According to guidelines of the brain trauma foundation and the congress of neurological surgeons for managing traumatic brain injury, surgical evacuation recommended for extradural haematoma with volume more than 30 cm3 regardless Glasgow coma scale (GCS) of patient. A case of asymptomatic extradural haematoma (volume 40.5 cm3) treated on regular clinico-radiological assessment (CRA) showed near complete resolution of extradural haematoma. This supports CRA as an ethically justified treatment approach in such cases. Simple CRA saves patient from complications related to anaesthesia and surgery, reduces workload on neurotrauma operation theatre and expenditure on health care. Further study needed in support.
Extradural haematoma, Traumatic brain injury, Clinico-radiological assessment
Traumatic brain injury (TBI) is a major health problem especially in the younger population and is said to be a silent epidemic. Incidence of extradural haematoma (EDH) is approximately 2% in TBI [1]. Timely surgical intervention in EDH gives excellent outcome. Results of surgery are very promising in EDH, out of all TBI. According to guidelines of the brain trauma foundation and the congress of neurological surgeons, for managing TBI surgical evacuation is recommended for EDH with volume more than 30 cm3, regardless Glasgow coma scale (GCS) of patient [2]. There are no definite criteria laid down till now, which can predict that a given asymptomatic EDH will resolve or increase.
