Overweight and Obesity among adolescents constitute medico-social menace with rising prevalence. This study, therefore, determined the prevalence of Overweight and Obesity and assessed the factors associated with Obesity/Overweight.
This was a school–based cross-sectional study. Consenting secondary school adolescents aged 10 to 18 years in Owo Local Government Area completed a pretested semi structured questionnaire. Anthropometric parameters were measured using standard methods. Overweight and Obesity were defined using Centre for Disease Control Body Mass Index percentile cut-off. Data were analysed using descriptive and inferential statistics.
A total of 1000 adolescents were evaluated, 41 (4.1%) were Overweight while 13 (1.3%) were obese. There was female preponderance for both Overweight (53.7%) and Obesity (53.8%). Obesity was predominance among those in high social classes. The proportions of Overweight and Obesity were more among the early adolescents (46.3% and 61.5% respectively). Overweight and obese adolescents had significantly higher mean for triceps skinfold thickness, waist circumference, hip circumference, and subscapular skinfold (p < 0.001). The factors associated with obesity and overweight were types of school attended and participation in school physical activities. The predictor of obesity was the type of school attended. Adolescents who attended private schools were three times more likely to be obese (OR = 2.6; 95% CI: 0.082-0.815; p = 0.021).
Routine screenings for Overweight and Obesity among school-aged adolescents is highly recommended for early treatment and follow up. The schools should inculcate physical exercise in the school curriculum.
Adolescents, Body mass index, Factors, Nigeria, Obesity, Overweight, Prevalence, School
Overweight and Obesity are potential health problems in Nigeria because of the increasing prevalence despite poor socioeconomic situation [1]. Obesity and Obesity-related morbidities are non-communicable diseases that are fast becoming an epidemic not only in developed countries but surprisingly in developing countries like sub-Saharan Africa [1,2]. In the recent past, communicable diseases form the bulk of the disease burden in the region, but with the current rising trend of Obesity, both non-communicable and communicable disease are bedeviling the region, a situation that has been dubbed the double burden of disease situation [3,4].
Obesity is the accumulation of excessive adipose tissue mass resulting in Body Mass Index (BMI) that is equal to or greater than the 95th percentile for age and sex in children [5]. Body Mass Index is an index of adiposity and it is defined as weight (in kilogram, kg) per the square of the height (in meters, m) (weight/height2) [6]. Body Mass Index greater than or equal to 30 kg/m2 is considered as Obesity [5]. Overweight, on the other hand, is defined as BMI equal to or greater than 85th percentile and below 95th percentile for age and sex in children or BMI equal to or greater than 25 kg/m2 [5].
Adolescent Obesity often persists into adulthood with the attendant morbidities [7]. The poor success rate of treatment of adult Obesity informs the urgent need to develop preventive measures in children. In United States of America, the prevalence of Obesity among adolescents was 17 percent [8]. Six hundred million people are estimated obese worldwide; seven percent (43 million) of this population are children [9]. In African, the prevalence of Obesity is estimated to be 8.5% in 2010 [10]. While in Nigeria the prevalence ranged from 0.2 to 18% [3,11,12]. Going by this rising trend in prevalence of Obesity, these figures could double by the year 2025 if no action is taken [9].
Obesity is caused by interaction of environmental factors, genetic predisposition and human behavior and is associated with an increased risk of numerous chronic diseases, ranging from cardiovascular diseases, diabetes, cancers and other systemic diseases [13]. Overweight and Obesity have become a global epidemic that has contributed to the increasing burden of Type 2 diabetes, cardiovascular diseases, strokes, cancers, and premature deaths worldwide [14]. Unfortunately, Overweight and Obesity are erroneously taken as a sign of good living especially in developing countries hence efforts have been geared towards raising awareness to its deleterious effects [14]. It has been opined that Obesity will almost always put the victims at health risks [9].
The seemingly elusive nature of Overweight and Obesity makes parents and even the healthcare provider delay intervention. Failure to make an early diagnosis of this condition and to institute corrective measures could predispose to early development of insulin resistance [10]. This, in turn, could put the affected children at risk of developing metabolic syndrome [10].
