Obesity is a national epidemic resulting in significant morbidity and mortality. Weight loss as modest as 5% of body weight significantly reduces the risk of hypertension, diabetes, and cardiovascular disease. The primary aim of this pilot study was to test the efficacy of a text messaging intervention in a primary care setting to motivate overweight patients to lose weight and reduce their waist circumference.
A total of 128 adult primary care patients who were overweight and classified as abdominally obese via waist circumference measurement were randomized to enhanced care (EC, n = 62) or standard care (SC, n = 66). Patients assigned to both groups met with the physician, and the SC received a standard clinic brochure on weight loss. In addition to the brochure, the EC group met with a research assistant to discuss the risks of abdominal obesity and resources to lose weight in addition to receiving 3 motivational text messages per week for 12 weeks and 2 phone calls to check in on their progress. At baseline, three, and six months, all patients had a survey administered and weight, waist circumference and blood pressure were obtained.
In the EC group, 50% (n = 16) reported reading all of the text messages, 31% (n = 10) found the text messages helpful, and 84% (n = 26) reported using the diet and physical activity resources provided. The average weight loss at six months was 4.3 pounds in the SC group and 3 pounds in the EC group (p = 0.17). The average reduction in waist circumference at six months was 0.5 inches in the SC group and 1.2 inches in the EC group (p = 0.15). The most commonly reported diet change was reducing calories, with 28% (n = 17) and 36% (n = 18) reporting a low-calorie diet at three and six months, respectively. At six months, 26% (n = 13) reported engaging in cardiovascular exercise like jogging aerobics or swimming, while 24% (n = 12) reported engaging in some form of weightlifting as a change from baseline.
This pilot study demonstrated the potential feasibility of a simple, texting-based intervention designed to motivate overweight individuals to lose weight and reduce their waist circumference in a primary care clinic. Both groups showed modest weight loss, slightly favoring the SC group, and waist circumference reductions favored the intervention group, although neither result was statistically significant. Future studies need creative ways to increase intervention exposure and harness the potential for mobile technology-based health coaching. While constraints of time and infrastructure may limit personalized counselling, mobile technology may serve as an excellent adjunct medium of communicating with patients about resources related to healthy eating and exercise. Novel methods for boosting the effectiveness of technology-based interventions are needed.
Obesity is currently a national epidemic and 71% of the US population over the age of 20 are overweight/obese based on a BMI equal to or greater than 25, and 37% are obese based on a BMI greater than or equal to 30 [1]. The prevalence of obesity and associated metabolic co-morbidities has significantly increased in the United States in the past two decades with an estimated annual medical cost of obesity in the U.S. at $147 billion dollars in 2008 [2]. The literature is clear that overweight/obesity is related to an increased risk of morbidity and mortality. Studies have shown that modest weight loss of 5% to 10% in patients who are overweight/obese can improve blood pressure, lipid levels and hemoglobin A1C levels and can reduce progression of disease [3-6].
While body mass index (BMI) has long been established as the clinical standard for diagnosing obesity and assessing the risk of obesity-related syndromes, several recent studies have shown that waist circumference (WC) may better predict risk of hypertension, type-2 diabetes, dyslipidemia, metabolic syndrome, and general cardiovascular (CVD) outcomes. One meta-analysis found that compared to BMI, WC improved discrimination of adverse outcomes by 3% (p < 0.05) and in light of this there is a growing need to universally use waist circumference measurements in addition to BMI to adequately risk stratify patients [7]. The Shape of Nations study revealed that worldwide, 45% of all physicians reported never measuring waist circumference and 59% of at-risk patients had not been informed by their doctors about the link between abdominal obesity and heart disease [8]. Considering the above facts, it is critical to include waist circumference as an important anthropometric measure to be used by health care providers when stratifying risk and giving lifestyle coaching to patients.
Despite the availability of guidelines recommendations on strategies for managing obesity, the successful prevention and treatment of this condition remains an unmet goal in most clinical practices. Evidence shows that patients tend to lose more weight when counselled by their primary care physician, but lack of time, resources and knowledge are barriers that physicians report when asked on treatment of obesity. Short term weight loss may be achieved by commercial diet programs but a majority of them struggle with weight maintenance and long-term compliance. Effective approaches should be aimed at changing behavior patterns to ensure long-term weight loss.
