To determine the effects of disease subtype, disease onset, and presence of anti-topoisomerase I antibodies (ATAs) on fertility and pregnancy outcomes in women with systemic sclerosis.
This study was conducted on 129 female patients from our scleroderma clinic, who were diagnosed according to the American College of Rheumatology (ACR)/European League Against Rheumatism (ACR/EULAR) classification criteria for systemic sclerosis (2013) and whose first symptoms had emerged before the age of 45 years. The patients' gynecological history was taken using a questionnaire, which included the marital status, history of infertility, pregnancy outcomes, and neonatal status during and after delivery.
Pregnancy occurred in 109 (84%) women (diffuse cutaneous systemic sclerosis, 48.8%; limited cutaneous systemic sclerosis, 52.2%). Based on the findings, 20 (15.5%) women were nulliparous. Overall, 229 pregnancies occurred before the disease onset and 49 pregnancies after the disease onset. Spontaneous abortion was reported more frequently in pregnancies occurring after the disease onset, compared to those occurring before the disease (24.4% vs. 9.6%; P = 0.005). Successful pregnancy was reported in 67% of pregnancies after the disease onset and 83.3% of pregnancies before the disease onset (P = 0.01). The frequency of preterm delivery after and before the disease onset was 16.3% and 4.3%, respectively (P = 0.002). The results showed that 6% and 1% of very-low-birth-weight neonates were born after and before the disease onset, respectively (P = 0.01). The disease subtype and presence of ATAs were not significantly effective in the outcomes of pregnancies occurring after the disease onset.
The results of this study showed that pregnancy after the disease onset was successful in two-thirds of systemic sclerosis patients. In addition, pregnancies occurring after the disease onset increased the rate of preterm delivery, pregnancy loss, and very low birth weight. The disease subtype and ATA positivity had no significant effects on the pregnancy outcomes after the disease onset.
Anti-topoisomerase I, Disease subtypes, Pregnancy outcomes, Systemic sclerosis
Systemic sclerosis (SSc) is a chronic connective disease, which predominately affects women of childbearing age. The female-to-male ratio of this disease is 5:1 [1]. The mean age of disease onset is in the middle 40's, but in 50% of patients, the disease may develop earlier before the end of childbearing age [2]. These patients and their physicians (e.g., rheumatologists, gynecologists, and neonatologists) are concerned about fertility, abortion, preterm delivery, low birth weight of newborns, and neonate's living status.
Early reports about SSc patients have suggested the negative impact of this disease on fertility and pregnancy outcomes, such as spontaneous abortion, prematurity, and low birth weight [2-7]. In recent studies, the rates of fertility and early pregnancy loss (miscarriage) in SSc patients are comparable to the general population, whereas premature delivery is more common than the normal population [1,8]. Many retrospective studies on SSc have used questionnaires for data collection [3,5,9-13]. In some studies, pregnancy outcomes were evaluated before the onset of SSc, while some studies focused on the outcomes after the disease onset, and some explored the outcomes of both pregnancy and disease [9,11]. The results of these studies may represent the proportion of pregnancy outcomes (as numerator) in all pregnancies (as denominator) with SSc, or only to pregnant women.
Although some studies have compared pregnancy outcomes in the two subtypes of SSc, the impact of anti-topoisomerase antibody (ATA) positivity has not been evaluated (1). It is worth mentioning that all published studies on the pregnancy outcomes of SSc patients were conducted in countries with the largest and most powerful economies, including the United states, the United Kingdom, Italy, Brazil, the Netherlands, Australia, and Canada [1,8-10,12-14].
In this study, we aimed to describe the gynecological history of 129 SSc patients in different geographical areas (Asia and the Middle East). First, we considered the effects of disease onset, disease subtype, and ATA positivity on pregnancy outcomes. Second, we compared the similarities and differences of pregnancy outcomes in SSc women between the present study and previous research.
