Thoracolumbar injury is one of the most common spine injuries. The injury manifesting as neurologic deficit usually requires surgery because of the underlying spinal instability and/or neural compression. The objectives of surgical treatment are to restore the biomechanical stability of the spine and/or to achieve neural decompression.
Aim: The aim of the study was to evaluate short-term outcomes in patients with symptomatic vertebral injury, underwent posterior instrumentation surgery in the acute stage.
Patients and methods: All patients underwent fixation of thoracolumbar injury from November 2007 to October 2018 were included in the study.
Results: A total of 255 patients with unstable fracture were enrolled. Two hundred nineteen (85.88%) were male and 36 (14.11%) females mechanism of injury, 141 (55.29%) patients fall from height. Eighty-two (32.15%) patients involved road traffic accident. Thirty-two (12.54%) patients had direct trauma. Seventy-two (28.23%) patients had American ASIA-A. Fifteen (5.88%) patients ASIA-B. Forty-one (16%) patients ASIA-C. Fifty-one (20%) patient.
ASIA-D and 76 (29.8%) patients ASIA-E. preoperatively evaluated. All patients had pre-operative CAT SCAN & 90% pre-operative Magnetic resonance imaging. T12 and L1 60.6%, involved, L1 37.6%, T12 23%. L2 12.8%.
All patients underwent posterior instrumentation surgery using pedicle screws and connecting rods, either short or long segment. No patient experienced neurologic deterioration perioperatively. Postoperative recovery evaluated heavily depended on the preoperative neurologic status: Fifty-seven (22/35%) patients improved neurologically according to ASIA SCALE. Six patients from ASIA A to C, 2 patients from ASIA A to B, 2 patients from ASIA A to D, 8 patients from B to C,5 patients from B to D. Nineteen patients from C to D, 14 patients from D to E. In general, early surgery better than late surgery for neurological recovery. Complications rate 4.7% but not major complications, none suffered death or permanent morbidity, 3.9% superficial-wound infection, one patient 0.4% mal-position of screws, & one patient 0.4% pulmonary embolism. X-ray follow up satisfactory except 16 patients 6% mild kyphosis. 2 patients 0.8% moderate kyphosis.
Conclusion: The Posterior instrumentation surgery is a safe and efficacious treatment for thoraco- lumber fractures.
ASIA, Acute stage, Decompression, Posterior instrumentation surgery, Thoracolumbar spinal injury
Thoracolumbar injury is one of the common spine injuries. Accidental fall and motor vehicle accident are the two most common causes of this injury [1,2]. Treatment of thoracolumbar injury depends on several clinical factors including age of the patient, mechanism of injury, degree of spinal canal compromised by bony fragments, degree of integrity of the posterior spinal elements, and presence of neurologic deficit [3-5]. Patients with thoracolumbar injury manifesting as neurologic deficit generally require surgical treatment, because they almost invariably have underlying spinal instability and/or neural compression [4,6]. Therefore, the Objectives of surgical treatment are to restore the biomechanical stability of the spine and/or to achieve neural decompression. Several surgical approaches are available for this type of injury, including the anterior, Antero-lateral approach, posterior approach, and combination of both [5-7].
Posterior distraction implants have gained popularity for a long time in the management of posterior ligamentous disruptions and/or anterior bony injuries. The problem of long fixation segment remains. This problem was still present, to a lesser extent, with plate fixation. The principle of screw anchorage to the pedicles, although not without complications, has popularized the concept of short segment fixation. The new modalities of implants can now serve the same goals i.e. to maintain the stabilization and unload the affected segment until healing occurs [1,2,8].
Aim of this study was to evaluate the results of management of unstable injuries of the thoracolumbar spine, with or without neurological deficits, by posterior stabilization using the principles of short and long segments pedicle screws fixation.
Two Hundred Fifty-Five patients with thoracolumbar fractures underwent surgical treatment at Hamad General Hospital, after sustaining high energy trauma between November 2007 - November 2018.
