Although the discordance in the disease activity scores based on 28 joints (DAS28) has been widely investigated, few data exist among black African (BA) populations. We aimed first to evaluate the correlation and second to assess the concordance between various DAS28 scores in the BA patients with rheumatoid arthritis (RA).
We conducted a multicenter cross-sectional study in adult patients who had RA from Guinea and Cameroon. These patients were diagnosed according to the 2010 ACR/EULAR criteria. Outcome measures were DAS28-ESR and various DAS28-CRP scores. Paired t-test, agreement kappa coefficient, spearman's correlation coefficient, Bland-Altman plots, and ROC curves were used to analyze different DAS28 scores.
Of 74 patients analyzed, 85% were female, mean age of these patients was 50 years, and median disease duration was 36 months (IQR: 12-90). Four DAS28 scores comparisons were performed. DAS28-ESR was on average higher than standard DAS28-CRP (Δ = 0.58, [95% CI: 0.45-0.71]; p < 0.0001) and DAS28-CRP without patient's global VAS assessment (Δ = 0.51 [0.46-0.75]; p < 0.0001). Correlation between DAS28 scores was moderate ranging from 0.6 to 0.82. Overall agreement was lower for the conventional DAS28-ESR (weighted kappa: Range, 37.3% to 55.3%) than Castrejon DAS28-CRP (72.6% to 87.1%). DAS28-CRP-3 has a higher predictive power to evaluate disease activity than DAS28-ESR-3 (AUC, 0.97 [0.95-1.00] vs. 0.80 [0.68-0.91], p = 0.0062).
The current study provides information on correlation and discrepancy between different disease activity scores in BA patients with RA, and suggests that these markers were not interchangeable.
Rheumatoid arthritis, Disease activity, Concordance, Correlation
RA: Rheumatoid Arthritis; DAS: Disease Activity Score; BA: Black Africans; ACR: American College of Rheumatology; EULAR: European League Against Rheumatology Classification Criteria; ESR: Erythrocyte Sedimentation Rate; CRP: C-Reactive Protein; TJC: 28 Tender Joint Count; SJC: 28 Swollen Joint Count; VAS: Visual Analog Scale, self-assessed patient global assessment of disease activity on a VAS of 0 to 100 mm; SD: Standard Deviation; IQR: Interquartile Range; CI: Confidence Interval
Rheumatoid arthritis (RA) is the most prevalent chronic inflammatory autoimmune rheumatism, which principally affects the synovial tissue of the small joints. Clinically, RA is characterized by the swelling, pain, and stiffness that lead to severe disability due to the progressive joints damage [1].
Although, the Disease Activity Score (DAS) is widely used to evaluate the pharmacological agent's effectiveness in clinical trials as well as to monitor disease activity in daily clinical practice, there is an emerging controversy on the optimal thresholds values to be used for patient's classification in remission [2-5]. Since the first validated version of the DAS which was derived from 28-joints counts (DAS28) for tenderness and swelling, erythrocyte sedimentation rate (ESR) and patients visual analogical scale on 100 mm (VAS) [6-8], several adaptations of the DAS8 score have been proposed in the literature [5,9-11]. These successive adaptations included the substitution of the ESR by the C-reactive protein (DAS28-CRP) [9], or the simple numerical addition of individual measures on their original scale (Simplified Disease Activity Index [SDAI]) [10], or the removal of the acute phase reactants (Clinical Disease Activity Index [CDAI]) [10], or the removing the patient visual analogical scale leading to three components in the DAS28 formula (DAS28-ESR-3 and DAS28-CRP-3) [11], or the consideration of a sole component (ESR and CRP), and finally the adjustment of the DAS28 score on age and gender [4].
The correlation and concordance between these different disease activity scores (DAS28-ESR and DAS28-CRP) have been widely examined in different populations around the world. Despite the strong correlation found in all studies except between of sole components, the concordance results are conflicting [4,11-17]. This disagreement results in the heterogeneity on medical decisions making and the difficulty of comparing studies with one another.