An eighteen-year-old male sustained trauma due to a hit by a wooden rod. He was having continuous diffuse headache and vomited twice on day one only. There was no history of loss of consciousness or seizures. Patient consulted some doctor after injury who advised CT scan head which showed left fronto parietal acute EDH (Figure 1).
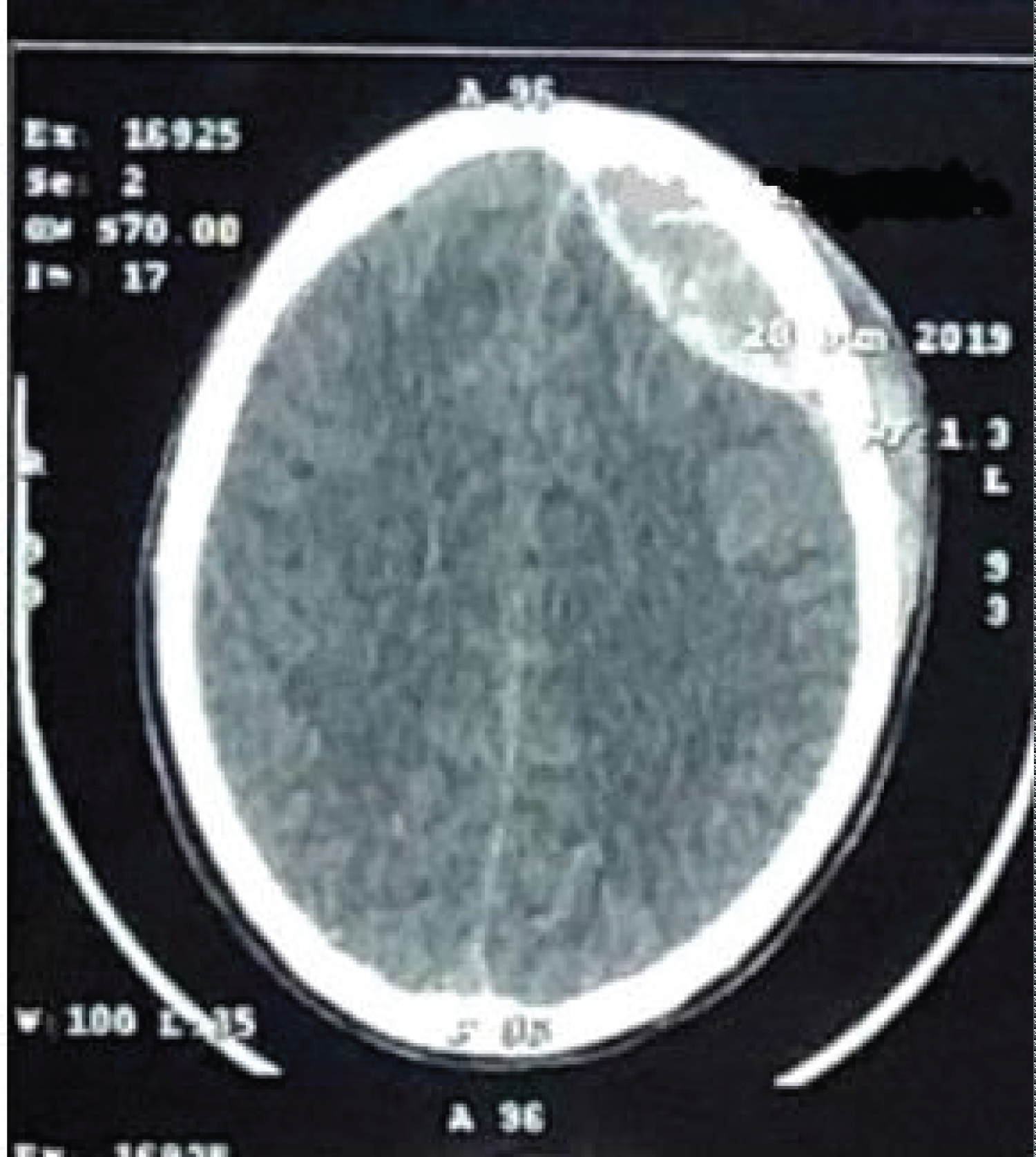 Figure 1: CT scan head (same day after injury) showing left frontoparietal extradural haematoma.
View Figure 1
Figure 1: CT scan head (same day after injury) showing left frontoparietal extradural haematoma.
View Figure 1
Patient came to our institute in Outpatient department (OPD) after one week with continuous diffuse headache. His neurological examination was normal and CT scan head (one week after trauma) shows sub-acute extradural haematoma (6 × 2.7 × 5, vol 40.5 cm3) (Figure 2).
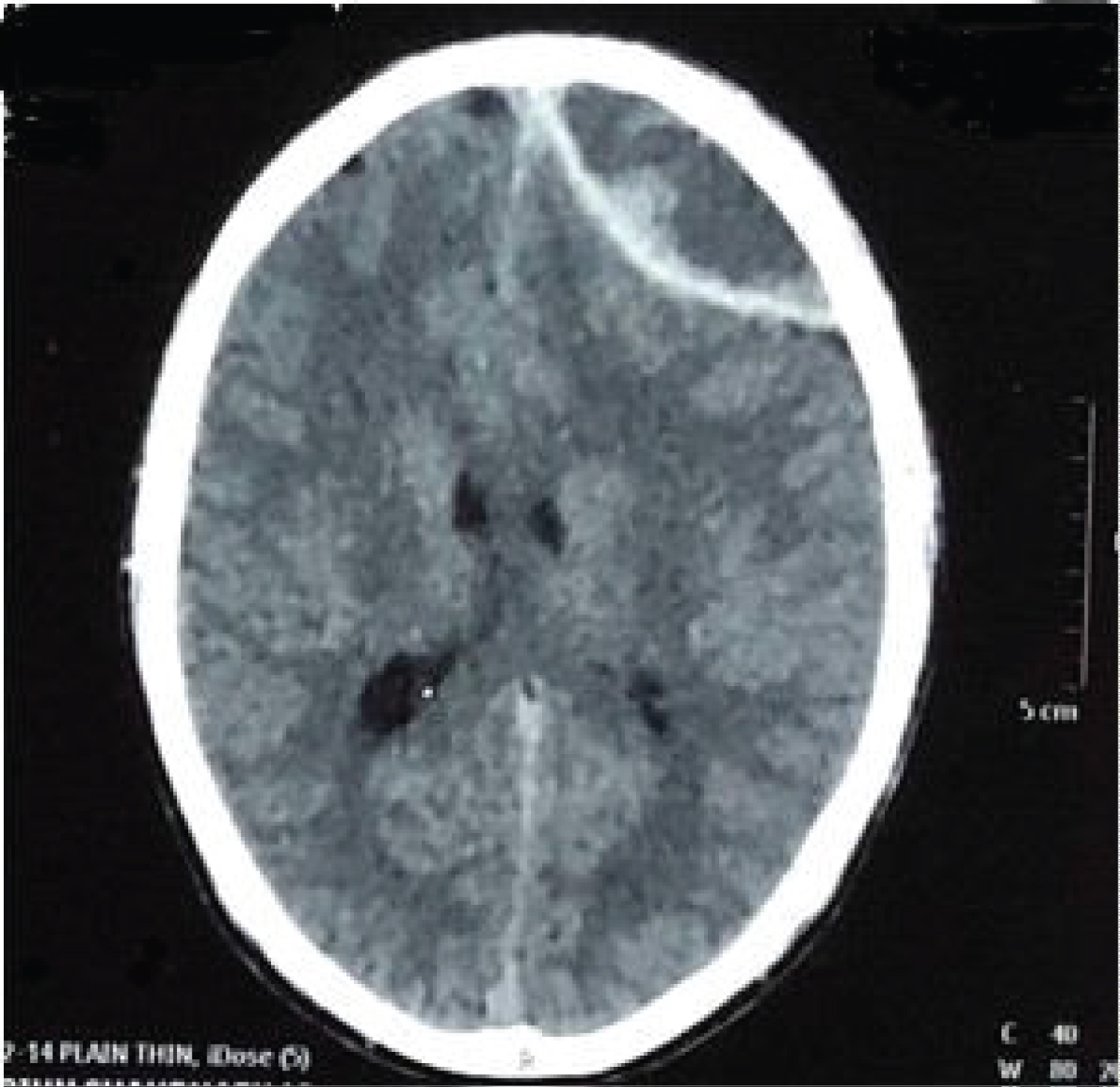 Figure 2: CT scan head (one week after injury) showing left frontoparietal extradural haematoma, volume 40.5 cm3 (6 × 2.7 × 5 cm3).
View Figure 2
Figure 2: CT scan head (one week after injury) showing left frontoparietal extradural haematoma, volume 40.5 cm3 (6 × 2.7 × 5 cm3).
View Figure 2
He was reluctant for opting any surgical intervention. Patient was advised to report urgently to hospital if develops any symptoms suggestive of raised intracranial pressure e.g., seizures, repeated vomiting, weakness of any limb, drowsiness, or unconsciousness. Patient was kept on symptomatic treatment in the form of analgesics and regular neurological assessment. Gradually