There are certain environmental and behavioral factors which predispose to Overweight and Obesity. These factors include sedentary lifestyle, high consumption of energy - dense food, reduced participation in exercise among others [15]. Many studies have been done both in developed and some developing countries in order to explore the association between these risk factors and Overweight/Obesity [3,9,12,15]. Some of these studies established a strong relationship between these risk factors and Obesity [3,14]. However, the association between these risk factors and Obesity has not been thoroughly studied among adolescents in Nigeria. Therefore, knowledge of its prevalence and predisposing factors will help in policy formulations leading to more timely interventions, thereby reducing morbidity and mortality from Overweight and Obesity. This study, therefore, attempted to document the burden of Overweight and Obesity as well as identify some of the risk factors contributing to its development.
The objectives of this study were to determine the prevalence of Overweight and Obesity, the relationship between parental socioeconomic class and Overweight/Obesity, the relationship between Overweight/Obesity and behavioural factors (diet, physical activities and screen time) and determine the relationship between Overweight/Obesity and waist-hip ratio and skinfold thickness among school-aged adolescents in Owo Local Government Area (LGA) using body mass index (BMI).
The study was carried out among secondary school students in Owo Local Government Area (Owo LGA), Ondo State, Nigeria. Owo LGA lies within latitude 7.1833°N and longitude 5.5833°E and is bounded by Emure-Ise-Orun Local Government Area of Ekiti State to the North; Akure and Idanre Local Government Areas of Ondo State to the East and South respectively while Ose Local Government Area of Ondo State forms the border to the West and part of the South [16]. According to the 2006 population census, the population of Owo is 218,886 and it occupies a land area of about 636 km2 [16]. The people are predominantly of the Yoruba tribe with few Igbos Ebiras and Igalas.
This was a cross-sectional school - based study. Ethical approval with registration number ZEO/OW/G-14 VOL II/245 was obtained from the Ministry of Education Zonal Education Office, Owo, Ondo-State, Nigeria and permission was obtained from the principals/proprietress of selected schools. Written informed consent was obtained from the parents/guardians of each eligible child and assent was obtained from each recruited child. The respondents were assured of the confidentiality of the information given and the data collected were entered and kept in a password protected computer.
One thousand school-aged adolescents aged 10-18 years were recruited for the study using a multistage sampling method. The number allocated to each group of students was determined using the formula n/N × 1,000, where n is the number in each group and N is the total number of students [17]. There were 33 secondary schools in Owo LGA, comprising 18 public and 15 private secondary schools. Consenting adolescents filled a pretested semi-structured questionnaire which was distributed consecutively during the break period and was filled. Adolescents with physical deformities who could not stand for height measurement were excluded. World Health Organization classification of adolescents was used in classifying the adolescents into early (10-13 years), middle (14-16 years) and late (17-18 years) adolescence [18].
Height (in centimetres) was measured with Leicester® stadiometer. The subjects stood erect, barefooted, feet together, chest out and looking horizontally straight ahead with the heel, buttock, and occiput touching the vertical plane of the instrument (Frankfort plane) [19]. The measurement was taken to the nearest 0.1 cm.
Weight (in kilograms) was measured using the analog weighing scale by SECA®, Great Britain with the participants wearing only school uniform and no shoes [19]. The scale was standardised before each measurement by ensuring the indicator returned to the zero mark. Also, commercially sold metals with known weights were used at weekly intervals for standardisation and readings were measured to the nearest 0.1 kg.
Skinfold thickness (in millimetres) was measured using Harpenden skinfold calipers. The caliper was used to grip the skin after pinching the skin with the index finger and the thumb at the appropriate sites to raise a double layer of skin and the underlying adipose tissue, but not the muscle. The caliper was then applied 1 cm below and at right angles to the pinch, and a reading in millimetres (mm) was taken two seconds later. The average of two measurements was then taken. Whenever the measurements differed greatly, a third measurement was done and the average was taken. The triceps skinfold was taken at the level of mid-point between the acromion and olecranon processes and the subscapular skinfold was measured just below the tip of the scapular. All the measurements were taken on the right side (for consistency) of the body.
Waist circumference (in centimetres) was measured with a flexible inelastic tape at the midway between the iliac crest and the lowest margins of the ribs, with the abdomen bare and at the end of normal expiration [19]. The trained female research assistant took the waist measurements for the female subjects.
