory function in the first 8 days after disease resolution (absence of general and otorhinolaryngological symptoms) [21].
Olfactory dysfunction improvement was described in 87% of the sample until the date of interview, with an average of 29.6 days to improvement. Given that this study included patients outside the viral transmission period (after the 14th day of symptom onset) and those with milder symptomatology, this result was expected, since a minority of patients evolve with maintenance of symptoms for longer periods [21]. Moreover, Kosugi, et al. (2020) described that sudden olfactory dysfunction had different forms of presentation among patients. Among those who fully recovered, participants with positive tests took an average of 5 days longer to regain their sense of smell as compared to patients with negative or unknown tests. Additionally, patients with a positive test had less total recovery and longer time of symptomatic evolution [17].
Regarding medication use, much has been discussed recently about the use of medications in the course of COVID-19. Currently, the use of preventive medications is not recommended. Given that the participants of this study had the disease at the beginning of the pandemic, this was a very controversial issue, which may have influenced the use of medications that are currently no longer recommended in mild cases. Particularly, this sample showed large adherence to azithromycin (50.9%) and ivermectin (31%) use by the interviewees, and dipyrone (or similar) was also reported by 28.6% of patients. In the study presented by Lechien, et al. in 2020, paracetamol (62.4%) was found to be the most prevalent medication, whereas the use of oral corticosteroids concomitantly with antibiotics was cited in 1.4% of the sample [21]. Thus, there were no significant differences in the mean number of days between the onset of flu-like symptoms and olfactory dysfunction or days with anosmia between patients who took or did not take medications (e.g., azithromycin, chloroquine or hydroxychloroquine, ivermectin).
Notably, there is a significant influence of traditional indigenous medicine as basic health care in the region where the study was carried out, making it one of the main reasons for the use of non-pharmacological medications in the present study's sample. The most prevalent non-pharmacological treatment was the use of garlic with lemon by 45.6% of patients. In addition to this being a traditional practice, another important factor that could be related to the abundant use of medicinal plants is the fact that they cause fewer side effects as compared to pharmacological drugs. In particular, an elaborate study published in March 2021 reviewed the importance and broad presentation of medicinal plants used in the viral infection treatments, as well as the antiviral properties of their phytochemicals. However, the study stated that further in vitro and in vivo studies are necessary to assess anti-SARS-CoV-2 specificities of these plants [24].
Furthermore, regarding the use of medications, this sample group was also questioned on the use of topical therapies for olfactory dysfunction, and among the most cited medications were nasal corticosteroids, naphazoline, Vick Vaporub®, and saline 0.9%. In this same context, Lechien, et al. (2020) also reported that nasal irrigation with saline solution and nasal corticosteroid was the most commonly used among patients [21]. However, despite use of at least one of these drugs, none of them had an impact on anosmia improvement, given that there were no significant difference in the mean number of days between symptom onset and olfactory dysfunction, or in the total number of days with olfactory dysfunction between patients who used nasal drugs and patients who did not. This result was similar to the findings of Kosugi, et al. (2020), which state that there was no difference in olfactory dysfunction recovery in correlation with different types of treatments used [17].
Other otorhinolaryngological symptoms were also reported by the included patients, particularly nasal obstruction and rhinorrhea. Similar results were found by Kosugi, et al. who describe nasal symptoms associated with olfactory dysfunction in approximately 44% of patients [17]. There was also a predominance of taste alteration in the dominant part of the our study sample, which was represented by 85% and was described as a total loss of taste sensitivity. However, this symptom was not objectively or qualitatively addressed in the study, which may have generated a bias in the results. Nevertheless, the data corresponded to the previously published outcomes of up to 90% of COVID-19 patients presenting a correlation between olfactory and gustatory dysfunction [22].
Certainly, the most robust result of this study is the change in the quality of life of participants during exposure to symptomatology, as well as the variable stages of disease progression. Approximately 55% of the patients with a positive serological test for SARS-CoV-2 reported severe/high day-to-day impairment due to olfactory dysfunction, whereas 48% of those with negative SARS-CoV-2 results reported the same degree of experience. There was not much discrepancy in the total percentage since, regardless of the serological test results, all participants were exposed to an unprecedented experience in the pandemic. As such, for the purposes of intervention, the experience reported by the patient has greater weight than the serological test result, and this can be taken into account when evaluating the impact of mental health status and care for guidance and interventions during the pandemic. Furthermore, it is possible that cases without serology were in fact untested or underestimated cases.