All patients Present with or without neurologic deficit. All of them unstable fractures came to the emergency room. All patients were treated by posterior approach pedicle screw fixation. Most of them underwent surgery within 48 hours of admission, 30% admission to the ward isolated spinal fractures and 70% admission to ICU. Need or asses others injury. The clinical characteristics and outcomes of the 255 patients were investigated retrospectively by meticulous review of medical charts, operative records, and radiographic images.
The patients were positioned prone on a Jackson table under general anesthesia. Short or long segments, either minimal techniques (MIS) used fluoroscopy or navigation systems or open techniques traditional or using navigation systems were exposed periosteal with a standard midline approach.
The superior and inferior boundaries and the transverse processes on either side of the vertebrae were then identified. The screws were placed through the pedicles under C arm x-ray guidance or navigation system guidance.
The entry point to pedicle was the intersection of a line bisecting the transverse process with the lateral margins of the facet joint complex. Tapping of the resultant tract was done. Screws of appropriate length ad diameter were then inserted. If decompression was considered necessary, the lamina over the fractured vertebra was removed.
The screws were connected to the titanium rods bilaterally. Maximal effort was made to achieve optimal alignment. The rods were then connected with a cross-link or without. Postoperatively, all patients underwent a rigorous rehabilitation program, and. Postoperative x-ray done for all of patients and deformity was measured above and below.
All patients with thoracolumbar fractures underwent surgical treatment at Hamad General Hospital, after sustaining high energy trauma between November 2007 - November 2018.