Hip circumference/girth (in centimetres) was measured using an inelastic measuring tape placed round the hip at the inter-trochanteric level which corresponds posteriorly to the level of the greatest posterior protuberance of the buttocks and anteriorly to about the level of the symphysis pubis. The stub of the tape and the housing were both held in the right hand while the left hand was used to adjust the level of the tape at the back to the adjudged level of the greatest posterior protuberance of the buttocks. The tape position was adjusted in front and the sides so that the tape was held in a horizontal plane at the target level. The trained female research assistant took the girth measurements for the female subjects.
Body Mass Index (BMI) was estimated by dividing the measured weight in kilogrammes by the square of the height in metres (kg/m2). The BMI was grouped into underweight, BMI below 5th percentiles; normal weight, BMI from 5th to 84th percentiles; overweight, BMI of 85th and less than 95th percentiles and obesity, BMI of equal to or greater than 95th percentile using Centres for Disease Control and Prevention (CDC) BMI-for-age chart [20].
Data were analysed using the statistical package for social sciences (SPSS) software version 20 (SPSS Chicago Inc., IL, USA, released 2011). Subjects were classified as non-Overweight when the BMI is less than 85th percentile; Overweight with BMI of 85th percentile to less than 95th percentile and obese with BMI of 95th percentile or more. BMI and BMI percentiles were generated using the Nutstat component of the Epi Info software [21]. Values and the results were expressed as means, standard deviation for continuous variables and as proportions and percentages for categorical variables. Data were compared among the non-overweight, overweight, and obese. Chi-square and Student's t-test were used for categorical and continuous variables respectively. Binary logistic regression was used to analyse the predictors of Overweight and Obesity. Probability value p less than 0.05 were taken as statistically significant.
A total of 1000 subjects were recruited into the study comprising 500 each of males and females giving a male to female ratio of 1:1. Table 1 shows the demographic characteristics of the study population. The age range was 10 to 18 years with a mean age of 14.05 ± 1.98 years. Four hundred and thirty-three (43.3%) of the subjects were aged 10-13 years and were the predominant age group. Six hundred and eighty (68.0%) of the subjects attended public schools. More than three-quarter of the subjects were Christian (86.4%) and Yoruba (82.6%). Three hundred and forty-eight (34.8%) of the subjects were from social class 3 while social class 4 were 344 (34.4%) followed by social class 1 with 133 (13.3%) and social class 2 with 124 (12.4%) subjects while the least social class was social class 5 with 51 (5.1%) subjects.
Table 1: Demographic distribution of the subjects. View Table 1
The overall prevalence of Overweight was 4.1% while that of Obesity was 1.3% (Figure 1). Twenty-two (53.7%) of the 41 Overweight subjects were females putting the prevalence of Overweight among females to be 4.4% while that of males as 3.8%. Seven (53.8%) of the 13 obese subjects were females thereby placing the prevalence of Obesity among the females as 1.4% while among males as 1.2%. This gender-related difference in the prevalence of Overweight and Obesity was statistically significant (χ2 = 19.733, p = 0.001) as shown in Table 2.