Moreover, the majority of these studies is conducted in Caucasian, Latin or Asian populations [4,11,12,14-17] with little data is available on Black populations, especially those about the epidemiology, clinical severity of RA, the socio-economic aspects as well as the genetic and/or environmental factors leading to the disease [13]. As age, gender and racial/ethnic influenced ESR and CRP levels, data on concordance and interchangeability of different DAS28 scores in Black Africans (BA) patients with RA are needed. In this study, we reported data on correlation and concordance of different DAS28 scores from two major centers in the management of patients with RA in Guinea, and Cameroon. We aimed first to evaluate the correlation and second to compare the concordance between different DAS28 scores in these countries.
This cross-sectional study was based on clinical data, stored as Excel electronic records, from consultation registry conducted from two major centers in the management of patients with RA in Guinea (Ignace Deen Hospital, Conakry), and Cameroon (Efoulan District Hospital, Yaoundé). These patients were diagnosed according to the 2010 American College of Rheumatology (ACR) [18] and European League against Rheumatology Classification Criteria (EULAR) [19]. Adult patients with RA, who had at least one record on both ESR and CRP were analyzed. The study was approved by the National Ethics Committee for Heath Research (NECHR) reattached to the Ministry of Health (Conakry, Guinea), and the Ethics Committee of the Efoulan District Hospital (Yaoundé, Cameroon).
The extracted sociodemographic and clinical data were age, gender, geographical location (Guinea and Cameroon), duration of symptoms at diagnosis, positivity of anticyclic citrullinated peptide antibodies (ACPA) and rheumatoid factor (RF), ESR, CRP, patient's global VAS (0-100), 28-tenders joints count (TJC), 28-swollen joints count (SJC), and the current medications including methotrexate.
Means (standard deviation; SD) or median (interquartile range; IQR), and frequencies (percentage) were used to describe parametric and non-parametric continuous, and categorical data respectively. A total of seven outcomes measures were calculated with the corresponding formula summarized in Table 1, yielding four comparisons from [A] to [D].
Table 1: Outcomes measures and comparison. View Table 1
Difference between two paired DAS28 scores was tested using the paired t-tests, and correlation between scores was assessed by the Spearman correlation coefficient. To evaluate the levels of agreement between DAS28 scores as a continuous outcome, Bland-Altman plots were applied, by plotting the difference of DAS28 scores (Y-axis) against the mean scores (X-axis) [20]. The measures were said to be interchangeable if most of the data were within the limits of agreement (mean ± 2SD). Because, the minimum value of different DAS28 scores was 3.6 in our sample, only the comparison between moderate and higher disease activity was done according to the conventional DAS28-ESR cut-off (high: > 5.1, moderate ≤ 5.1) [19,21], and those suggested by Castrejon [2] (high: > 4.9, moderate ≤ 4.9). Then, we used the receiver-operating characteristic (ROC) applying the Youden's index method [22] to assess the optimal cutoffs points of the various DAS28-CRP measures that correspond to the conventional DAS28-ESR of 5.1 and to the Castrejon DAS28-CRP of 4.9. Performance measures including the sensitivity, specificity, positive and negative predictive values (PV), and area under curves (AUC, 95% CI) were estimated at this optimal threshold. Finally, the concordance for a higher disease activity between different DAS28-CRP scores using the optimal cut-off estimated in this study and those with conventional DAS28-ESR and Castrejon DAS28-CRP were assessed by the weighted kappa coefficient and their respective confidence interval. All data analyses were done in R (version 3.5.1). Significance was defined as a p-value less than 0.05, and all tests were two-sided.
A total of 74 patients with RA were analyzed (Table 2), among them 64 (86.5%) patients from Guinea, and 10 (13.5%) patients from Cameroon. The mean age of these patients was 50 years, 85% were female, with a median disease duration of 36 months (IQR: 12-90). Seventy nine percent of our patients (51/65) were seropositive for rheumatoid factor (RF) and 82% (31/38) were positive for the ACPA. All patients were under methotrexate. The laboratory characteristics were shown in Table 2.
