Sarcoidosisis a chronic granulomatous condition that primarily affects the respiratory system. Its aetiology remains poorly understood. Isolated sarcoidosis of the palatine tonsils, when there is no evidence of disease elsewhere, is very rare occurrence, with only a few reported cases in the literature. We report the case of a 59-year-old man presenting with unilateral swelling of a tonsillar pillar, associated with dysphagia and dysphonia. The histopathology report on the tonsillectomy biopsy specimen shows the presence of noncaseating granulomatous lesions compatible with sarcoidosis. Culture did not grow any organisms and Ziehl-Neelsen stain was negative for acid-fast bacilli. Further investigations to exclude other sites of involvement were negative. This case is a reminder that sarcoidosis should be considered in the differential diagnosis of tonsillar pillar/oropharyngeal swelling. When non caseating granulomatous lesions are found in a tonsillar specimen, the work up should include investigations to confirm the disease, to detect any multisystem involvement, and to exclude an underlying malignancy.
Sarcoidosis is a chronic granulomatous condition that primarily affects the respiratory system, where it manifests as pulmonary infiltrations and hilar lymphadenopathy. Ocular and cutaneous lesions are not uncommon. Head and Neck manifestations of sarcoidosis are also not that rare a finding [1,2].
Isolated tonsillar sarcoidosis in the absence of other systemic manifestations of the disease is a very rare occurrence [3]. There are very few reports in the literature of such an isolated presentation.
The diagnosis of Sarcoidosis relies on three criteria, a compatible clinical and radiologic presentation, pathological evidence of non caseating granulomas and exclusion of other diseases which can mimic the disease such as malignancy and certain infections [4].
Sarcoidosis affects primarily young and middle age adults. Presenting complaints usually include an unexplained cough, shortness of breath and constitutional symptoms. Patients may be asymptomatic in the early phase of the disease. The cornerstone of treatment is usually corticosteroid therapy. Advanced disease may require immunosuppressive therapy [4].
The differential diagnosis includes [4]:
a) Toxins- drug induced hypersensitivity reactions, foreign body granulomatosis
b) Immunodeficiency - Chronic granulomatous disease, Common variable deficiency
c) Infections - Bacterial tuberculosis, brucellosis, fungal, parasites and viral -HIV
d) Inflammations- Bronchogenic granulomatosis, Esonophilic granulomatosis
e) Malignancy - Lymphoma, sarcoidosis like granuloma reactions from primary tumours and regional lymph nodes
f) Vasculitis - Churg -Strauss Syndrome and Granulomatosis with polyangiitis (Wegener granulomatosis)
There are no reliable biomarkers for the disease. While the serum Angiotensin Converting Enzyme (ACE) can be elevated in up to 75% of untreated patients, it lacks specificity and does not consistently correlate with severity of the disease [5].
Imaging is required in the assessment of the disease. CT Chest can show bilateral hilar lymphadenopathy and diffuse interstitial changes in lung parenchyma. F- Flurodeoxyglucose positron emission tomography is helpful to identify areas which can be biopsied. It can identify cardiac involvement and may correlate with disease activity. Gallium scan can show an increased uptake in hilar and paratracheal lymph nodes, as well as in the parotid and lacrimal glands. Magnetic Resonance Imaging (MRI) can identify Central Nervous System involvement. Cardiac Magnetic Resonance Imaging can show myocardial involvement [6,7].
A 59-year-old male with no significant past medical history presented with a 3-week history of dysphagia, dysphonia and swelling in the left oropharyngeal area. On examination, no lymphadenopathy was noted in the neck. Intraoral examination showed erythema and oedema of the left anterior and posterior tonsillar pillars. The oedema was obscuring the view of the tonsils. The erythema extended towards the soft palate on the left side. The right tonsil and the right side of the oropharyx looked normal. Flexible endoscopy revealed oedema of the left lateral pharyngeal wall and the left arytenoids.
The patient had no constitutional symptoms and was a non smoker and non drinker. His blood profile was unremarkable. A CT of his neck shows mucosal thickening only on the left side of the oropharynx, hypopharynx, epiglottis, and of the left arytenoid, with a soft tissue mass extending to the parapharyngeal fat pad. An MRI Neck shows oedema and enhancement of the epiglottis, the left aryepiglotic fold, the left tonsillar fossa and the posterior pharyngeal wall. This was interpreted likely being due to an infective or a neoplastic process. A PET Scan shows uptake confined to the left oropharyngeal and non odal or metastatic disease.