Data were entered and analyzed using SPSS version 23. Categorical variables were reported using numbers (n) and percentages (%). Continuous variables are reported as mean ± SD, and categorical variables were represented as frequency and percentage. The Kolmogorov-Smirnov test proved these variables to be normally distributed. Between-group comparisons were performed by using the chi-square test for categorical variables and the t-test for continuous variables. Differences were considered statistically significant at p ≤ 0.05.
Majority of patients had vertebral injury due to fall (141/55%) (Table 1). The demographic data for the 255 patients are summarized in Table 2. 219 males’ 85.88% and 36 females 14.11%, were aged between 19 to 68 years, 45% ≤ 30 yrs. Causes of thoracolumbar fractures were: fall from height 141 patients (55.29%), motor vehicle accident 82 patients (32.15%), and direct 32 patients 12.54%. Hospital stay ranged from 3 to 70 days.
Table 1: Mode analysis of injury. View Table 1
Table 2: Patients demographic data. View Table 2
The distribution of the type and anatomical level of TL injury is illustrated in Figure 1, and it is mainly L1 and T12.
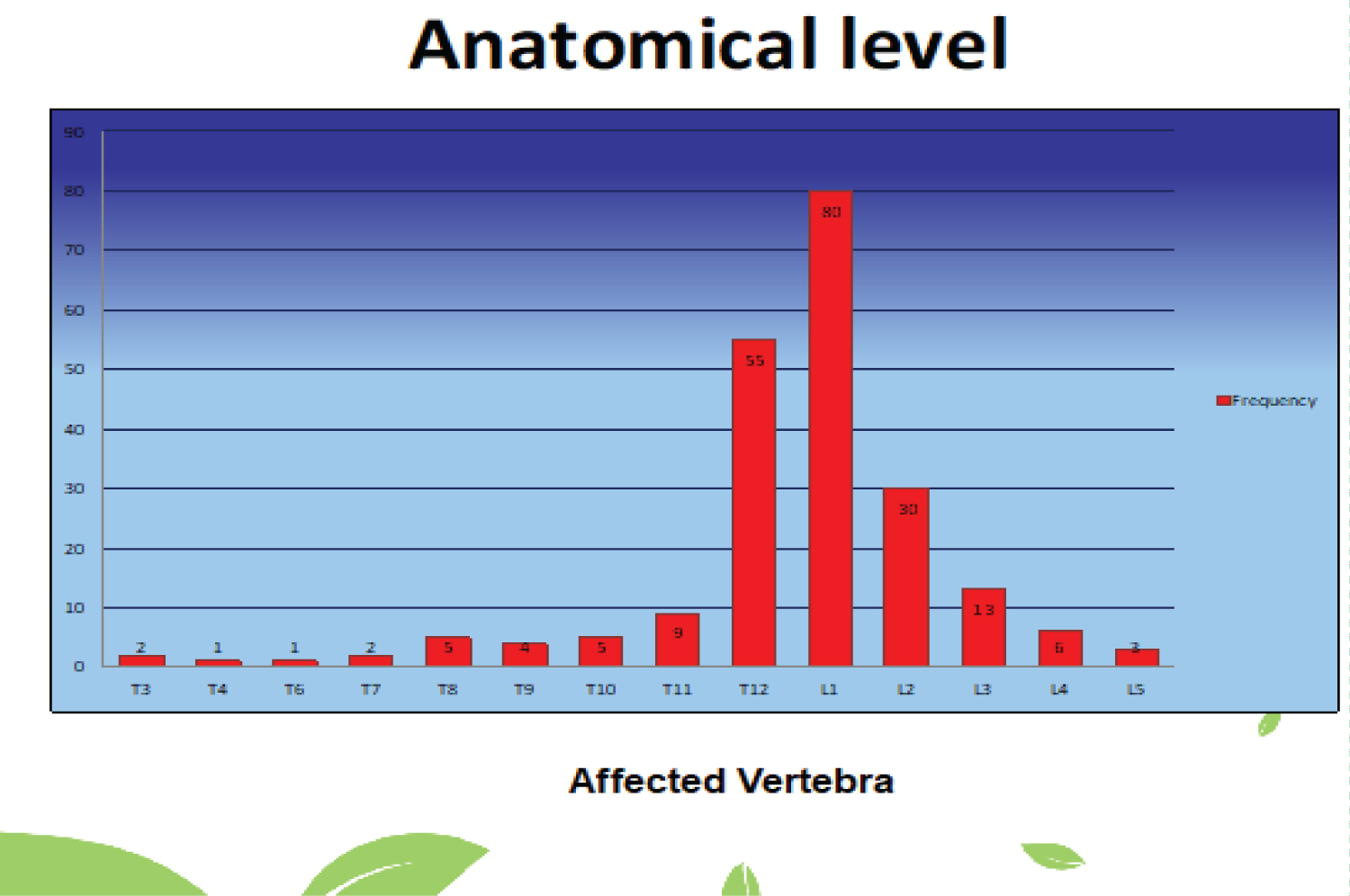 Figure 1: Anatomical level of vertebral injury. View Figure 1
Figure 1: Anatomical level of vertebral injury. View Figure 1
The neurological deficit (Table 3) in each patient was evaluated by the American Spinal Injury Association (ASIA) classification (Table 4). Preoperatively, 72 patients had ASIA Grade A deficits, 15 had Grade-B, 41 had Grade-C, 51 had Grade-D, and 76 had grad E.
Table 3: Neurological status on admission. View Table 3
Table 4: American spinal injury association classification. View Table 4
Surgery was performed for most of them within 48 HOURS of admission in most of them, in whom surgery was delayed after admission because of the associated injuries.
No patient experienced neurologic deterioration in the immediate postoperative period. The follow-up period after discharge was done 70% of them.
The patients underwent routine neurologic examination after discharge. The overall results improved 57 cases 22.35%, are summarized in Figure 2. 72 patients with Grade-A deficits. 10 patients improved, 6 patients of them became grade C, 2 patient was became Grade-B, and 2 patients became Grade D.