Table 2: Patients characteristics at baseline and disease scores comparison. View Table 2
Data for DAS28 scores comparisons using the paired t-tests given in Table 2 showed a significantly higher DAS28-ESR mean score compared to the mean DAS28-CRP both for standard scores (DAS28-ESR and DAS28-CRP, Δ = 0.58, [95% confidence interval: 0.45-0.71]; p < 0.0001) and those using three variables (DAS28-ESR-3 and DAS28-CRP-3, Δ = 0.51 [0.46-0.75]; p < 0.0001). Nevertheless, the standard mean DAS28-ESR was comparable to the mean adjusted DAS28-CRP scores derived from Tamhane and the current study data-specific score (Δ = -0.018 [-0.14-0.10]; p = 0.7563, Δ = 0 [-0.10-0.10]; p = 0.9992) respectively. In addition, the comparison between the mean of DAS28-CRP scores from this current study data-specific and Tamhane showed no significant differences (Δ = -0.018 [-0.08-0.04]; p = 0.5341).
Figure 1 showed the scatter graphs for correlation according gender (blue for men and yellow for women) and in opposite the Bland-Altman plots for level of agreement corresponding to the same DAS28 scores comparisons. We found a significantly moderate correlation ranging from r = 0.6 to 0.82; p < 0.0001, with some disagreement as shown by the scatter diagram of the equality line. In addition, the Bland-Altman plots (Figure 1) showed that the differences between DAS28 scores in comparisons [A] and [B] were positive for 86% of patients. The corresponding rates of patients in comparisons [C] and [D] were 45%, and 55% respectively. The observed positive mean difference (bias) display in Table