One of the areas which has been researched in the area of weight loss is self-monitoring which not only increases awareness of food and caloric intake but stresses on the importance of enhancement of self-efficacy and allows for monitoring progress and long-term results [9]. Mobile technology is rapidly advancing and the use of text messaging and internet resources to educate and motivate patients on interventions related to weight loss has been actively pursued. The widespread use of cellular phones among different age groups, socio-economic backgrounds and population groups make it a feasible medium to deliver weight loss interventions [10]. This mode of intervention may provide an easy and cost-effective platform with the use of frequent reminders and educational information on healthy behavior patterns and physical activity. Studies have been equivocal in demonstrating weight loss using text messaging with many of them being limited due to number of patients enrolled and also lack of statistical power in demonstrating meaningful weight reductions. Most of the studies examined weight loss with the use of mobile technology but limited studies demonstrated association with WC. Thus, this pilot study was developed as a randomized-controlled quality improvement intervention to include the measurement of waist circumference in addition to BMI to risk stratify overweight patients and to study the efficacy of a low-cost intervention using text messaging to provide education on weight loss and lowering waist circumference measures among overweight patients. Further, this project aimed to compare if enhanced weight loss interventions using text messaging and follow-up phone calls resulted in increased efforts by patients to lose weight and reduce waist circumference, as compared to the standard weight loss counselling given by the physician as a part of a routine clinic visit.
This pilot study was conducted at an urban, academic family medicine clinic. The study was reviewed and approved by the local institutional review board. The research assistant approached 313 patients who were coming in for doctor visits to the above clinic between April 2015 and March 2016. Initially adult patients over the age of 18 classified as overweight by BMI between 25 and 29.9 kg/m2; (ethnic cut offs by WHO of 23.0-24.9 kg/m2 for Asians were used when appropriate) were identified [11]. These patients then had their WC measured and if qualified as abdominally obese > 102 cm (40 in) in men and > 88 cm (35 in) in women (based on International Diabetes Federation (IDF) criteria; ethnic cutoffs of > 90 cm in men and > 80 in women were used when appropriate [12]) were invited to participate in the study. Additional inclusion criteria were: The patient should have a phone capable of receiving text messages and should be able to read English. A total of 178 patients were eligible, and 128 patients consented to be randomized to one of two groups: Standard care (SC) or enhanced care (EC). A randomization-allocation log was created using a random number generator (randomization.com), stratified based on insurance type (public vs. private). The research associate was blinded to condition prior to participant randomization.
Those assigned to SC were provided with a brochure containing information on abdominal obesity and associated health risks, along with the routine counselling during the office visit. Those assigned to the EC group also received the brochure and met with the research assistant or nurse to discuss their WC and strategies to lose weight and reduce their risk of obesity-related diseases. The information discussed with the patients was scripted and was universally delivered to all the patients via the BigTxt program. Text messages were author constructed and sent out automatically in a pre-determined order via the web based BigTxt web application. BigTxt recorded information on delivery times and failed messages. Example text messages included "Tip: Swap fatty sour cream with fat-free Greek yogurt - one of the world's healthiest foods!", and "Keep track of the calories you consume per day. This can be done using a smartphone, computer, or a food journal". They also received motivational text messages (three per week for 12 weeks) on healthy eating tips and physical activity. Resources on the web related to weight loss were also a part of the text messaging. Participants had their weight, height, and waist circumference measured in the office at baseline, 3 months and 6 months and completed an interview conducted by the research assistant at all three visits. If for some reason a patient was unable to come to clinic for the three or six month visit, the survey was administered over the phone (n = 7 at 3 month and n = 15 at 6 month) and patients were encouraged to come in at a convenient time to have their anthropometric measurements taken. There was also a phone call placed at one month and four months post-randomization to the EC group to answer any questions the patients had regarding the study or the resources they had received.