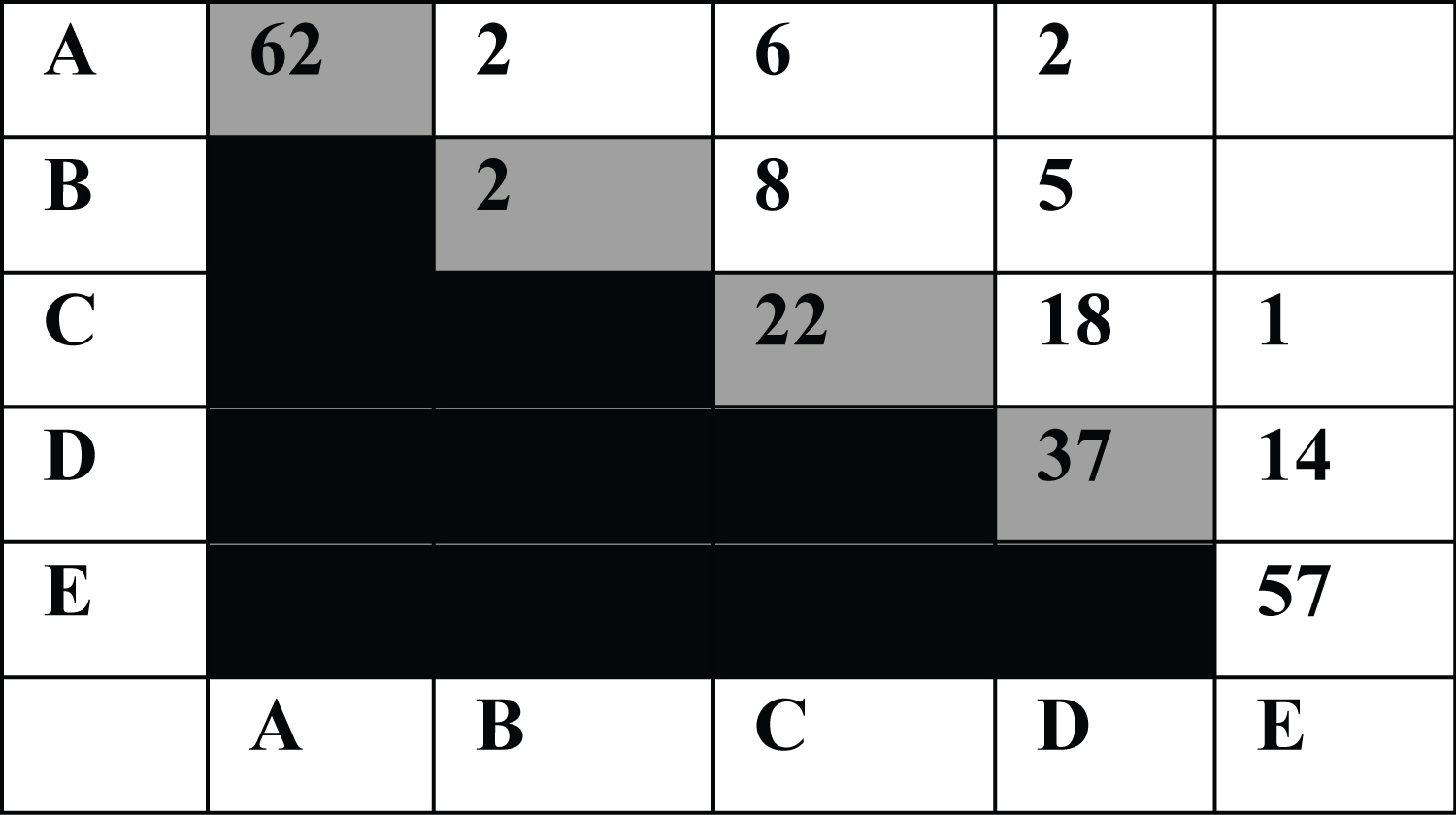 Figure 2: Diagram showing the pre- and postoperative neurologic status of 195 patients, using the American Spinal Injury Association (ASIA) classification. The postoperative status of each patient was evaluated. View Figure 2
Figure 2: Diagram showing the pre- and postoperative neurologic status of 195 patients, using the American Spinal Injury Association (ASIA) classification. The postoperative status of each patient was evaluated. View Figure 2
15 patients with Grade B. 13 patients improved 8 improve to C and 5 to Grade-D.
41 patients GRADE C, 19 patients improved 18 to D and 1 to E.
51 patients GRADE D, 14 patients improved to E.
All patients with grade-E maintained their grade and showed no deterioration.