Interestingly, complaints regarding quality of sleep were also frequent symptoms among COVID-19 patients. This may be related to the fact that their experiences in the pandemic resulted to persistent feelings of uncertainties with daily exposures to stress, anxiety, and depression, especially in the city of Manaus, a capital city that was greatly affected by the first and second waves of cases.
Sleep research is essential for human health, as poor sleep quality has been found to be associated with an increased risk for cardiovascular and degenerative diseases, as well as an increased predisposition to infections [25,26]. In relation to the pandemic, a study published by L'Encephale in 2020 concluded that poor sleep quality during the pandemic was related to confinement and decreased sleep hours, in addition to reduced exposure to daylight and increased screen use at night [27]. A study by Brito-Marques, et al. in 2021 also observed that symptoms of depression, anxiety, and insomnia among physicians had a direct impact on sleep quality [28].
With the report of sleep complaints, the presence of anxiety symptoms was found to be positively correlated with sleep quality, as measured by the MSQ in the present study. Aside from the previously mentioned reasons for sleep complaints, it is well-established that sleep is important for mood regulation, showing a two-way relationship with anxiety. Wang, et al. (2021), in particular, assessed the risk of a quarantined population regarding the development of depression, anxiety and insomnia in comparison to control patients. It was found that younger, single and lower-income patients had a higher risk of anxiety symptoms when compared to older, less educated, married, and higher family income patients in quarantine [29], which can also be reflected in the population of this study, since we evaluated mostly young adult patients. Therefore, the follow-up of mental, psychological and sleep symptoms in all COVID-19 patients should be a priority in coping with this current pandemic.
Despite these findings, this study had certain limitations, including the evaluation of patients outside the transmission period, the subjective assessment of sleep- and anxiety-related symptoms, and the absence of diagnostic tests for all cases of mild flu syndrome.
The evolution of olfactory dysfunction occurred mostly and suddenly with other general clinical symptoms. Anosmia was the most prevalent dysfunction, and they evolve with a greater average of days with olfactory disorders when compared to patients with other types of olfactory dysfunction.
Participants who used oral or topical medication had no difference in their evolution. Patients with olfactory dysfunctions proven by the objective and qualitative tests with essences commonly had nasal structural and inflammatory alterations.
As can be seen, there is an evident change in the quality of life of patients with mild flu syndrome and a positive COVID-19 test, and these are due to changes in sleep quality, excessive sleepiness and expressive symptoms of anxiety.
To the Foudation Hospital Adriano Jorge (FHAJ/AM) and Hospital Adventista de Manaus for their institutional support. To the Amazonas Research Support Foundation (FAPEAM) for the financial support.
The authors declare that there are no conflicts of interest.
Luana Mattana Sebben foi responsavel pela curadoria dos dados, analise formal, investigacao, administracao do projeto, supervisao e validacao. Alem disso, liderou a escrita do rascunho e manuscrito final.
Dr. Diego Monteiro de Carvalho liderou a conceituacao, analise formal, metodologia, administracao do projeto e supervisao da pesquisa.
Dr. Jose Cardoso Neto liderou a curadoria de dados, programas, validacao e visualizacao.
Dr. Joao Bosco Lopes Botelho foi responsavel pela conceituacao, analise formal, administracao do projeto, supervisao e visualizacao.
Dr. Alvaro Siqueira da Silva foi responsavel pela conceituacao, supervisao e analise formal.
Dr. Carlos Mauricio Oliveira de Almeida foi responsavel pela conceituacao e analise formal.
Dr. Marcus Vinicius Della Coletta auxiliou na conceituacao e supervisao final da pesquisa.
Juliana Costa dos Santos foi responsavel pela investigacao, curadoria e administracao do projeto.
Mr. Ricardo de Queiroz Freitas foi responsavel pela investigacao e visualizacao.
Mr. Wenberger Lanza Daniel de Figueiredo auxiliou na investigacao, administracao do projeto e foi responsavel pelos programas.