The primary endpoint in this study was a reduction in WC over the period of 6 months. The primary outcome were measured via nurse recorded WC, weight, and height data for all patients at each of their 3 clinic visits. The survey that was administered to the patients at the baseline visit included demographic data, smoking and alcohol use, their current exercise habits and also their initial knowledge regarding WC and its associated risk with chronic medical conditions. The subsequent 3- and 6-month surveys reevaluated their knowledge to demonstrate improvement and also had specific questions to the enhanced group on the efficacy and utility of the text messaging. Anthropometric data were collected at each of the follow-up visits. The final 6-month interview assessed the readiness of the patients to continue their weight loss efforts after the completion of the study.
Frequentist statistics were used to describe the study sample and compare demographic characteristics of the two groups. Repeated measures ANOVA was used to compare mean WC and weight between study groups across all three visits. Spearmann correlation was used to determine if WC was correlated with any other health-related behaviors or conditions. All analyses were performed in SAS version 9.4 (Cary, NC).
One hundred and twenty-eight patients were enrolled, with 62 randomized to Enhanced Care (EC) group and 66 to the Standard Care (SC) group. Sixty-one (48%) patients completed their 3-month follow-up and 51 (40%) completed their 6-month follow-up. (Figure 1). A total of 2242 text messages were sent using BigTxt, an automated text-messaging program, 2179 messages were successfully delivered and 63 were noted as failed. Of the patients who completed the 3-month follow-up, nearly 91% reported having read greater than 50% of the text messages. The mean age of the patients was 54 years and females constituted 70% of the enrolled patients, with African Americans representing 52%. Most of the enrolled patients had completed high school and close to 50% of the patients had hypertension. About 40% reported exercising 1-2 times per week and 18% reported exercise 3-4 times a week and about 34% (n = 43) reporting no form of exercise. The average weight and WC at baseline was 175.2 pounds and 38.9 inches respectively (Table 1).
Table 1: Baseline demographic and health characteristics of participants (n = 128). View Table 1
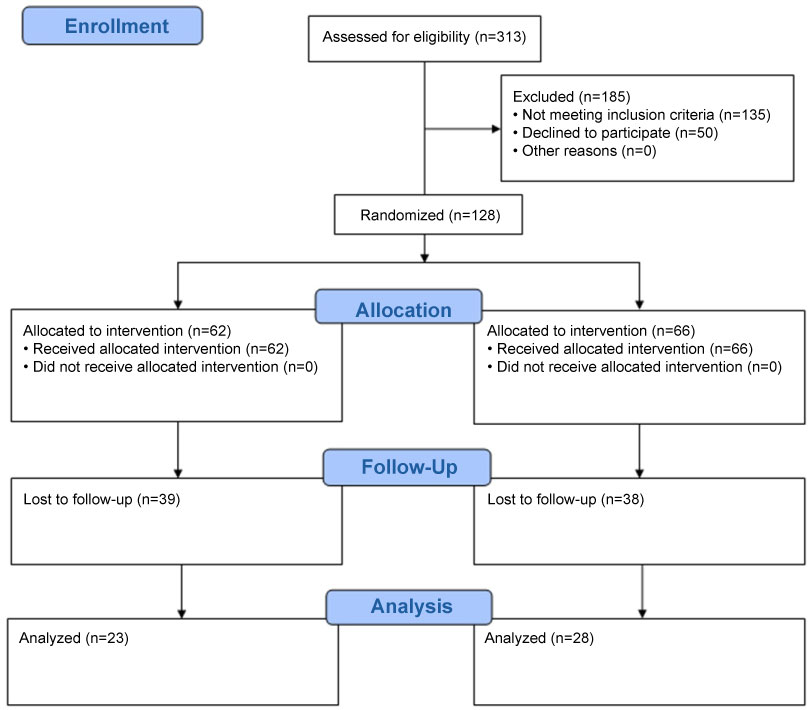 Figure 1: Consort diagram. View Figure 1
Figure 1: Consort diagram. View Figure 1
Regardless of study group, patients overall weighed less at the end of the six-month follow-up period. However, the weight loss seen in both groups was modest, with the SC group losing an average of 4.3 pounds per person and the EC group losing an average of 3 pounds per person. The EC group had a 1.2-inch average reduction in their waist circumference over the period of 6 months compared to an average 0.5-inch loss among the SC group (Table 2). Using repeated measures ANOVA to compare mean WC between study groups across the three visits, no effect of treatment on WC was found, and similarly, no effect of treatment was found when comparing baseline WC to any follow-up WC (p = 0.34 and p = 0.24, respectively). No effect of treatment on weight, systolic and diastolic blood pressures was found. Using Spearmann correlations it was found that WC at either follow-up visit was positively correlated with binge drinking frequency (ρ = 0.71).