A total of 129 female patients, who were visited to our scleroderma clinic from July 2017 to September 2018 and whose first symptoms had emerged before the age of 45 years, were included in the study. The diagnosis of SSc was established according to the American College of Rheumatology (ACR)/European League Against Rheumatism (ACR/EULAR) classification criteria [15]. All demographic, clinical, and serological data were extracted from the scleroderma database in the rheumatology clinic.
The patients were classified into limited cutaneous (lcSSc) and diffuse cutaneous (dcSSc) subtypes, according to the LeRoy criteria [16]. The gynecological history of the subjects was obtained using a questionnaire, which included marital status, history of infertility, pregnancy outcomes, and neonatal status during and after delivery. The data related to pregnancy outcomes were subdivided into pregnancy before and after the disease onset. The pregnancy outcomes were evaluated according to the definitions presented in Figure 1.
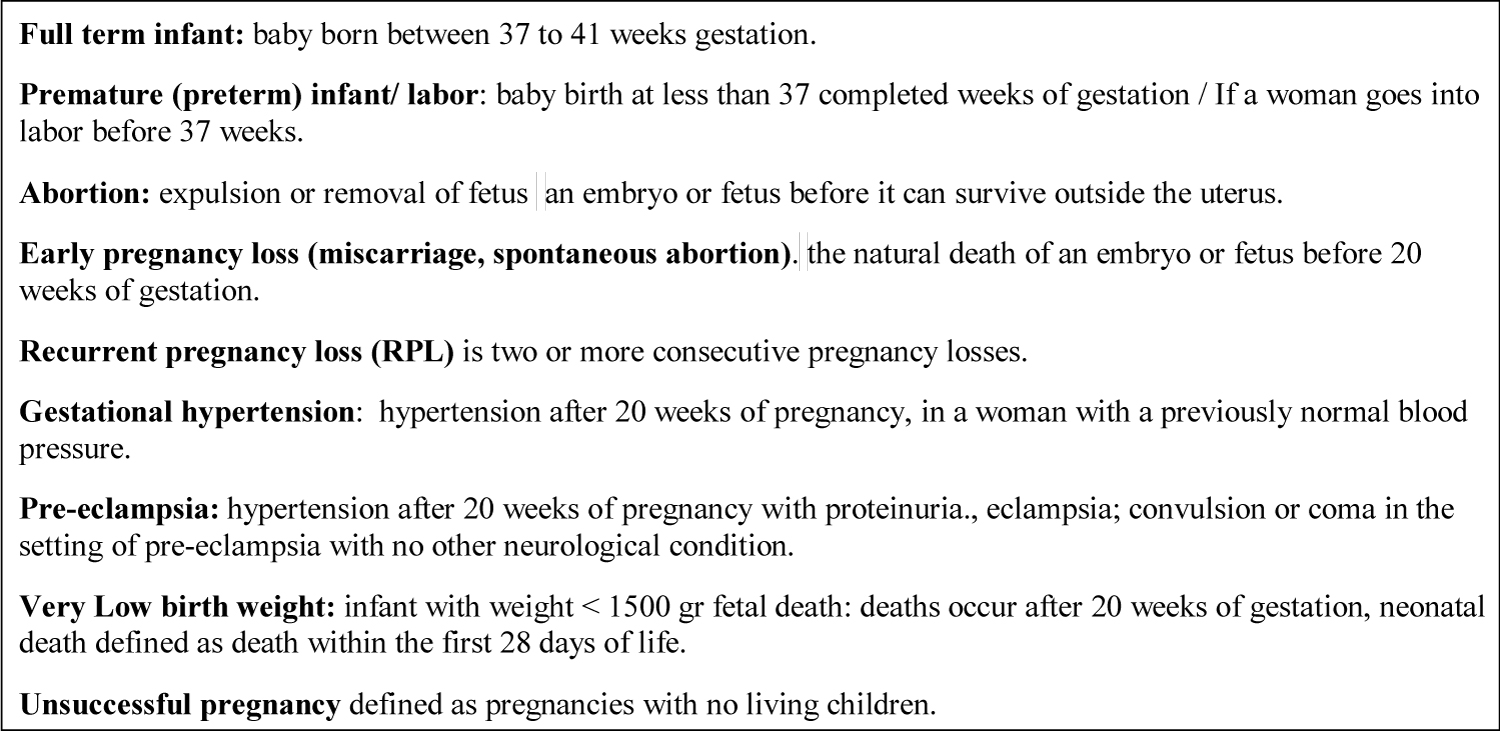 Figure 1: Definition of pregnancy outcome. View Figure 1
Figure 1: Definition of pregnancy outcome. View Figure 1
This study was approved by the Institutional Review Board of Iran University of Medical Sciences. Written informed consents were obtained from all subjects according to the Declaration of Helsinki.