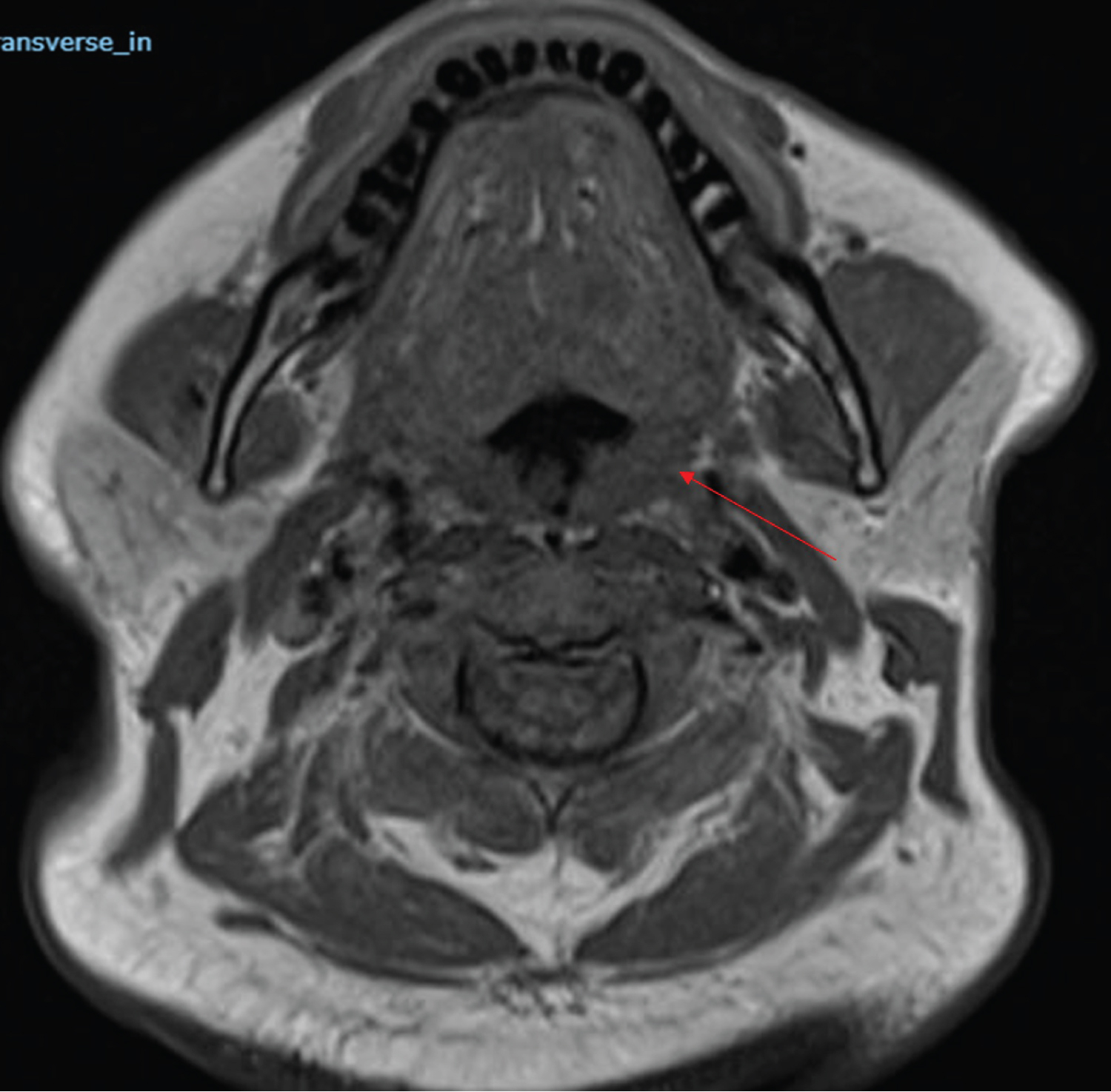 Figure 1: A T1 MRI of his neck shows mucosal thickening only on the left side of the oropharynx, hypopharynx, epiglottis, and of the left arytenoid, with a soft tissue mass extending to the para pharyngeal fat pad.