S1, suggested that the DAS28-ESR method yielded a higher disease activity than the measured simultaneously with the DAS28-CRP method. The limit of agreement varied across comparisons (Table S1), the observed bias was 0.58 (0.45-0.71), and the limits of agreement were between -0.55 (-0.77, -0.32) and 1.71 (1.48, 1.94) in comparisons [A] (DAS28-ESR and DAS28-CRP). The percentages of error between comparisons were higher than 30% except in comparison [A] (Figure S1).
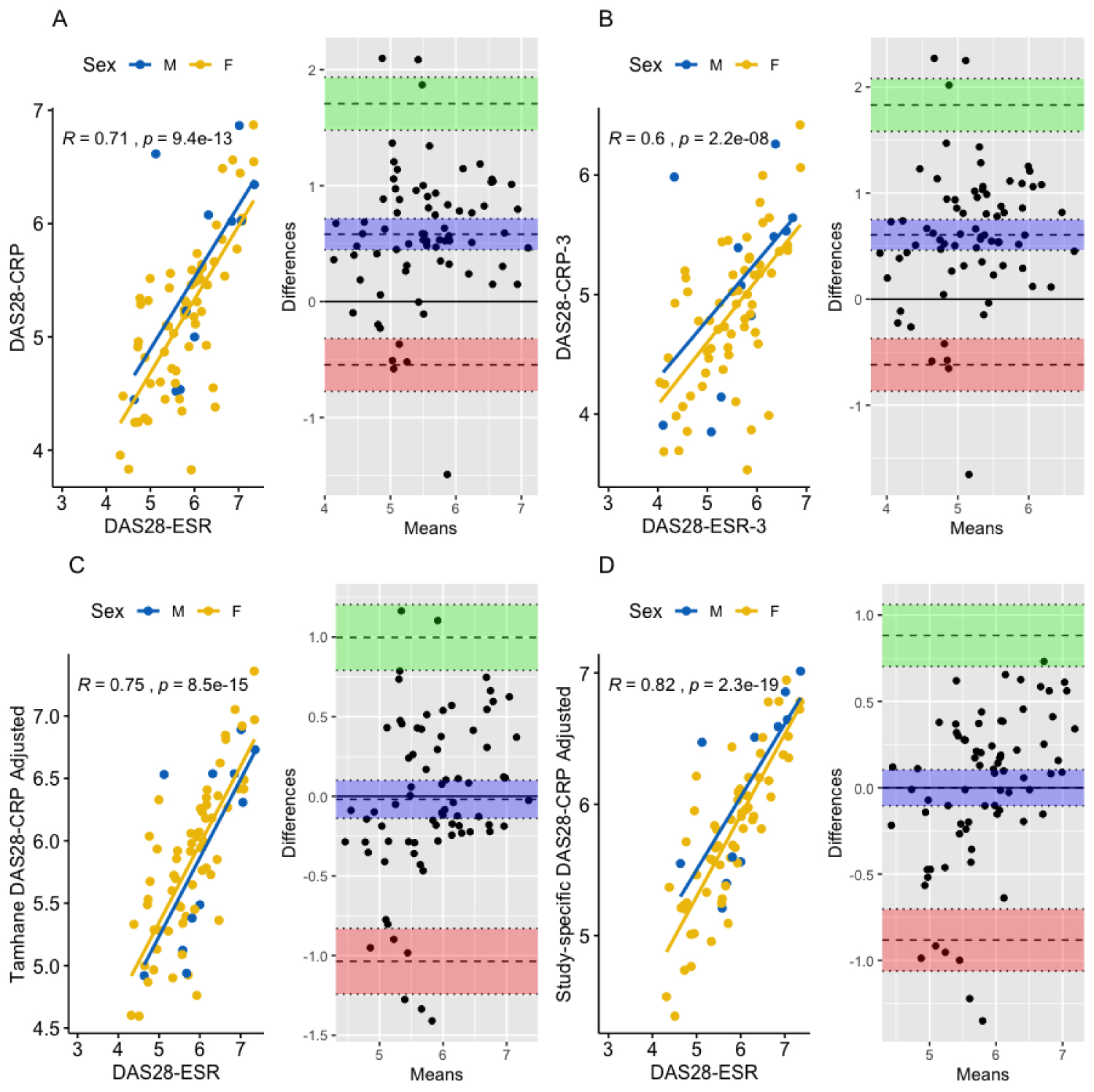 Figure 1: Correlation and the corresponding agreement using the Bland-Altman plots for various activity disease scores.
Figure 1: Correlation and the corresponding agreement using the Bland-Altman plots for various activity disease scores.
DAS: Disease Activity Score; ESR: Erythrocyte Sedimentation Rate; CRP: C-Reactive Protein; Comparison A: DAS28-ESR and DAS28-CRP (standard); B: DAS28-ESR-3 and DAS28-CRP-3 (excluding the patient's global VAS assessment); C: DAS28-ESR and Tamhane, et al. DAS28-CRP (adjusted for age and sex), D: DAS28-ESR and current study data-specific DAS28-CRP (adjusted for age and sex); For each comparison, correlation was display according to the gender (blue for female and yellow for men) in left panel, and the Bland-Altman plots in right panel: Dashed lines represent the bias (purple), lower (pink) and upper (green) limits of agreement, and dotted represent their corresponding confidence interval; difference was the one between DAS28-ESR and DAS28-CRP scores, and means was the mean of the corresponding DAS28-ESR and DAS28-CRP scores.