Table 2: Weight and waist circumference over the period of 6 months from baseline. View Table 2
At baseline, 82% (n = 104) reported not having tried a weight loss program in the past year and close to 75% (n = 94) of the patients reported that they never exercise or exercise less than 1-2 times per week with only 8% (n = 11) reporting exercising > 5 times per week. Approximately 30% (n = 17) of all patients reported that they adopted a low-calorie diet post program at 3 months and about 36% (n = 18) reported being on a low-calorie diet at 6 months. Roughly 25% (n = 13) of the patients reported doing some form of cardio exercise and weight training at 6 months (Table 3).
Table 3: Self-reported attempts to lose weight and reduce waist circumference at follow-up. View Table 3
Nearly all (94%; n = 118) patients were aware of a relationship between abdominal fat, health, and an increase in heart attacks. There was no statistically significant difference seen in knowledge at 6 months among the SC and EC group. About 40% (n = 24) of patients across the EC and SC groups reported having made some effort to reduce waist circumference at 3 months which dropped slightly to about 30% (n = 15) at 6 months. About 25% (n = 15) of all the patients reported an effort to lose weight at 3 months which increased to 35% (n = 18) at the end of 6 months. There was no statistical difference in the effort reported to lose weight or reduce waist circumference on comparison of the SC and EC groups.
Almost one third of the EC group reported that the information obtained via text messaging was extremely helpful and about 85% reported having used the diet and physical activity resources that were provided. About 50% of the patients at 6 months reported that text messaging and brochures would be helpful in future interventions to promote weight loss and about 26% reported that they would continue their efforts to reduce WC and weight post their last intervention visit.
This quality improvement project was conducted to evaluate a simple quality improvement intervention using text messaging to provide health coaching to reduce waist circumference and weights among overweight patients. Small differences were found in weight loss (favoring the SC group) and waist circumference (favoring the EC group) but these modest changes were not statistically significant across the two groups. However, in the EC group patients expressed readiness and interest in the use of medical technology for health coaching. Unlike similar studies, which used a multi-faceted approach involving internet resources, text messaging, and face-to-face behavioral therapy [13], the aim of our study was to investigate the efficacy of a simple and very low to no cost mobile technology using text messaging to motivate patients to make changes in their life style relating to diet and exercise that could be realistically implemented in primary care. Though this study did not show a statistically improvement in the weight measures, about 30% of participants reported that the text messaging was extremely helpful and about 85% reported that they used the dietary and physical activity resources mentioned in the text messages.
It has also been shown that physician directed education geared towards weight loss has resulted in successful weight loss [14]. The widespread use of mobile phones provides a unique opportunity to enhance effect of a health coaching intervention due to its ease of access, cost-effectiveness and barrier reduction related to time and transport to a health care facility.
Studies of mobile phone interventions have shown positive correlations in reducing diabetes risk, increasing physical activity and tobacco cessation but the results relating to text messaging and weight loss have been controversial [12]. Studies have shown statistically significant weight loss when text messaging was combined with a mix of delivery modes, such as email, phone calls, intensive web-based health coaching and or face-to face meetings [12,15]. Arguably, a challenge to implementation in primary care. A study by Silina, et al. [16] examined whether text messaging facilitated weight loss and a reduction in waist circumference among overweight/obese patients. The study did have laboratory and CT evaluation included with the anthropometric measures pre and post-intervention, text messaging was delivered over a period of one year. The study did show statistically significant weight loss and change in laboratory values inferring that the use of text messaging may be a viable platform for information regarding weight loss [16].