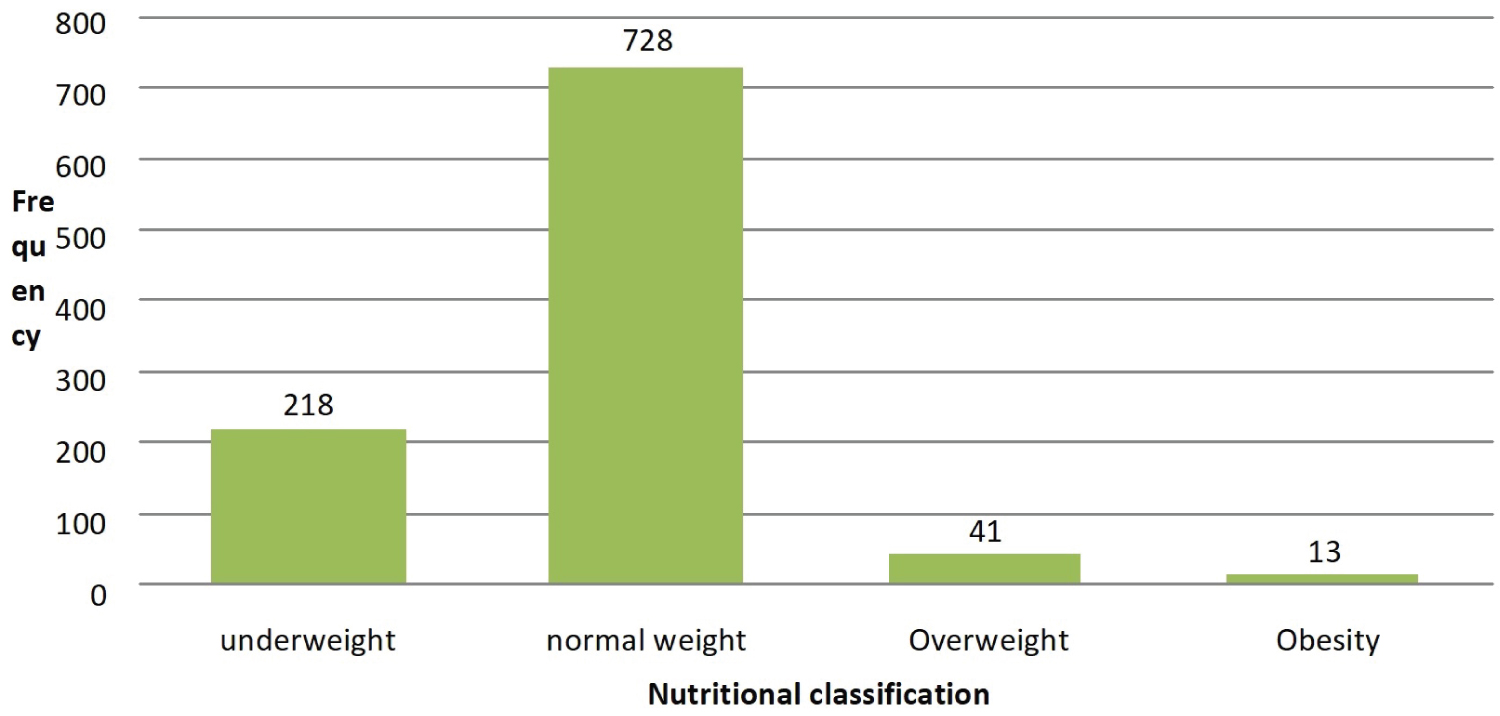 Figure 1: Nutritional classification of the subjects.
View Figure 1
Figure 1: Nutritional classification of the subjects.
View Figure 1
Table 2: Sex and nutritional classification of the subjects. View Table 2
Table 3 showed the mean distribution of anthropometric measurements of the subjects according to sex. The mean weight was similar for both sexes, however the boys were significantly taller than the girls (p = 0.005). The body mass index and waist circumference were significantly higher among female than male subjects (p < 0.05).
Table 3: Distribution of Anthropometric measurements according to sex. View Table 3
Table 4 revealed the factors associated with Overweight and Obesity. The proportion of subjects with Obesity was highest in social class 1 (3.0%) whereas none was observed among those in social class 5. Overweight was higher among class 5 (5.9%) followed by social class 4 (4.9%). This was no statistically significant. A statistically significant proportion of subjects attending private schools (2.5%) were obese compared with those attending public schools but Overweight was higher among public school students (p = 0.039). A statistically significant percentage of Overweight and obese subjects were involved in school physical exercise once per week (p = 0.008). Obesity and Overweight were observed more among the early adolescents with proportions of 1.8% and 4.4% respectively.
Table 4: Factors associated with Overweight and Obesity. View Table 4
The relationship between dietary pattern, alcohol consumption and Overweight and Obesity is shown in Table 5. Majority of Overweight (65.9%) and obese (46.2%) subjects took in-between-meal snacks daily. Only one (7.7%) of the obese subjects reported consuming alcohol at most once daily while the remaining obese subjects rarely or never took alcohol. However, no statistical significance was found between the differences in percentages of Obesity and Overweight in relation to number of daily meals, consumption of snacks, fast food, vegetable and fruit consumption, intake of soft drinks and alcohol consumption.
