'Talk and die' patients are a small number of patients who present with a mild head injury (Glasgow coma scale [GCS] 13-15) and then subsequently deteriorate and die from intracranial causes. We report the case of a 60-year-old man who had the first mild head injury, followed by chronic subdural hematoma and finally suffered from the high-energy second head injury and was ambulated to our hospital with a GCS of 15. He presented with severe headache and uncontrollable high blood pressure but he could talk. Computed tomographic scans showed a small brain contusion and traumatic subarachnoid hemorrhage (SAH) in the right temporal lobe, the left frontal lobe, and the anterior interhemispheric space around the pericallosal artery. 2 hours after injury, he suddenly vomited and then suffered from the status epileptics. Seizures were controlled after administration of consecutive 3 times intravenous 10 mg diazepam and followed by one shot thiopental 250 mg, then he was intubated, and ventilated. 4 hours after the injury, his GCS was 4 and bilateral pupils were moderately dilated and fixed. CT showed massive bifrontal and right temporal contusion hematoma and massive subarachnoid hemorrhage. He died two days after admission. One of his family members claimed malpractice and mentioned medicolegal issue but the author repeatedly explained that an unpredictable delayed intracranial hematoma and SAH had occurred in this patient. All family members understood it. In this paper, the authors investigated the possible factors affecting 'talk and die' pathophysiology and concluded that autonomic dysfunction and anatomical abnormality caused by the first head injury by the healing process of chronic subdural hematoma may be the possible causes of deterioration, and we would mentioned that 'talk and die' patients have potential medicolegal issue by inadequate explanation or informed consent on admission.
Mild traumatic brain injury, Talk and die, Medico legal issue
Reilly, et al. first introduced the term 'talk and die' in 1975, before the advent of computed tomographic (CT) scans to describe the small number of patients who present with a mild head injury (GCS 13-15) and then subsequently deteriorate and die from intracranial causes [1]. 'Talk and deteriorate' patients had been defined as patients who articulate recognizable words at some point after experiencing a head injury and then deteriorate to a GSC of ≤ 8 within 48 hr of the impact [2-5]. They represent a very small but important subgroup of patients with brain injury [6,7]. In majority of these patients, the cause of this deterioration is intracranial hematoma [2-7].
Several clinical practice guidelines (CPGs) have been issued [7-13]. They state that patients who have incurred a mild head injury and have a glasgow coma scale [GCS] score of 13-15 on their initial evaluation and imaging evidence of traumatic subarachnoid hemorrhage (SAH) and/or intraparenchymal contusion do not require a neurosurgical consultation or transfer to tertiary care center and can be safely discharged [7-13]. These studies have described the utility of CPGs for brain injury treatment but most of these CPGs have focused primarily on cost-effectiveness and the allocation of resources [7-13]. In fact, the number of such patients who received neurosurgical intervention is < 1% [7-14]. A prospective cohort study conducted in Canada that included consecutive adults who presented with a GCS score of 13-15 after head injury revealed that 8% of the patients had a clinically important brain injury and only 1% required neurosurgical intervention [15]. However, clinical studies have revealed that there is heterogenous pathophysiology among patients with GCS scores of 13-15, and detailed clinical pictures in case by case are obscure [16]. Highest incidence of 'talk and die' patients among a population with mild head injury was 2.6% [17]. The CPGs have recently been met with some skepticism - particularly within the neurosurgical community - because the promise of CPGs has not been matched by the reality, and those who oppose CPGs fear that such guidelines will hinder the art of medicine and limit physician and patient autonomy [18]. Traumatic brain injury is necessarily a neurosurgical pathology, and it has been opined that the exclusion of a neurosurgical consultation should be the exception rather than the rule [19].
The prediction and prevention of the 'talk and die' status is an old but still unsolved problem [20,21]. Here, we report a 'talk and die' patient who suffered a high-energy head trauma, and we discuss possible factors in his deterioration, e.g., a medical history of previous head trauma, subsequent chronic subdural hematoma, hyperperfusion by autonomic dysregulation, status epilepticus, hypertension, etc. and we extend the discussion to the potential medicolegal issues.