Descriptive statistics were used to summarize the study population's characteristics and the frequency of variables. For continuous variables, t-test was used. Data are presented as mean and standard deviation (SD). For categorical variables, Chi-square test or Fisher's exact test was used. The odds ratio [OR] and 95% confidence interval [CI] were measured for evaluating cross-group associations in MedCalc statistical software.
The study population comprised 129 women. Pregnancy occurred in 109 (84%) women, including 52 (78.8%) women with dcSSc and 57 (90.5%) women with lcSSc. Table 1 summarizes the basic and demographic data of the study population. Pregnancy was reported in only 18 women after the disease onset and in 71 women before the disease onset. Six (33.3%) women who had become pregnant after the disease onset were diagnosed with the dsSSc subtype, while 36 (50.7%) women who had become pregnant before the disease onset were diagnosed with dcSSc. Twenty (15.5%) patients were nulliparous (14 with dcSSc and six with lcSSc), 15 of whom were never married (12 with dcSSc and three with lcSSc). Seven women had problems carrying a pregnancy to term.
Table 1: Demographic and baseline data of 129 women with systemic sclerosis. View Table 1
Smoking was reported in two women with the experience of pregnancy and one non-gravid woman. The mean (± SD) age of women at the disease onset was 31.4 ± 8.78 years (31.83 ± 8.0 years in the dcSSc group and 30.21 ± 9.45 years in the lcSSc group; P < 0.05). Successful pregnancy, regardless of the disease onset, occurred in 102 (93.6%) women, while unsuccessful pregnancy was reported in seven (6.4%) women (two women with dcSSc and five women with lcSSc). Abortion (spontaneous or induced) was reported in 46 (16.5%) pregnancies, and the rate of early pregnancy loss (miscarriage or spontaneous abortion) was reported to be 12.2% per pregnancy. Also, ten women experienced recurrent pregnancy loss (RPL).
Six women were positive for ATAs, while three were negative for these antibodies. One woman with an unsuccessful pregnancy reported three RPLs. The fluorescent antinuclear antibody (FANA) was positive in 90.8% of the patients. ATAs were positive in the sera of 78 (68.4.2%) patients [48 (61.5%) patients with dcSSc and 30 (38.5%) patients with lcSSc; P = 0.001]. The anti-centromere antibodies (ACAs) were positive in 8.8% of the patients, all of whom had the lcSSc subtype.
Pregnancy: Comparison of pregnancy outcomes between the two disease subtypes and two groups of patients becoming pregnant before and after the disease onset is shown in Table 2. The total number of pregnancies was 278 (mean number of pregnancies: 2.55 per woman). The mean pregnancy rate was 2.36% in women with dcSSc and 2.71% in women with lcSSc.