his headache even regressed completely within a week. EDH was regressing in repeat CT scan head which were done thereafter, and CT scan head done after twelve weeks showed near complete resolution of left fronto parietal EDH (Figure 3).
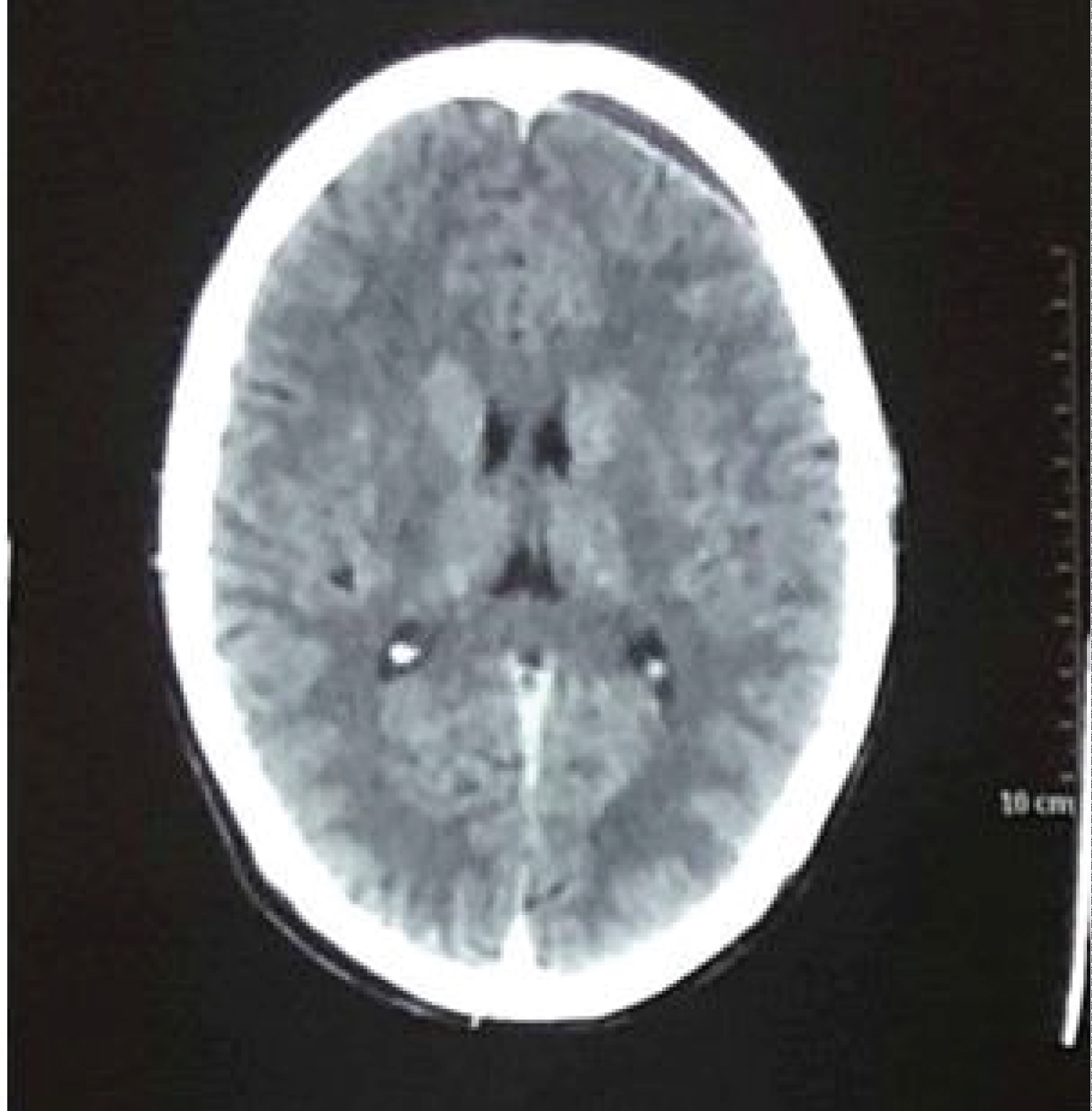 Figure 3: CT scan head (after 12 weeks), showing near complete resolution of left frontoparietal extradural haematoma. View Figure 3
Figure 3: CT scan head (after 12 weeks), showing near complete resolution of left frontoparietal extradural haematoma. View Figure 3
Results of surgical evacuation in EDH are very promising. It is the great responsibility of treating neurosurgeon to take decision of opting particular treatment (surgery/no surgery) for patient. According to guidelines of the brain trauma foundation and the congress of neurological surgeons, surgical evacuation should be done if volume of EDH is more than 30 cm3 irrespective of GCS [3]. In this case presented, CT scan head shows acute EDH in left fronto-parietal region. CT scan was done same day after injury outside of our institute. Patient came to OPD after one week with the complaints of continuous diffuse headache persisting after injury. Neurologically patient was normal. This time repeat CT scan head showed subacute EDH volume 40.5 cm3 (6 × 2.7 × 5 cm3). Patient was reluctant for surgery, hence advised analgesics and told to come to the hospital immediately if any symptoms suggestive of raised intracranial pressure develop like headache, vomiting, seizures and loss of consciousness. His neurological assessment performed at regular intervals. Headache regressed completely in a week. Patient remains neurologically normal throughout. CT scan head after twelve weeks from injury showed near complete resolution of EDH. Resolution of EDH in this case, where surgical evacuation was indicated as per "guidelines of the brain Trauma foundation and the congress of neurological surgeons, for managing TBI", after putting him on regular CRA. It gives a justified treatment option for nearly asymptomatic EDH with volume more than 30 cm3 in the form of regular CRA, saving patient from complications of surgery and anaesthesia. This also will reduce workload on neurotrauma operation theatre and expenditure on health care. There are no criteria defined till today which will predict about a EDH whether it will increase or resolve with due course of time. However, some authors have reported resolution of EDH like Zakaria, et al. [4], Weaver, et al. [5] and Knuckey, et al. [6]. Purpose of presenting this case is to draw the attention of neurotrauma surgeons that apart from following recommendations of guidelines of the brain trauma foundation and the congress of neurological surgeons in asymptomatic EDH with volume more than 30 cm3, regular CRA is ethically justified treatment approach.
Simple regular clinico-radiological assessment, an ethically justified treatment option for asymptomatic large extradural haematoma with volume more than 30 cm3. Further study needed in support.
None.