A 60-year-old Japanese man was brought to our hospital with a GCS of 15. He had fallen from a standing position, and the right parietal region was impacted. He had a 3-cm laceration of the scalp; it was treated with a stapler. CT scanning showed a thin right parietal subdural hematoma (Figure 1). He had a mild headache and nausea on admission, but they disappeared within a few days and he was discharged 7 days post-admission.
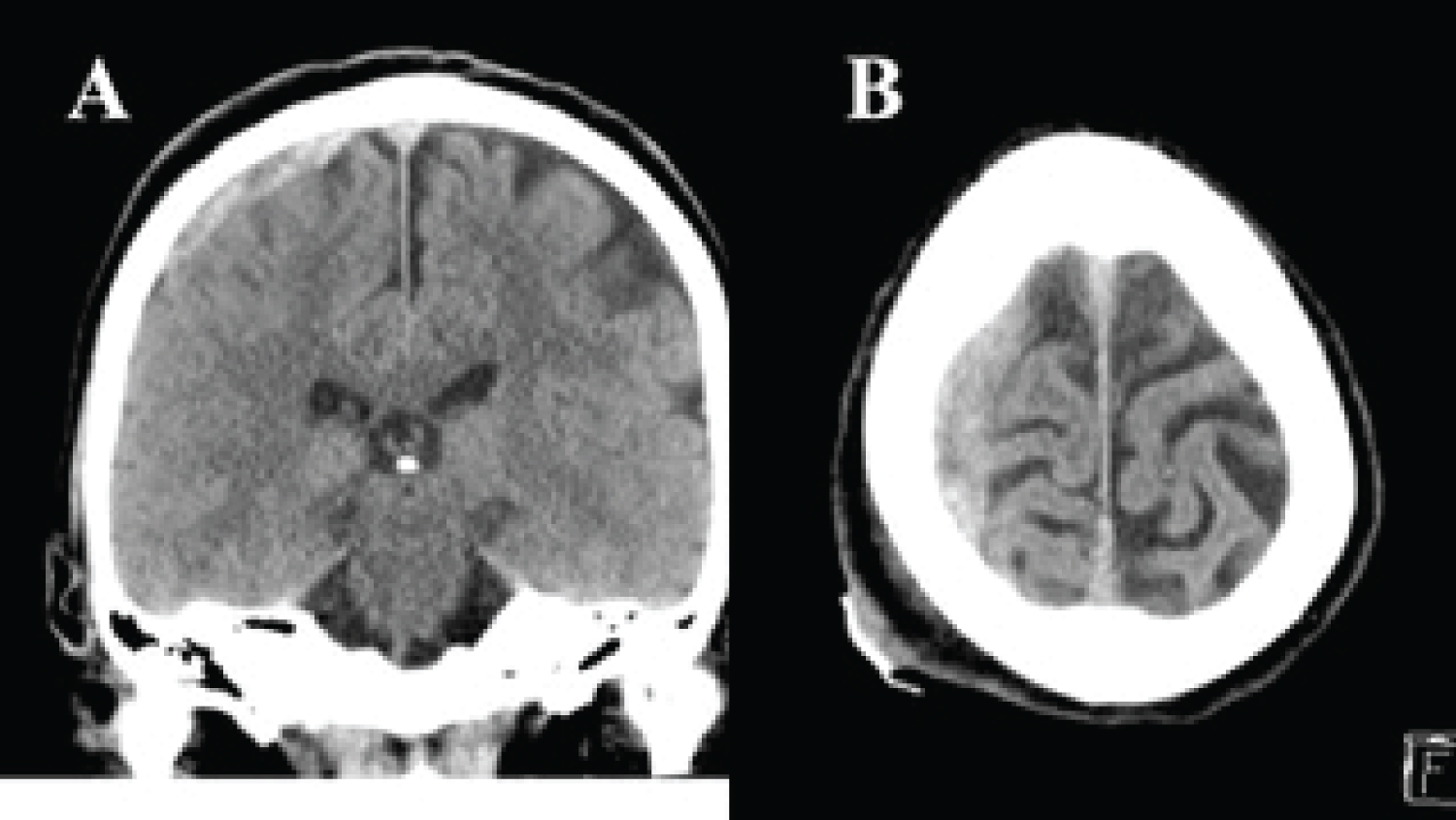 Figure 1: CT scan on the patient's first admission showing the thin right parietal subdural hematoma. View Figure 1
Figure 1: CT scan on the patient's first admission showing the thin right parietal subdural hematoma. View Figure 1
Two months later, the patient developed disorientation, dysarthria, and weak right hemiparesis and was admitted to our hospital. Under the diagnosis of a left chronic subdural hematoma (Figure 2), he underwent emergency single burr-hole drainage with the placement of a subdural drain for 24 hr under local anesthesia. He was discharged 7 days later with no symptoms.
