We report an exceptional case of vertebral artery aneurysm presented with dyspnea and cough symptoms which is misdiagnosed with bronchiectasis. Literature showed that cough can be an exceptional symptom of vertebral aneurysms.
Vertebral aneurysms presented with cough are rare and might be confused with other lung diseases such as pneumonia, chronic obstructive lung disease (COPD) or bronchiectasis.
Introduction: Giant intracranial aneurysms are rare entities defined by a diameter of at least 25 mm, accounting for 5% of all cases of intracranial aneurysm. These aneurysms can treat with endovascular; flow diverters, stents, primary coiling and combined treatments and vascular procedures such as clipping, or bypass surgeries. In the present case report, because of the main symptoms of cough and dyspnea, aneurysm diagnoses are delayed and the patient had a treatment of bronchiectasis over a year.
Conclusion: Cough and dyspnea can be the only symptoms of the aneurysms. Vertebral aneurysm should be in the differential diagnoses of coughs that doesn't alleviate.
Vertebral artery aneurysm, Endovascular treatment, Cough, Dyspnea
Giant intracranial aneurysms are rare entities defined by a diameter of at least 25 mm, accounting for 5% of all cases of intracranial aneurysm [1]. As their nature of rarity giant aneurysms are less seen in posterior circulation and associated with high mortality and morbidity [2]. Due to small size of posterior fossa, posterior circulation aneurysms can present with cranial nerve palsies, hydrocephalus, motor impairment therefore substantial mass effect. Because of the mass effect, infrequently vertebral artery aneurysm can confer with cough and dyspnea due to vagal nerve deterioration [3]. Although, anterior circulation aneurysm can treat with endovascular; flow diverters, stents, primary coiling and combined treatments and vascular procedures such as clipping, or bypass surgeries also posterior circulation can be treated with same methods on the other hand they have poor outcomes when we compare with the anterior circulation aneurysms. Regarding the giant and complexity of aneurysms cannot be managed with surgical strategies, Flow diversion such as pipeline embolization devices with coil assistance is an alternative treatment [4]. However, the mortality and morbidity rates of posterior circulation aneurysm treated using flow diversion devices are much higher compared with those of pre circulation aneurysm [5]. In the present case report, because of the main symptoms of cough and dyspnea aneurysm diagnosis is delayed and the patient had a treatment of bronchiectasis over a year.