View Figure 1
Figure 1: A T1 MRI of his neck shows mucosal thickening only on the left side of the oropharynx, hypopharynx, epiglottis, and of the left arytenoid, with a soft tissue mass extending to the para pharyngeal fat pad.
View Figure 1
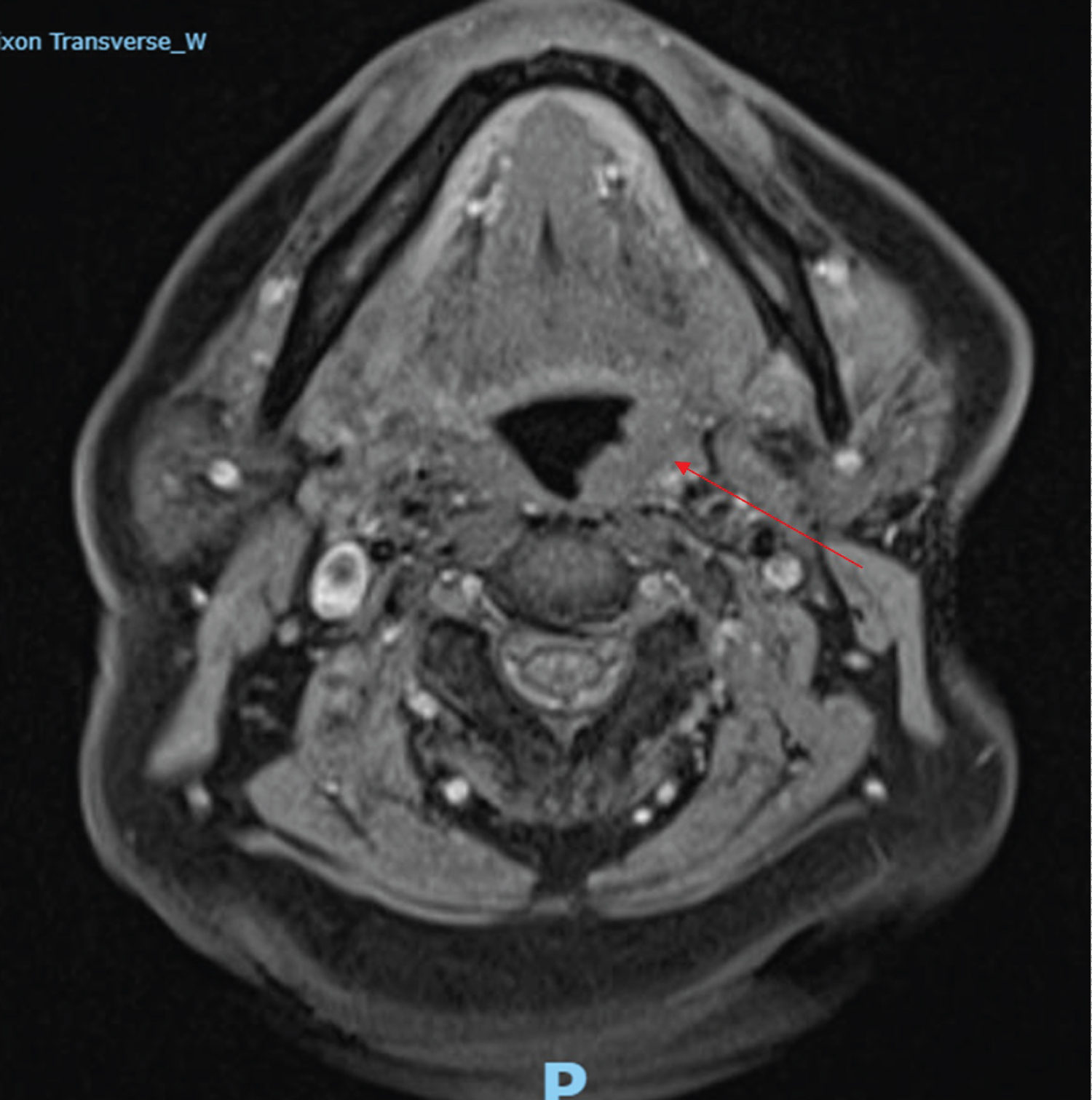 Figure 2: A T2 MRI Neck shows oedema and enhancement ofthe epiglottis, the left aryepiglotic fold, the left tonsillar fossa and the posterior pharyngeal wall.