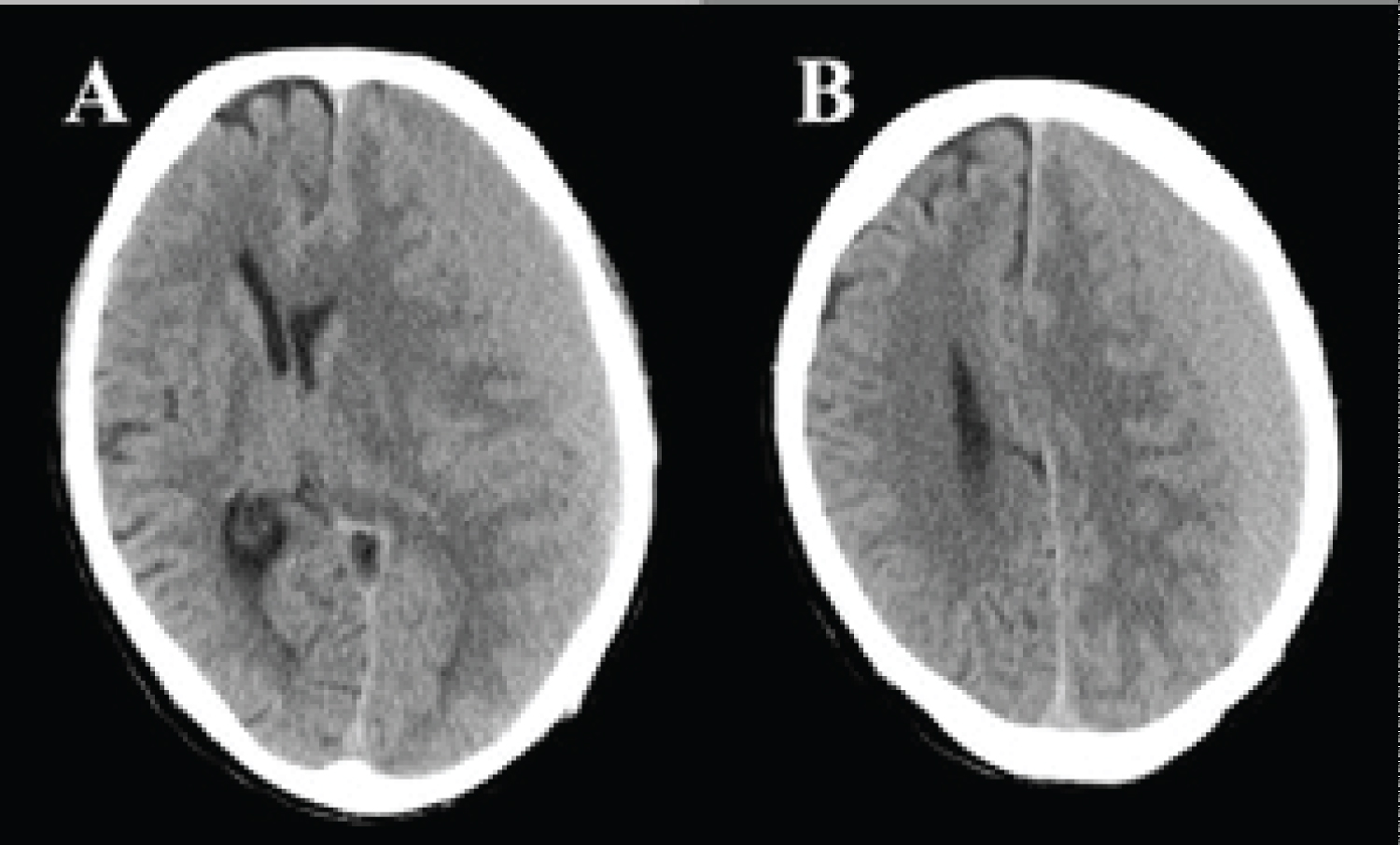 Figure 2: CT scan revealing the left chronic subdural hematoma with midline shift. View Figure 2
Figure 2: CT scan revealing the left chronic subdural hematoma with midline shift. View Figure 2
2 years later the patient was found by his wife lying on the concrete. He had fallen from on top of a 2.5-m-high carport while trimming a tree. He was able to talk. He was ambulated to our hospital with a GCS of 15. On admission, he presented with severe headache and nausea. He had a left parietooccipital subcutaneous hematoma. He had not been taken any antiplatelet or anticoagulation agent, and he had no medical history of hypertension. His vital signs were as follows: blood pressure, 218/126 mmHg; heart rate, 112 bpm; oxygen saturation, 96% on room air. The pupil diameters were 3.0 mm/3.0 mm with a prompt counter light reflex. Hematological and laboratory studies including a blood coagulation test revealed no abnormality with the exception of a white blood cell count of 14,000.