Table 5: Relationship between Dietary pattern/alcohol consumption and Overweight and Obesity. View Table 5
Table 6 showed the relationship between sedentary lifestyle and Overweight and Obesity. The proportion of subjects who were Overweight and obese increased with television viewing time and computer browsing time. However, there was no statistically significant difference between these sedentary lifestyles and Overweight and Obesity.
Table 6: Relationship between sedentary lifestyle with Overweight and Obesity. View Table 6
The mean anthropometric measurements of the study subjects in relation to nutritional status are shown in Table 7. Overweight and obese subjects had significantly higher mean for TSF, SSF, WC, HC, sum of TSF and SSF (p < 0.001). Table 8 showed the logistic regression analysis of factors associated with Overweight/Obesity. Type of school and participation in physical activities were not significantly associated with overweight from bivariate analysis but subjects who attended private school were three times more likely to be obese (OR = 2.6; 95% CI: 0.082-0.815; p = 0.021) compared to those who attended public school.
Table 7: Mean anthropometric measurements in relation to nutritional status. View Table 7
Table 8: Predictors of Overweight and Obesity using multiple logistic regression analysis. View Table 8
The overall prevalence of Overweight in this study was 4.1 percent while that of Obesity was 1.3 percent. This observed prevalence was about double for Overweight and quadruple for Obesity compared with what was documented earlier in Ile-Ife in southwestern Nigeria among children and adolescents [3]. The higher prevalence in the present study could be adduced to the inclusion of only adolescents in this present study unlike the Ile-Ife study that included children of all age groups. It has previously been reported that Overweight and Obesity are more common among adolescents [22], therefore inclusion of children outside the adolescent age group (in which Obesity is not as common) is likely to have a lowering effect on the prevalence of Obesity that will be obtained. In addition to this, the rising trend of Overweight and Obesity in the country and globally could also explain the higher prevalence in the current study [23,24].
The prevalence of Obesity in this study was markedly lower than the 11.5 percent reported in a study in Enugu [12]. The high socioeconomic status of the subjects studied by Nwaiwu, et al. [12] could have accounted for the higher prevalence rate of Obesity recorded in their study. These subjects are more likely to consume high calorie diet, have reduced activities, spend long hours at the screen and these ultimately lead to positive energy balance [2]. Also, the location of the study, Enugu, is a state capital expectedly with higher level of urbanisation compared to Owo, hence a higher prevalence of Obesity is not unexpected.
The prevalence of Obesity observed in the present study was also lower than those reported from outside Nigeria. Ogden, et al. [2], in 2012, reported a prevalence of 17 percent for Obesity in United State of America children. Al Seindi, et al. [25] among the Bahraini adolescents aged 12 to 17 years reported a prevalence of Obesity of 21 percent and 35 percent for boys and girls respectively. Also, Gargari, et al. [26] in Iran in 2004 reported prevalence rates of Obesity as 3.6 percent among high school adolescent girls in Tabriz. The higher prevalence seen in most of these high-income countries could be due to exposure to high calorie diets and engagement in sedentary lifestyles.
This present study found a higher prevalence rate for Overweight and Obesity in female than male adolescents, which is similar to the findings in previous studies among adolescents in low- and middle- income countries [18,27,28]. This may be related to the rapid growth that occurs during puberty which is earlier and more pronounced in females [29]. In addition, it has been suggested that the female hormone oestrogen inhibits thyroid hormone thereby reducing basal metabolism and encourage fat storage [30]. Oestrogen also modulates the hypothalamic hormones through the activity of leptin thus stimulating appetite and resulting in positive energy balance [30]. Furthermore, in certain cultures, fatness is perceived as a sign of happiness and affluence and fatness allows them to engage in sport activities that need strength and also makes one look respectable [31]. On the contrary, a study reported higher rate of Overweight and Obesity among boys than girls [12].
In this study, the highest proportion of obese subjects was from social class I, although this was not statistically significant. However, some studies found a direct relationship between parental socioeconomic status and Obesity [11,32]. While others found an inverse relationship between parental socioeconomic status and Obesity [33,34]. This inconsistency in the relationship between socioeconomic status and Obesity could be due to differences in populations, genetic variations, methodologies, sampling variation and the range of social classes in the populations studied [32]. Obesity is more common in the higher social classes because such families by virtue of their better social standing, can afford high calorie food that might be in excess for their children and also more likely to engage in sedentary lifestyles [35].