View Figure 2
Figure 2: A T2 MRI Neck shows oedema and enhancement ofthe epiglottis, the left aryepiglotic fold, the left tonsillar fossa and the posterior pharyngeal wall.
View Figure 2
 Figure 3: A T2 MRI showing edema of left hypopharynx.
View Figure 3
Figure 3: A T2 MRI showing edema of left hypopharynx.
View Figure 3
The patient underwent an esophagoscopy and tonsillar biopsy. The cervical esophagus, pyriform fossa and posterior pharyngeal wall all looked normal. There was oedema of the anterior and posterior tonsillar pillars with significant fibrosis of the oropharynx. There was also some swelling of the left lateral oropharyngeal wall. The base of the tongue, the right tonsil and the right side of the oropharynx looked normal. An incisional biopsy of the left tonsil was sent for histopathology, lymphoma protocol and for microbiology.
Histology shows numerous well formed non-necrotising granulomata. There is no evidence of suppuration. Special stains for mycobacteria and fungal elements are negative.
Based on the histology, the absence of evidence of infection or malignancy and no systemic manifestations of sarcoidosis, a diagnosis of isolated tonsillar sarcoidosis was made.
Sarcoidosis is a chronic granulomatous condition characterised histologically by non-caseating granulomas. Isolated involvement of a tonsil is very uncommon.
When Kardon, et al. reviewed the histopathology of 26,386 tonsillectomy cases, they identified 22 cases of isolated tonsillar granulomas, representing 0.08% (22/26386) of cases. Of those 22 cases, 7 had a diagnosis of sarcoidosis, 3 had tuberculosis, 2 had Hodgkin's disease, 1 had Squamous Cell carcinoma and 1 had toxoplasmosis. The rest were classified as idiopathic or unknown. Tonsillar sarcoidosis accounts for less than 0.03% of all tonsillectomy cases examined at their institution. They postulated that isolated tonsillar sarcoidosis could represent a response to the usual pathogens that lead to chronic tonsillitis, given that 8 of these patients had a clinical diagnosis of chronic tonsillitis on presentation [8]. As our patient did not have features to suggest tonsillitis, it is unlikely his histological findings are due to a response to a chronic infective process.
Sarcodosis of the head and neck area is relatively rare and is found in 2-18% of generalised cases. It can present in the ears, sinonasal region, pharynx, larynx and very rarely the tonsils [9]. The histological detection of isolated sarcoidosis in tissue of the waldeyer's ring is a very rare occurrence [10,11].
When Rogers, et al. examined reports of sarcoidosis in the upper respiratory tract of children, they only found 13 cases documented in the literature. The most common documented symptoms on presentation in the paediatric group were - in decreasing order- localised erythema and oedema, a singular mass, the presence of punctiform submucosal nodules [12].
In the case we present, the patient had dysphonia, dysphagia and localised erythema and oedema.
Based on our patient presentation, we conclude that tonsillar sarcoidosis can manifest as erythema, oedema of surrounding tissues as well as dysphagia and dysphonia. Abnormal tissue architecture (fibrosis) of the tonsillar pillars was also noted.
A definite diagnosis of isolated unilateral tonsillar sarcoidosis requires exclusion of other possible pathologies such as lymphoma, squamous cell carcinoma and infective processes like Tuberculosis.
While less than 2% of patients with sarcoidosis have hypercalcemia, the workup in our patient showed a normal calcium and ACE level. Given the presentation, the Imaging and Histopathology was reviewed by the Head and Neck Tumour Board. Their consensus opinion was that this represented an extremely rare case of Isolated Tonsillar Sarcoidosis with no systemic manifestations of the disease.
While Karakantza, et al. have postulated that sarcoid disease can predispose to lymphoid malignancy due to a disturbance of the immune system, this theory was however not supported by Seersholm, et al. who followed 245 patients for 25 years [13,14]. Given the unusual presentation, we plan to follow our patient up with a repeat PET scan in the upcoming months.
Isolated tonsillar sarcoidosis can be an unexpected finding in a patient presenting with tonsillar asymmetry and localised oedema and erythema of a tonsillar pillar and the surrounding tissue. The patient may present with symptoms such as dysphagia and dysphonia. In such cases, clinical vigilance is warranted. Other pathologies such as lymphoma, squamous cell carcinoma, infective processes and foreign body/immune mediated conditions should be excluded. When sarcoidosis is confirmed, involvement of other sites should be excluded.
Declarations of interest from both authors: None.