A total of 12 cases of complications 4.7% that occurred in our series are summarized in Table 5 and Table 6. Intraoperative complicated occurred in one patient who had misplacement of a pedicle screw, which violated the medial pedicle wall and partially protruded into the spinal canal. The misplaced pedicle screw in case of Grade A did and repositioning of the screw was replaced after four days, it was T3. Postoperative complications of infection occurred in 10 patients 3.9%. Superficial wound infection and 1 patient 0.4% developed pulmonary embolism after operative treatment and he was cured.
Table 5: Complications. View Table 5
Table 6: Patients outcome. View Table 6
Recently, treatment of thoracolumbar fracture has undergone a significant paradigm shift. Particularly, the role of surgical treatment for burst fractures has become more obscure [9,10]. Conservative management may be sufficient for patients with stable burst fracture who present without neurologic deficit as shown in a prospective, randomized study in which surgical treatment had no major long-term advantage compared with non-operative treatment [9,11,12]. In contrast, surgery is generally warranted for patients presenting with neurologic deficit, because they almost invariably have underlying biomechanical instability and/or neural compression [11,13]. Therefore, the main objectives of surgical treatment for patients with symptoms are restored of the biomechanical stability/physiological alignment and/or neural decompression. The degree of neurologic recovery after surgery largely depended on the preoperative neurologic status in the present study; patients with ASIA Grade-A deficits usually had a limited neurologic recovery, whereas some with Grade-C or D became ambulatory. The trend has previously been reported by many authors [8,9,14,15].
There have been lengthy debates on whether the anterior or posterior approach should be used for unstable thoracolumbar fractures [16]. The choice of surgical approaches has mostly been anecdotal, influenced heavily by the surgeon's preference and education. In our institution, symptomatic fractures are approached from the posterior direction. The short-term outcomes were generally satisfactory with low rates of serious complications, which have made us convinced that the stand-alone posterior approach may be sufficient for most patients who present with a non-progressive neurologic deficit unless some transitional zone [17-20]. Although there has been concern whether the stand-alone posterior surgery can be adequately stabilized the two or three columns the thoracolumbar fracture [21]. The advocates of anterior surgery have also reported satisfactory results for symptomatic patients operated on from the anterior approach only [22,23]. Although randomized, controlled studies would clarify which approach is more suited for everyone, such studies to compare the efficacy of the two approaches for patients with symptomatic thoracolumbar fracture have never been conducted [22,23]. In that context, a spine surgeon may be allowed to adopt the approach with which he or she feels more comfortable in many circumstances. Generally, the posterior approach is tough to be less effective in neural decompression compared with the anterior approach [6,24,25]. In experienced hands, adequate spinal canal decompression can be achieved with a combination of laminectomy and ligamentotaxis. On the other hand, the posterior approach was essential because of the presence of posterior ligamentous disruption.
The number of thoracolumbar vertebral segments to be incorporated into the posterior instrumental fixation also remains controversial. In our institution, we are doing both short and long segments, we did not find significates different unless in some cases of transitional zone. Although the range of motion may be diminished after a long segment posterior fixation, the risk of hardware failure is smaller compared with a short-segment posterior fixation that is, fixation incorporating the two vertebrae (one above and one below the fractured segment). Laboratory as well as clinical studies revealed that short-segment posterior fixation may be biomechanically incompetent to support the destroyed or weakened vertebral column in patients with unstable burst fracture [26,27]. However, short-segment posterior fixation is superior to long-segment fixation in that the range of motion is less compromised and the risk of pedicle screw related complications is smaller because of a short segment fixation uses half the number of pedicle screws [20,28]. The injection of poly-methyl methacrylate into the fracture vertebral body to strengthen the anterior column in combination with a short segment posterior fixation has been improvised to overcome the shortcomings of conventional short-segment fixation [7,29]. The technique may be beneficial in selected patients.
There are several limitations in the present study. Firstly, this is a retrospective case series, without different treatment methods for comparison. Although we are convinced that posterior instrumentation surgical is a safe and efficacious treatment, it cannot be determined whether the posterior approach is superior to the anterior approach, or vice versa. Secondly, because of the limited duration of the follow-up period, the long-term outcomes, including the quality of life parameters, of the patients could not be evaluated.
The Posterior instrumentation surgery is a safe and efficacious treatment for thoraco-lumber fractures with lesser complications.