Glioblastoma scalp dissemination is uncommon. Infiltration may occur through the craniotomy, suggesting diffusion from the surgical site as the most likely mechanism. At Magnetic Resonance Imaging (MRI), features of the metastatic tissue resemble those of the primary tumor. We show multimodal MRI appearance of a glioblastoma disseminating to the scalp. The patient presented with a stiff, non-tender palpable mass within the extracranial soft tissues, five months after surgery. Distinctive findings included low signal on T2 weighted images and relatively low diffusivity values suggesting hypercellularity, marked contrast enhancement, and increased perfusional blood volume, a marker of neovascularity.
MRI: Magnetic Resonance Imaging; WHO: World Health Organization; IDH: Isocitrate Dehydrogenase; MGMT: Methylguanine-DNA Methyltransferase
A 51-years-old, Caucasian man presented with partial faciobrachial seizure, with subsequent tonic-clonic generalization in April 2015. Imaging showed a left post-central intra-axial mass lesion. Biopsy results were lower grade astrocytoma (IDH1-2 wild-type, 1p19q non-codeleted, EGFR amplified, MGMT non-methylated). He underwent partial surgical resection due to tumor proximity to the sensorimotor cortex and cortico-spinal tract. Histopathological finding was a secondary progression to glioblastoma WHO grade IV. Radiotherapy (Intensity-Modulated Radiation Therapy) and chemotherapy (Temozolomide) were performed but, after 1 year, he underwent a second surgical excision for local relapse, followed by Bevacizumab treatment. This relapse was located in the left post-central gyrus and underwent to a gross total resection. At the clinical follow up performed five months later, the patient presented with a stiff palpable mass within the extracranial soft tissue at the level of the craniotomy. Multimodal MRI, including structural T2 and post-Gadolinium T1 weighted sequences, as well as diffusion and perfusion-weighted sequences, was performed. The scalp mass exhibited typical MRI characteristics found in glioblastoma tissue: low signal on T2-weighted images, marked and inhomogeneous contrast enhancement, relatively low diffusivity values suggesting hypercellularity and increased perfusional blood volume, a marker of neovascularity (Figure 1). There is not a post-mortem histology that could confirm the radiological diagnosis. Considered the poor general clinical condition of the patient, it was decided to perform palliative radiotherapy on the scalp lesion. The patient died few months after.
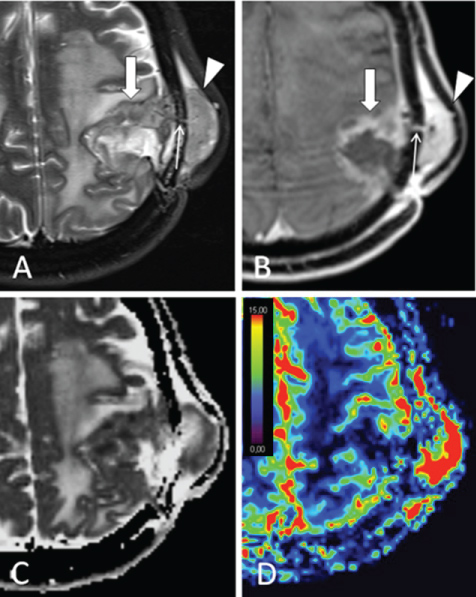 Figure 1: Fat-saturated T2w A) And post-gadolinium; B) Images show expansive tissue spreading from infiltrated brain parenchyma (large arrow) through the anterior craniotomy border (thin arrow) into the scalp (arrowheads). Apparent diffusion coefficient; C) And relative cerebral blood volume; D) Maps respectively show relatively low diffusivity and increased perfusion within the tissue. Relative cerebral blood volume scale values are in arbitrary units.
View Figure 1
Figure 1: Fat-saturated T2w A) And post-gadolinium; B) Images show expansive tissue spreading from infiltrated brain parenchyma (large arrow) through the anterior craniotomy border (thin arrow) into the scalp (arrowheads). Apparent diffusion coefficient; C) And relative cerebral blood volume; D) Maps respectively show relatively low diffusivity and increased perfusion within the tissue. Relative cerebral blood volume scale values are in arbitrary units.
View Figure 1
We showed a case where multimodal MRI could non-invasively demonstrate an extracranial dissemination of glioblastoma recurrence, and at the same time excluded other potential causes for scalp swelling, such as infection and/or dural defect. Converging MRI lesions features typical for a hyperperfused, hypercellular solid tissue, strongly supported diagnosis, and allowed to avoid biopsy in a patient with poor general clinical status.
Extracranial glioblastoma dissemination is rare [1-8]. Scalp dissemination may occur through direct extension or seeding from intracranial lesions through the craniotomy defect. Multimodal MRI may be helpful in the diagnosis of such lesions, because they exhibit features that resemble those of the primary tumour [5].
All of the authors certify that they will take public responsibility for the contents, have contributed substantially to the drafting, and have approved the final version. None of the authors has any conflicts of interest with the contents. All of the authors attest that all applicable subject protection guidelines and regulations were followed in the conduct of this research. The work has not been published and is not under consideration elsewhere and does not duplicate or overlap other published work.
No funding were received for this work from any of the following organizations: National Institutes of Health (NIH); Wellcome Trust; Howard Hughes Medical Institute (HHMI); and other(s). In this case the Data Protection Act does not apply because the patient is dead and relatives were not contactable. We guarantee complete patient anonymity in case description and MRI images. Ethical approval for this case report has been waived by our institution IRB.