View Figure 1
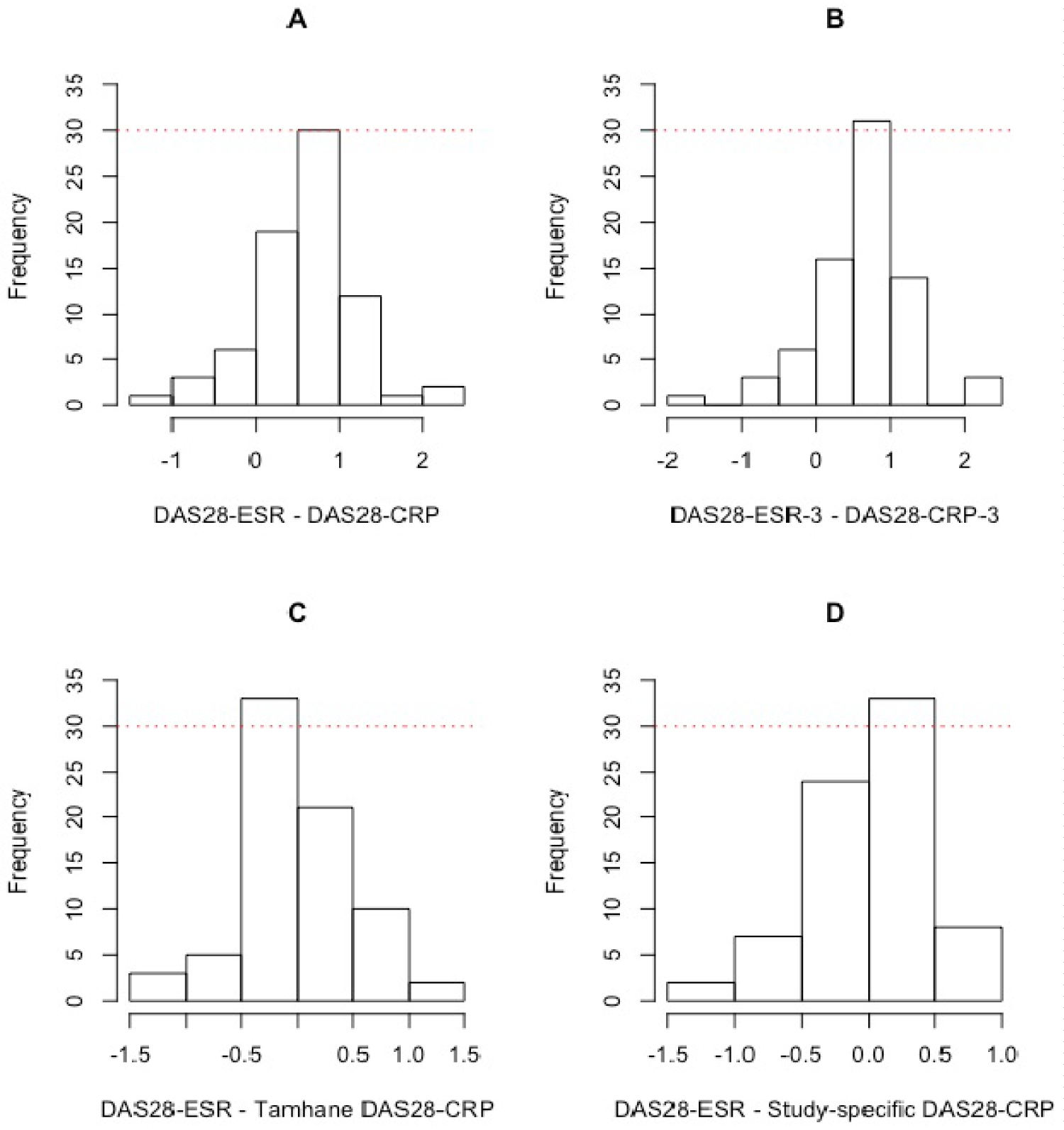 Figure S1: Histogram of the difference scores; the differences in scores were distributed normally around the bias (0.58, 0.61, -0.02, and 0.00).
Figure S1: Histogram of the difference scores; the differences in scores were distributed normally around the bias (0.58, 0.61, -0.02, and 0.00).
DAS: Disease Activity Score; ESR: Erythrocyte Sedimentation Rate; CRP: C-Reactive Protein.