The patient was a 47 year old female admitted to Ankara Bilkent City Hospital (Ankara, Turkey) in June 2018, who had been experiencing symptoms of cough, dyspnea and hoarseness for 1 year. Her cough was treated with several antibiotics and diagnosed with bronchiectasis but there was no improvement of her complaints. In June 2019 because of the progression of her dyspnea, admitted to our hospital's emergency service. Her tachypnea got worse and saturation fell down. At last, the patient has elective intubation in the E.R. On the elective intubation, E.R doctor noticed that the patient's left vocal cord was paralyzed and an emergent head and cervical computer tomography angiography performed. Ct scans revealed a large vertebrobasilar aneurysm and obvious compression of the brainstem (Figure 1). Patient transferred to a neurosurgery intensive care unit and started antibiotic of teicoplanin with the loading dose of 400 mg 2 × 1 and continued 400 mg 1 × 1.
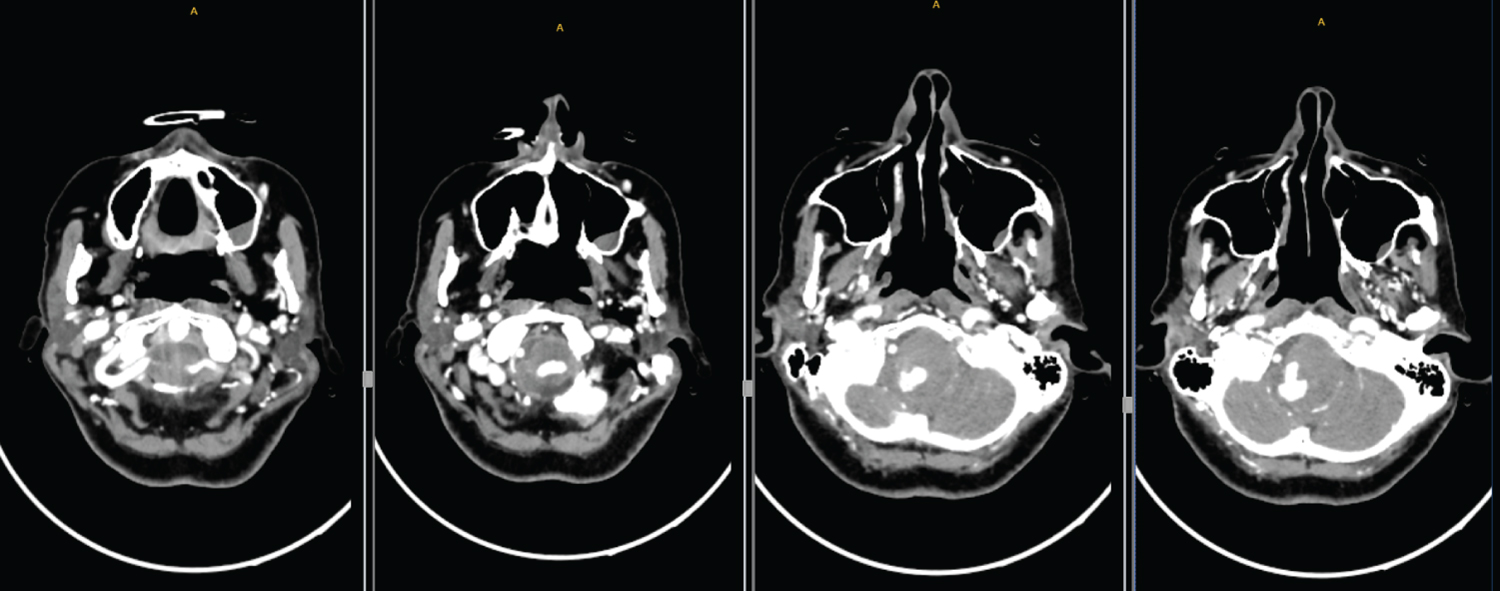 Figure 1: Ct scans revealed a large vertebrobasilar aneurysm and obvious compression of the brainstem. View Figure 1
Figure 1: Ct scans revealed a large vertebrobasilar aneurysm and obvious compression of the brainstem. View Figure 1
Physical examination was performed before intubation by the E.R. doctor and showed an obvious right slant tongue extension, right sided walking with Medical Research Council [6] grade 5 muscle strength in the right limb and negative bilateral finger to nose and heel to knee tibia tests with normoactive reflexes. After admission to the ICU, the patient underwent digital subtraction angiography (DSA) at Ankara Bilkent City Hospital. A giant spherical aneurysm right vertebral V4 segment aneurysm with a maximum diameter of 30 mm was identified (Figure 2).
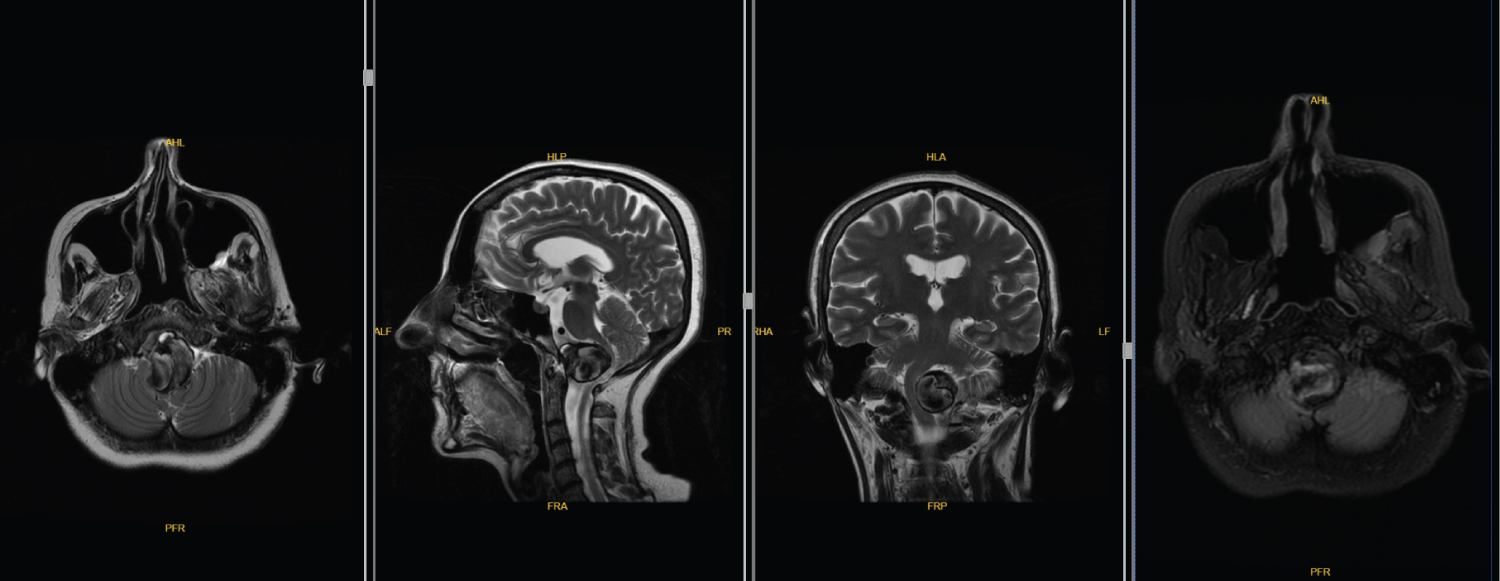 Figure 2: A giant spherical aneurysm right vertebral V4 segment aneurysm with a maximum diameter of 30 mm was identified. View Figure 2
Figure 2: A giant spherical aneurysm right vertebral V4 segment aneurysm with a maximum diameter of 30 mm was identified. View Figure 2
Informed consent was provided by the patient and her relatives prior to endovascular therapy. A treatment plan was formulated after angiography. First, a microcatheter (headway 17) was placed through the right vertebral artery and the Pipeline was completely released through the right VA. Subsequently, the aneurysm was relatively tightly embolized with coils. Clopidogrel was administered with a loading dose of 300 mg and continued with 75 mg per day. The Clopidogrel resistance test was evaluated with 72% on day 4. At 5 days following hospitalization, the giant aneurysm of the V4 segment was embolized with Pipeline 5 × 35 mm flow diverter device. Stagnation of blood in the aneurysm was seen in control angiograms.