CT scans taken just 45 min after the head injury showed contusion or traumatic subarachnoid hemorrhage (SAH) in the right temporal tip, the left frontal tip (Figure 3A, Figure 3B, Figure 3C and Figure 3D), and SAH in the anterior interhemispheric space around the pericallosal artery (Figure 3E and Figure 3F). We had told the family that the patient could be discharged within a few weeks (possibly on foot) but that there was a very small possibility that the contusion hematomas might expand and hematoma evacuation would then be necessary; repeated CT would be taken 6 hr later regardless the patient's conscious level.
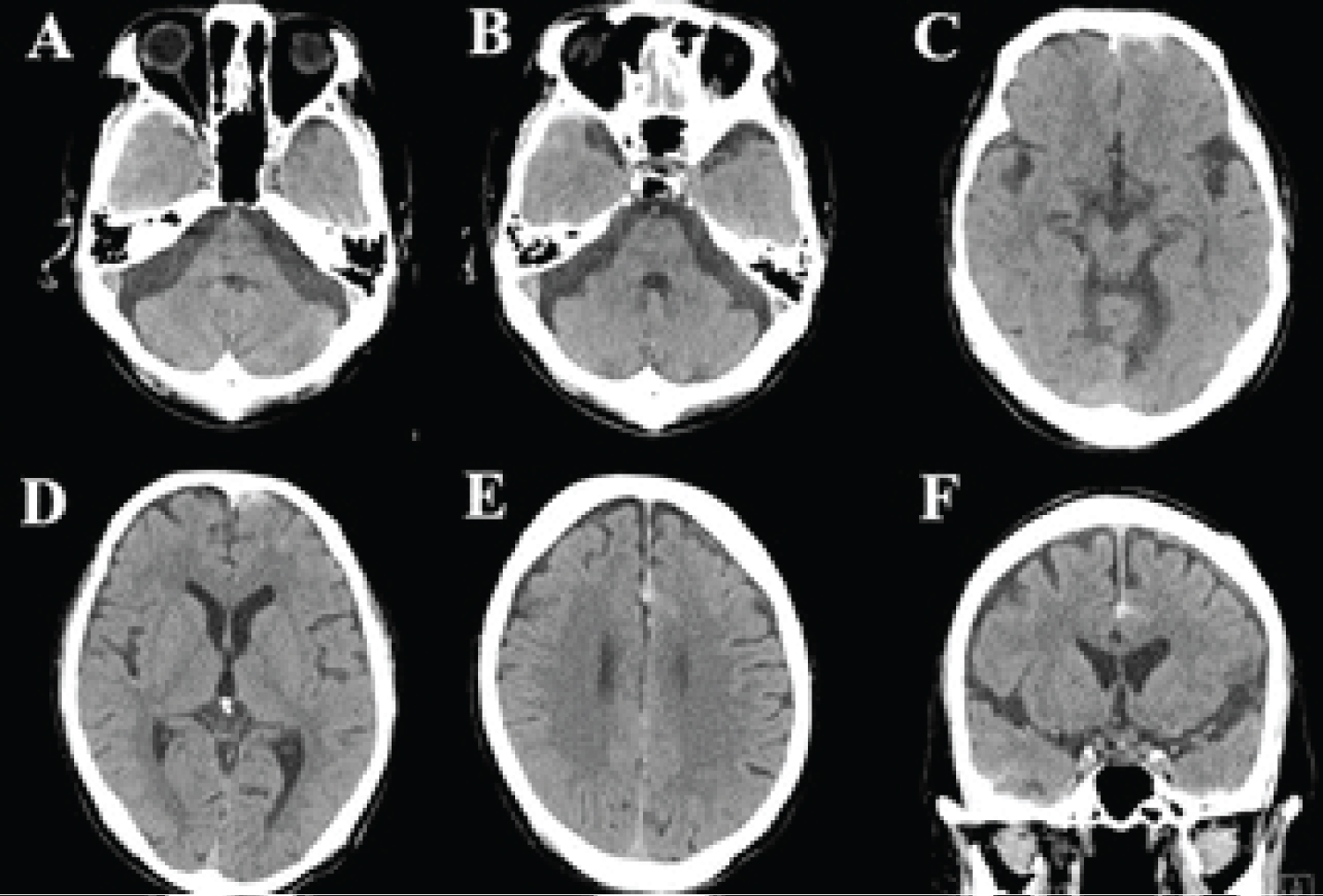 Figure 3: (A-D) CT scan at 45 min after the high-energy injury demonstrating contusions or traumatic subarachnoid hemorrhage (SAH) in the right temporal tip; (E,F) SAH in the anterior interhemispheric space around the pericallosal artery. View Figure 3
Figure 3: (A-D) CT scan at 45 min after the high-energy injury demonstrating contusions or traumatic subarachnoid hemorrhage (SAH) in the right temporal tip; (E,F) SAH in the anterior interhemispheric space around the pericallosal artery. View Figure 3
Intravenous nicardipine (> 30 mg/hr) was continuously administered to the patient in an attempt to decrease his blood pressure to < 140 mmHg, but his blood pressure continued to be > 180/100 mmHg. At 2 hr after admission, he suddenly vomited and then fell into status epilepticus. The seizures were refractory despite three consecutive intravenous administrations of 10-mg diazepam. A single injection of 250-mg thiopental was administered, and the patients was intubated and ventilated. His seizures were controlled with a continuous administration of thiopental (5 mg/kg/hr) under the continuous mandatory ventilation. Immediately after the seizure and the respiratory control, it was 2.5 hr after the patient's fall/head injury, a second CT examination revealed massive bifrontal and right temporal lobe hematomas and a massive SAH (Figure 4). These seemed to be multiple delayed contusion hematomas and an SAH due to an aneurysmal rupture or multiple arterial dissections. There was no indication of decompressive craniotomy and hematoma evacuation. The patient died next day. A family member of the patient claimed misdiagnosis or malpractice on our part because of the unexpected early death. After the coroner's post-mortem examination, the coroner examined the patient's CT images and concluded that a judicial autopsy was unnecessary. We asked the patient's family for permission to perform an autopsy, but they did not give their consent. They indicated a desire to take the matter up in court. We repeatedly explained to the family members that the delayed hematoma and SAH were unpredictable. We apologized for the inadequate informed consent in the patient's case, which did not mention the possibility of the 'talk and die' status on admission. The family withdrew the legal proceeding.