View Figure S1
Table S1: Agreement between disease activity scores in 74 black African patients with RA. Bias, lower and upper limits of agreement are shown. View Table S1
The best performance measures to identify patients with a higher disease activity were observed using the cut-off proposed by Castrejon, et al. (Table 3). The best trade-off DAS28-CRP value from the current study data-specific corresponding to DAS28-ESR value of 5.1 (conventional) and to DAS28-CRP value of 4.9 (Castrejon) was 5.6. At each level of disease activity (Table 3 and Appendix, Figure S2), the estimated performance measures based on this optimal trade-off were greater for DAS28-CRP than for DAS28-ESR (84.5% vs. 88.2% for sensitivity, 81.3% vs. 87% for specificity, 94.2% vs. 93.8% for positive predictive values, and 59.1% vs. 76.9% for negative predictive values), with no observed difference between their predictive power (AUC, 0.87 [95% CI, 0.76-0.97] vs. 0.92 [0.86-0.99], p = 0.3645). Nevertheless, the predictive power was significantly higher for DAS28-CRP than DAS28-ESR when DAS28-CRP from Tamhane (p = 0.0034) or DAS28-CRP without patient's global VAS assessment (p = 0.0062) were applied. In addition, we found a higher predictive power for Tamhane modified DAS28-CRP than our data-specific modified DAS28-CRP (p = 0.0231).
 Figure S2: Receiver Operating Characteristic (ROC) curves for various activity disease scores according to the conventional threshold (DAS28-ESR ≤ 5.1) and Castrejon threshold (DAS28-CRP ≤ 4.9) for moderate disease activity.
Figure S2: Receiver Operating Characteristic (ROC) curves for various activity disease scores according to the conventional threshold (DAS28-ESR ≤ 5.1) and Castrejon threshold (DAS28-CRP ≤ 4.9) for moderate disease activity.
DAS: Disease Activity Score; ESR: Erythrocyte Sedimentation Rate; CRP: C-Reactive Protein; DAS28-CRP (orange line), DAS28-CRP-3 (olive line), current study data-specific DAS28-CRP adjusted for age and sex (green line), and DAS28-CRP Tamhane, et al. adjusted for age and sex (purple).
View Figure S2
Table 3: Performance of disease activity score (DAS28-CRP, DAS28-CRP-3, Tamhane, et al. DAS28-CRP, and the current study-specific DAS28-CRP) according to the conventional threshold (DAS28-ESR ≤ 5.1) and Castrejon threshold (DAS28-CRP ≤ 4.9) for moderate disease activity. View Table 3
Using these estimated optimal cut-offs for each different DAS28-CRP score (Table 3), we evaluated the concordance for a higher disease activity over the conventional DAS28-ESR and Castrejon DAS28-CRP thresholds applying the weighted kappa coefficient. Overall, the agreement was good for the Castrejon DAS28-CRP thresholds (weighted kappa range, 72.6% to 87.1%), and lower for the conventional DAS28-ESR thresholds (37.3% to 55.3%) (Table 4). When compared to the conventional DAS28-ESR, disagreement with the current study data-specific DAS28-CRP was observed in 13 (17.7%) patients, in whom DAS28-ESR overestimated disease activity in 10 (77%) cases. Between DAS28-ESR and DAS28-CRP, 19 discrepant cases were observed in whom 79% (15 patients) were overestimated by DAS28-ESR. The corresponding proportions of disease activity overestimated by DAS28-ESR were 67% (10/15) and 86% (18/21) respectively for comparisons [B] and [C]. Similarly, the rates of a higher disease activity overestimated by the proposed Castrejon DAS28-CRP thresholds when compared to the DAS28-CRP-3, the modified DAS28-CRP from Tamhane and the current study data-specific were 75% (8/8), 25% (1/4), and 67% (6/9) respectively.