In this study, higher proportion of students attending private schools was found to be obese more than those in public schools. This was similar to the findings in Kenya where children attending private schools were 3.2 times more likely to be overweight and obese compared to those attending public schools [36]. While public schools in Kenya are funded by the government through the free primary education programme, private schools charge fees. It therefore follows that only parents who can afford the fees charged opt to enroll their children in private schools.
The numbers of meals, in-between-meals snacks, eating from fast food restaurants, consumption of fruits and vegetables have not been found to be associated with overweight and obesity in most studies [37]. This was also observed in the present study. Additionally, the quantities eaten and the fact that the subjects in this study also engage in some forms of exercise could explain why meal was not significantly associated with development of overweight and obesity. Also, Overweight and Obesity were not associated with alcohol consumption in this study as reported by Dupuy, et al. [38], whereas positive association was found in other studies [39,40]. The reason for the non-association of Overweight and Obesity with alcohol consumption in the index study could be due to the fact that almost 90 percent of the subjects reported no or rare intake of alcohol.
The effect of physical activity and sedentary behaviour was explored in this study and it was observed that more of the Overweight and obese subjects exercise less than their non- Overweight and non-obese counterparts. This finding was similar to the report by Janssen, et al. [37] in a study among children aged 11-16 year where physical exercise was found to be low in Overweight and obese participants but is contrary to the report by Manal, et al. [41]. It may be difficult to infer from this study whether this was a cause or effect relationship. Several studies have documented positive relationship between sedentary lifestyle and occurrence of overweight and obesity [15,24]. The positive relationship could be explained by the fact that less activities enhances fat accumulation thereby predisposing to Obesity [42]. On the other hand, high weight could hamper mobility and could also expose affected individuals to bullying hence less participation in physical exercise.
Relationship between waist-hip ratio and Overweight and Obesity was explored in this study. There was no significant difference in the mean waist-hip ratios of both sexes and among the different nutritional groups in this study. This is contrary to the findings in Ile-Ife where a higher mean for waist hip ratio in males was reported [43]. A study among Greek adolescents had hinted on the non-suitability of the use of WHR as indicator of obesity in adolescents because of the cut offs which are basically suitable in adults [44]. There is therefore a need for a large-scale study to determine the appropriate WHR cut offs in adolescents and its correlation with BMI.
Some researchers have checked for the independent predictive values of the factors that are associated with Overweight and Obesity using logistic regression model [45]. The findings are varied but generally; gender, private schools' attendance, lack of physical activity and intake of sweetened drinks have been reported as independent factors associated with Overweight and Obesity [34,37]. Some of these associations were seen in the present study with attendance of private school being independent associated factors with Obesity. It is possible that some of the significant factors in this study that were subsequently not independently associated with Overweight and Obesity exert their effects in the presence of other associated factors.
The limitation of this index study was the information on dietary pattern and sedentary lifestyle provided by the respondents were based on recall which may be source of bias, as it could not be verified.
In conclusion, the prevalence of Overweight and Obesity in this study were 4.1 percent and 1.3 percent respectively demonstrating a double burden disease co-existing with already established undernutrition. The main factor contributing to the rising Obesity were type of school attended and participation in physical activities. Therefore, physical education should be encouraged in all schools.
The authors appreciate the effort of Dr J.A.O Okeniyi, of the Department of Paediatrics and Child Health, Obafemi Awolowo University, Ile-Ife, Osun-State for proof reading of the paper.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
The authors declare that there are no conflicts of interest, financial or otherwise in the publication of this paper.
All the authors (Ibitoye B. Samuel, Olumuyiwa A. Alonge, Abiodun J. Kareem, Qasim O. Salau, Tolulope O. Jegede, Ifedayo O. Fasonranti, Korede O. Oluwatuyi, Emmanuel O. Babalola, Toluwalope Ejiyooye, Oluwadamilola E. Orotunde) were involved in the conception and design of the title, literature search, analysis and interpretation of the data, drafting of the article, revising the article critically and final approval of the version to be published.