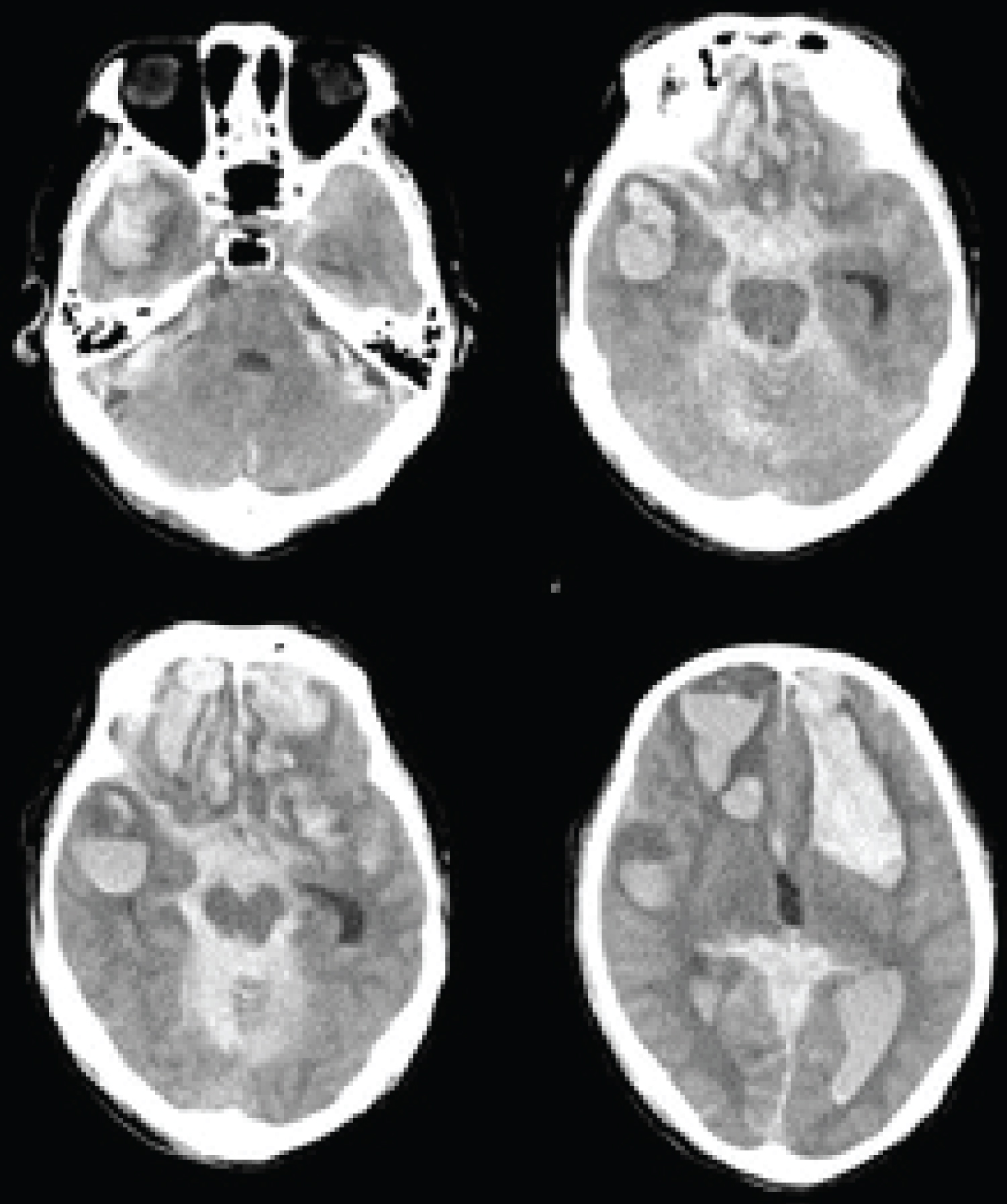 Figure 4: CT scan at 4 hr post-injury displaying multiple large contusion hematomas and the massive SAH. View Figure 4
Figure 4: CT scan at 4 hr post-injury displaying multiple large contusion hematomas and the massive SAH. View Figure 4
We speculate that after the patient's second and fatal head injury, increased intracranial pressure had developed due to hypertension and hypeyperfusion caused by dysregulation of cerebral blood flow due to the patient's high-energy injury and epilepsy. This case report describes several clinical pitfalls, i.e., the patient's high blood pressure could not be controlled, and a CT examination was not performed during the patient's status epilepticus and intubation.
'Mild head injury' is defined as head trauma involving a loss of consciousness or amnesia but with normal neurological findings on arrival at a hospital (i.e., GCS 15) [7-13]. High-risk mild head injuries are defined as high-energy injuries such as a fall from a height, a traffic accident, or an assault; trauma-related positive CT scans or the observation of a skull fracture on x-ray are important risk factors [16,22]. Another guideline defines high-energy injury as due mainly to falls from > 3 m [23]. The severity of the injury mechanism is described as an independent risk factor in many studies, and the early detection of intracranial lesions may be life-saving [24,25]. Barlow and Teasdale reported that clinicians involved in the management of head injuries regard the estimated prognosis soon after injury as having an important influence on subsequent management [26]. However, even with sophisticated clinical and radiological technologies, it is not possible to predict a patient's precise outcome based on the CT images taken a day after the injury, despite sufficiently early and appropriate management [27]. Delayed hematoma was described as a cause of disseminated intravascular clotting and fibrinolysis [27]. Studies presenting the 'talk and die' patients tend to be much older and/or taking anticoagulants and coagulopathy was reported to be the strongest prognostic predictor of poor outcome [20,27-29]. Recent meta-analysis including 21 studies estimated of the effect of patient' risk factors as follow: age, initial glasgow coma scale (GCS), type of injury, and anti-coagulation [30].