Table 2: Pregnancy outcomes in 109 women according to disease subset and disease onset in systemic sclerosis. View Table 2
Pregnancy outcomes: Abortion: Abortion was significantly different between the dcSSc and lcSSc groups. Nine (17.3%) abortions were reported in women with the dcSSc subtype of disease and 23 (40.3%) abortions in women with the lcSSc subtypes of disease (OR: 0.30; 95% CI: 0.12-0.75, P = 0.01). There was no significant difference in terms of abortion rate according to the onset of disease. RPL was not significantly different between the lcSSc and dcSSc groups (P = 0.80) and had no significant relationship with the disease onset (P = 0.59).
The total number of abortions was 46 (16.5%) out of 278 pregnancies (11.4% in the dcSSc group vs. 20.6% in the lcSSc group) (OR: 0.49; 95% CI: 0.25-0.9, P = 0.04). Abortion was reported in 29% of pregnancies after the disease onset and 14% of pregnancies before the disease onset (OR: 2.46; 95% CI: 1.19-5.07, P = 0.001). Spontaneous abortion was more common in pregnancies after the disease onset (OR: 3.05; 95% CI: 1.39-6.69, P = 0.005). Of 227 deliveries, 108 were reported in the dcSSc group and 119 in the lcSSc group.
Twin pregnancy: There was only one twin pregnancy after the disease onset in a patient with lcSSc.
Term delivery: Full term delivery was less frequent in pregnancies after the disease onset, compared to those occurring before the disease onset (51.1% vs. 81.6%) (OR: 0.27; 95% CI: 0.14-0.53, P = 0.0001).
Preterm delivery: Preterm delivery was reported in 44% of women who had become pregnant after the disease onset and 12.6% of women who had become pregnant before the disease onset (OR: 5.51; 95% CI: 1.72-17.63, P = 0.004).
Stillbirth: There was no significant difference between the two groups of patients, and stillbirth had no significant association with the disease onset.
Unsuccessful pregnancy: Unsuccessful pregnancy occurred frequently in women who had become pregnant after the disease onset (33.3%), compared to those who had become pregnant before the disease (1.4%); (OR: 35.00; 95% CI: 3.86-317.08, P = 0.001).
Obstetric complications: There was an increasing trend in the prevalence of preeclampsia in pregnancies after the disease onset. No eclampsia was reported in this study.
Delivery mode: Vaginal delivery was reported in 65.1% of pregnancies before the disease onset and 34.6% of pregnancies after the disease onset (OR: 0.28; 95% CI: 0.15-0.54, P = 0.0001). Cesarean section (CS) deliveries were more prevalent after the disease onset. Overall, 48 out of 229 (20.9%) pregnancies before the disease onset were delivered through CS, and 18 out of 49 (36.7%) pregnancies after the disease onset were delivered through CS (OR: 2.18; 95% CI: 1.12-4.24, P = 0.02).
Neonatal outcomes: Live birth: Live births were less frequent in pregnancies after the disease onset, compared to those occurring before the disease onset (67% vs. 83.4%); (OR: 0.41; 95% CI: 0.20-0.81, P = 0.01).
Very low birth weight: The prevalence of very low birth weight was higher in newborns who were born after the disease onset, compared to those who were born before the disease onset (6.1% vs. 1%), and the difference was statistically significant (OR: 7.40; 95% CI: 1.20-45.55, P = 0.003). Neonatal death: The disease subtype and disease onset had no significant effects on the prevalence of neonatal death.
Among women who had become pregnant after the disease onset, 24 (36.4%) were positive for ATAs in the sera, while nine (30.0%) were negative for ATAs. The ATA positivity had no significant effect on pregnancy and its related complications after the disease onset (Table 3).
Table 3: Pregnancy outcomes in 129 women with systemic sclerosis after the disease onset according to ATA positivity. View Table 3
In this retrospective study, the disease subtype and ATA positivity had no significant effects on the pregnancy rate and outcomes. However, our findings showed that women who had become pregnant after the disease onset were more likely to experience early pregnancy loss (spontaneous abortion), preterm birth, unsuccessful pregnancy, and very low birth weight of the newborn, compared to those who had become pregnant before the disease onset. In consistence with previous studies, we found that 67% of pregnancies after the disease onset were successful [1,5,10]. Smoking was rare in our study population and could not be considered a contributing factor for preterm delivery.