A meta-analysis of 14 randomized control trials conducted by Liu, et al. with more than 1300 participants documented significant decrease of approximately 1.44 kilograms in body weight associated with mobile phone intervention. There was no association between a mobile phone intervention and waist circumference, this could be explained by the limited number of studies exploring the relationship of this anthropometric measure [12]. Another meta-analysis done by Schippers, et al. included 12 randomized controlled trials assessing the efficacy of weight loss interventions using mobile technology [15]. These trials resulted in significant weight loss, but the weighted average effect size for weight loss found in this analysis was small to moderate. One of the important findings of this above meta-analysis was results indicated that weight loss interventions delivered via mobile phones were efficacious, but it was necessary to enhance them with other forms of contact like phone, email, or face to face conversations [15]. A study by Patrick, et al. [9] evaluated a text message-based intervention for weight loss among 65 patients over a period of 4 months. The study used text messaging, a personalized mobile phone-based application to improve dietary behaviors, goal setting and self-monitoring [9]. The results showed an adjusted average weight loss of about 2.88 kilograms among the intervention participants as compared to the controls indicating that text messages might prove to be a good form of communication to promote healthy behaviors [9]. One 3-armed randomized controlled trial of 385 overweight and obese patients compared the efficacy of a weight loss intervention delivered by a cell phone application, personal contact enhanced by the cell phone application and usual care. This study showed that the cell phone application arm showed the least amount of weight loss with no significant difference from the control group but the group with the personal contact in addition to the cell phone intervention did show a significantly greater weight loss at 6 months [4,14]. Our study was very similar to the above, but with the caveat that there was no additional health coaching or other components that were provided in addition to text messaging which may explain the lack of weight loss differences found in our study.
Due to modest weight loss in both intervention groups it is hard to draw conclusions on the benefit of the use of text messaging as a form of health coaching for weight loss, but participants did repot using the resources obtained via the text messaging and found it very helpful to incorporate into their lifestyle. Our study did show the that text messaging maybe a good platform for health coaching related to weight loss, but reiterated the need for future studies to explore the benefit of text messaging with the use of additional strategies like personalized web programs, phone contacts and behavioral therapy to obtain significant and sustained weight loss. The loss of patients to follow up due to barriers related to access, cost and lack of incentive for the visit just to measure anthropometric data limited this study from drawing conclusive inferences on the benefits of text messaging as a health coach for the management of obesity and overweight. This study was limited only to the measure of anthropometric data which may not accurately predict risk of morbidity. The use of laboratory evaluation (e.g., lipids and insulin levels) would have provided additional information on risk stratification. The loss of patients to follow up resulting in a reduced number of patients at the conclusion of the 6 months of intervention was the most significant limitation of this study. Like other studies, there was a significant female representation in this study and sociodemographic diversity was limited, with 50% of the population being African American thus making it difficult to study the impact of the intervention among different ethnic groups. As information on income was not available no conclusion on socio-economic status could be drawn.
In conclusion, it is well known that obesity is a risk factor for multiple co-morbid conditions and there is a growing need for health care providers to be more involved in the weight loss strategies of their patients. While constraints of time and infrastructure may limit personalized counselling, mobile technology may serve as an adjunct medium of communicating with the patients in regard to resources related to healthy eating and exercise. This study was limited due to the number of patients and did not show significant weight loss among the EC group, however it did highlight the readiness among patients to use mobile technology to receive health coaching. This study also showed the need to develop and test multi-component interventions such as web resources and personal face-to-face contact in addition to text messaging to see if the impact on weight loss and other anthropometric measures is significant and sustained. There is an urgent need to further study ways to enhance weight loss in the current milieu of restricted time, finances and resources using mobile technology due to its low cost and high-volume patient accessibility.
The study was funded by the Texas Academy of Family Physicians (TAFP) in the amount of $5000; TAFP had no role in the design or execution of the project.