Early CT findings in patients with mild traumatic brain injury are heterogenous but usually consist of an isolated subdural hematoma, isolated SAH, isolated epidural hematoma, or intraparenchymal hematoma or contusion hematoma [10,12,21,29,30]. Combinations of these are often encountered, but an analysis of patients with such combinations revealed that among the cases of all-inclusive subtypes with a GCS score of 13-15, the isolated subdural hematoma group had worse outcomes [2,30]. A large proportion of acute traumatic intraparenchymal contusions and hematomas will progress; in addition, basal cistern absence, positive midline shift, and intraventricular hematoma or SAH on the initial head CT scan were each a strong predictor of early death [21,29,31].
The massive traumatic SAH in the present case may have been caused by a traumatic intracranial arterial dissection or pseudoaneurysm which are often observed proximally in the internal carotid artery at the supra-clinoidal portion [32,33]. A high-energy head injury that involves immediate shearing force might produce a pseudoaneurysm or arterial dissection [32,33], and a fatal rupture could occur a few hours later with the contribution of abnormal hypertension as in our patient's case.
In the present patient's case, during the healing process of the acute subdural hematoma and chronic subdural hematoma, an abnormal anatomical structure may have been formed in which pia matter and arachnoid and/or dura matter may be organized to be one-layer fibrous tissue that may adherent to the brain tissue. A large occipitoparietal impact accelerates the hard and light skull tissue, which moves readily and stops, whereas soft and heavy brain tissue does not readily move or stop; a contrecoup hematoma then develops due to cavitation theory-related negative pressure. In addition, based on the anatomical abnormality, a large hematoma might develop with the aid of hyperperfusion and hypertension. Immediately following a head injury, there are several metabolic, hemodynamic, structural, and electric changes that alter normal cerebral function [34]. Brain hyperemia appears to play a role in the deterioration of some head-injury patients [4,35]. With regard to cytokines, proinflammatory cytokines play an important role in regulating autonomic and cardiovascular function in hypertension and heart failure [36]. Peripherally administered proinflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin-1 beta (IL-1β) act on the brain to increase the blood pressure, heart rate, and sympathetic nerve activity [36,37]. In the present case, uncontrollable hypertension and a severe headache were observed; these symptoms might be due to hypeyperfusion and intracranial hypertension. The patient's status epilepticus devastated the intracranial condition, finally resulting in the fatal hemorrhage and massive SAH. Sympathetic hyperactivity occurs in a subgroup of patients after traumatic brain injury [38]. The rostral ventrolateral medulla (RVLM) is a key region for the activity of the sympathetic nervous system [38].
The potential medico-legal issues involved in the 'talk and die' status have very rarely been discussed [20]. A few papers in the area of neurosurgical practice describing how to obtain a fully informed consent have been published [39,40]. However, practicing neurosurgeons rarely have the time to explain every potential complication or unexpected event. Clinical practice guidelines (CPGs) can in theory provide a vehicle through which neurosurgeons can more efficiently integrate the most current evidence into patient management [18]. A major medical malpractice crisis is unfolding in the United States [40-43], although certain experts stress that most healthcare errors arise from the faulty systems in which proficient clinicians work, not from the clinicians themselves [41]. Jena, et al. analyzed malpractice data in the U.S. from 1991 through 2005 for all physicians with a nationwide client base (40,916 physicians and 233,738 physician-years of coverage) [42]. Of all departments, the proportion of physicians facing a claim each year was the highest in neurosurgery at 19.1% [42]. Although the 'talk and die' status is rare in patients who have experienced a mild head injury, it is very important to explain the possibility of this status to the family members of a patient with a head injury, even in cases of a mild head injury.
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.