Table 4: Weighted agreement kappa coefficient between different disease activity scores as assessed by the DAS28-CRP, DAS28-CRP-3, Tamhane, et al. DAS28-CRP, and current study-specific DAS28-CRP according to the conventional threshold (DAS28-ESR ≤ 5.1) and Castrejon threshold (DAS28-CRP ≤ 4.9) for moderate disease activity. View Table 4
In this cross-sectional multicenter study, the data of BA patients with a higher rheumatic arthritis activity were analyzed. Despite the moderate positive correlation between DAS28-ESR and DAS28-CRP, we observed that, DAS28-ESR was significantly higher than DAS28-CRP, and their agreement was lower suggesting that these two markers were not interchangeable. Nevertheless, the agreement was good when the Castrejon [2] DAS28-CRP thresholds were used.
Unlike the previous published studies [14-17], we found a moderate correlation between DAS28-ESR and DAS28-CRP whatever the type of formula used to compute the disease activity score. This result has no impact on the interchangeability between ESR and CRP since the strong correlation is not synonymous with concordance. In 44.6% of our patients, the difference between DAS28-ESR and DAS28-CRP was greater than measurement error (> 0.6) that was lower to those reported by Tamhane (50.8%) [13] and Restrepo-Correa (58%) [16]. The corresponding value for comparison between DAS28-ESR-3 vs. DAS28-CRP-3 was 50% which was comparable to those found by Tamhane (47.2%) [13].
As reported previously, DAS28-ESR tends to overestimate the disease activity when compared with DAS28-CRP measures [23]. We found that in 79% of cases, DAS28-ESR overestimated the disease activity when compared to DAS28-CRP, which was comparable to discrepant rates from Colombian study (76%) [16], and lower to those reported by Tamhane (93%) [13]. Additionally, our estimated weighted kappa for agreement was 0.39, which was comparable to those reported in Black African American patients (k = 40.5). Discordance between literature results may be explained by genetic background, study follow-up, patient's characteristic, and health care systems.
To overcome this discrepancy between DAS28-ESR and DAS28-CRP, many authors suggested a new threshold searching across different populations and areas. Therefore, we examined the predictive power for various DAS28-CRP measures on conventional DAS28-ESR threshold of 5.1 [21] and Castrejon threshold of 4.9 [2] to well classify patients in moderate or higher disease activity. The best trade-off DAS28-CRP value from the current study corresponding to DAS28-ESR value of 5.1 (conventional) was 5.6, which was higher to the reported value in Spain (4.35) [2]. In contrast, the sensitivity (93% vs. 85%) and specificity (96% vs. 81%) were lower in our study. In addition, except for the current study data-specific DAS28-CRP, we found a higher predictive power for DAS28-CRP than DAS28-ESR especially when DAS28-CRP without patient's global VAS assessment and Tamhane [13] modified DAS28-CRP were used. These findings support the usefulness of CRP instead of ESR to evaluate disease activity in RA, because CRP is a direct measurement marker of inflammation, more sensitive to change in inflammation, and easy to standardize in a laboratory [24,25].
To the best of our knowledge, this is the first study to assess correlation and concordance between different diseases activities scores in Black African patients treated for rheumatic disease from Guinea and Cameroon. Despite the use of the ACR/EULAR criteria [18,19] to assess disease activity and adapted statistical methods, the current study has a number of limitations. First, compared with the previous studies, our sample was too small which consisted of patients with long-term disease duration at inclusion, making it impossible to show the concordance between remission and low disease activity, which is more important when treat-to-target approach is considered. Second, we not able to assess influence of ethnicity or race on ESR, CRP or disease activity score, because these data were not recorded. Third, the current findings were not able to be generalizable in BA patients with RA possibly due to the population selection bias, since the study centers are not referral centers for PR management.
In conclusion, the current study provides information on correlation and concordance between different disease activity scores in BA patients with RA. Moderate correlation and major discrepancy found between DAS28-ESR and DAS28-CRP, suggests that these two markers were not interchangeable. Nevertheless, future large prospective multisite cohort studies are needed to validate thresholds for DAS28-ESR and DAS28-CRP in BA patients with RA to better adopt medical decisions.
We declare no competing interest in relation with this work.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.