We found that the risk of early pregnancy loss (miscarriage) was 28.5% after the disease onset. In previous studies, the rate of early pregnancy loss was between 12% and 15%, which is somewhat higher than the estimates in the general population (10%) [3,5,7,8,11-13,17,18]. In a previous study, the rate of pregnancy loss was 15% before and after the disease, without any significant difference [5]. Similar to two prospective studies, we found no significant relationship between the frequency of pregnancy loss and the disease subtype (limited vs. diffuse) [8,17].
We found that preterm birth had a higher prevalence in pregnancies occurring after the disease onset, compared to those occurring before the disease onset (16.3% vs. 4.3%). In a previous study, premature birth in SSc women had a significant association with the time of pregnancy. Preterm birth occurred in 8% of pregnancies before the disease onset (n = 409) and 15% of pregnancies after the disease onset (n = 89) [12]. Moreover, in the present study, the prevalence of fetal loss in pregnancies after the disease onset was 4.1%, and the disease subtype and time of pregnancy did not affect the occurrence of still birth. It should be noted that previous studies have used different definitions for fetal loss. Its prevalence ranges from 2% in the Italian Multicentric Study on Pregnancy in Systemic Sclerosis (IMPRESS) to 1-5% in studies by Steen, et al. [6,9,12,17]. However, smoking was rare among women and could not be considered a contributing factor for preterm delivery.
Our findings showed that 23.7% of newborns were delivered via CS. The World Health Organization (WHO) has recommended a CS rate of 10-15%, which can be effective in saving the maternal and neonatal lives if they have any medical indications. The rate of CS in the present study was six times higher than the WHO recommendation, which may be attributed to the inappropriate increase in the prevalence of CS in Iran [19]. In IMPRESS, CS constituted 51 out of 109 pregnancies (52% of total deliveries). We believe that two factors can explain the higher rate of CS in SSc women. First, there is a rising trend of CS around the world, including Iran [19,20]. Second, women with SSc may be considered as high-risk patients; therefore, they are suitable candidates for CS delivery.
The results of the present study showed that the prevalence of very low birth weight was significantly higher in pregnancies after the disease onset. However, the disease subtype and time of pregnancy had no significant effects on neonatal death. These findings were compared with the results of previous research [8,11]. In our study, ATA positivity and disease onset had no significant effects on the pregnancy success rate or pregnancy complications. Neonatal birth weight and neonatal death were not affected by ATA positivity of mothers. In this regard, Taraborelli, et al., in the IMPRESS study, suggested that ATA positivity might play a protective role against preterm delivery [9].
In this study, similar to most retrospective research, data collection was based on questionnaires, which is prone to memory bias. To overcome this limitation, in the design of the questionnaire, we did not include questions about factors which could not be recalled, such as the cause of preterm delivery, definite birth weight, and intrauterine growth retardation. Due to the low number of pregnancies after the disease onset, the prevalence of pregnancy outcomes was low; therefore, the effect of ATA positivity could not be examined in all pregnancy outcomes. Finally, we did not consider the effect of organ involvement on the pregnancy outcomes.
Our findings indicated that two-thirds of pregnancies were successful in SSc patients. Pregnancy after the disease onset was associated with the increased rate of preterm delivery, pregnancy loss, and very low birth weight. However, ATA positivity had no significant effects on the pregnancy outcomes. The discrepancy between our results and previous studies conducted in developed countries may be due to differences in healthcare provision and knowledge about the pregnancy outcomes of SSc patients among healthcare professionals and the general population. To improve the pregnancy outcomes, we suggest that pregnant women with SSc visit in tertiary centers for a close follow-up by an expert team of rheumatologists, obstetricians, and neonatologists, who are familiar with scleroderma.
The authors declare no conflict of interest.