For 2 days following the endovascular treatment, the patient was listless and complained of a headache worse than those that had occurred during the pre embolization period. Physical examination revealed no new positive signs. Postoperative the patient transferred to the neuro-ICU and on post-operative day 2 her vitals were improved and extubated. Antibiotics were stopped on the day 10 of the admission. The patient was transferred to the Neurosurgery inpatient service at the day of 12 of her admission.
After 2 months of the operation, the patient had increased white phlegm and her choking cough was continuing. Furthermore, the patient's right limb muscle strength was improved compared with that pre embolization and the patient has Medical Research Council grade 5 muscle strength in the right limb. Three months after embolization, re examination of the head MRI and MRA revealed that the aneurysm was completely occluded [Raymond Roy classification, Class I [7]]; although, the brainstem was still compressed when comparing with the pre-embolization Mri (Figure 3). At 12 months after surgery, her phlegm was markedly improved and discontinued with the medical drugs. Cough and hoarseness disappeared. Re examination of DSA revealed no aneurysm recurrence [Raymond Roy classification, Class I [7]] and no stenosis in the parent artery on MRI (Figure 4) and computer tomography angiography (Figure 5). The modified Rankin scale score [8] of the patient is 1 point.
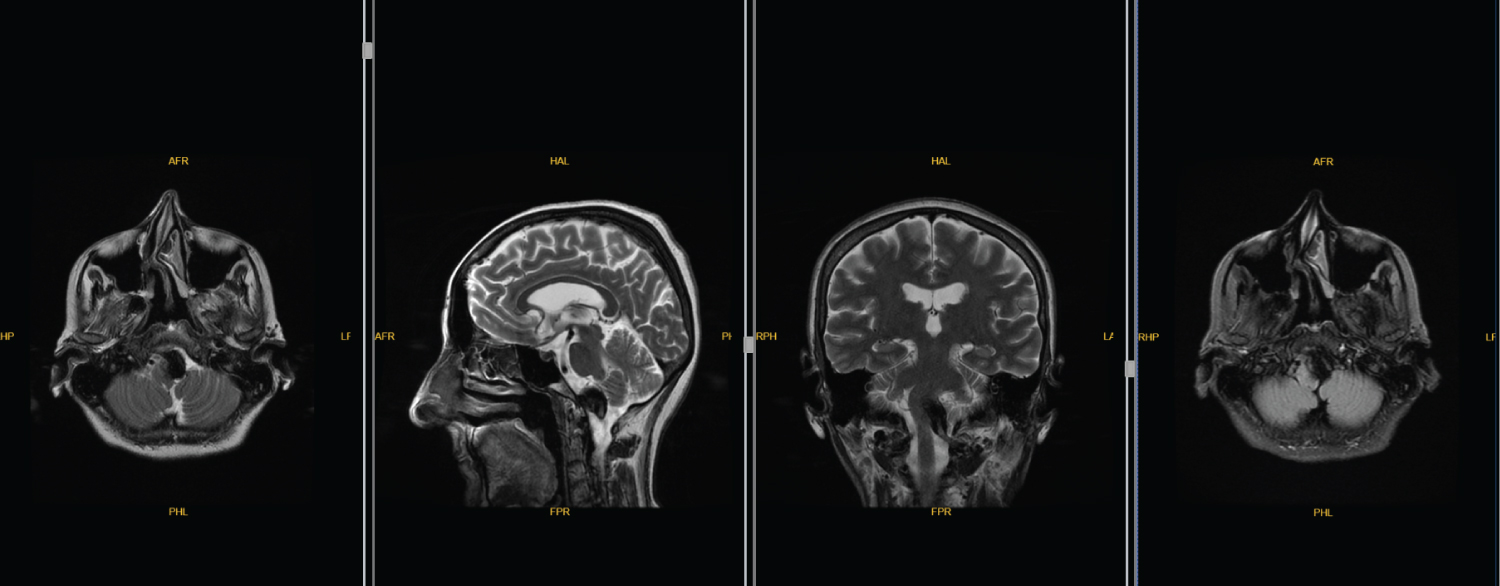 Figure 3: At 12 months after surgery, her phlegm was markedly improved and discontinued with the medical drugs. View Figure 3
Figure 3: At 12 months after surgery, her phlegm was markedly improved and discontinued with the medical drugs. View Figure 3
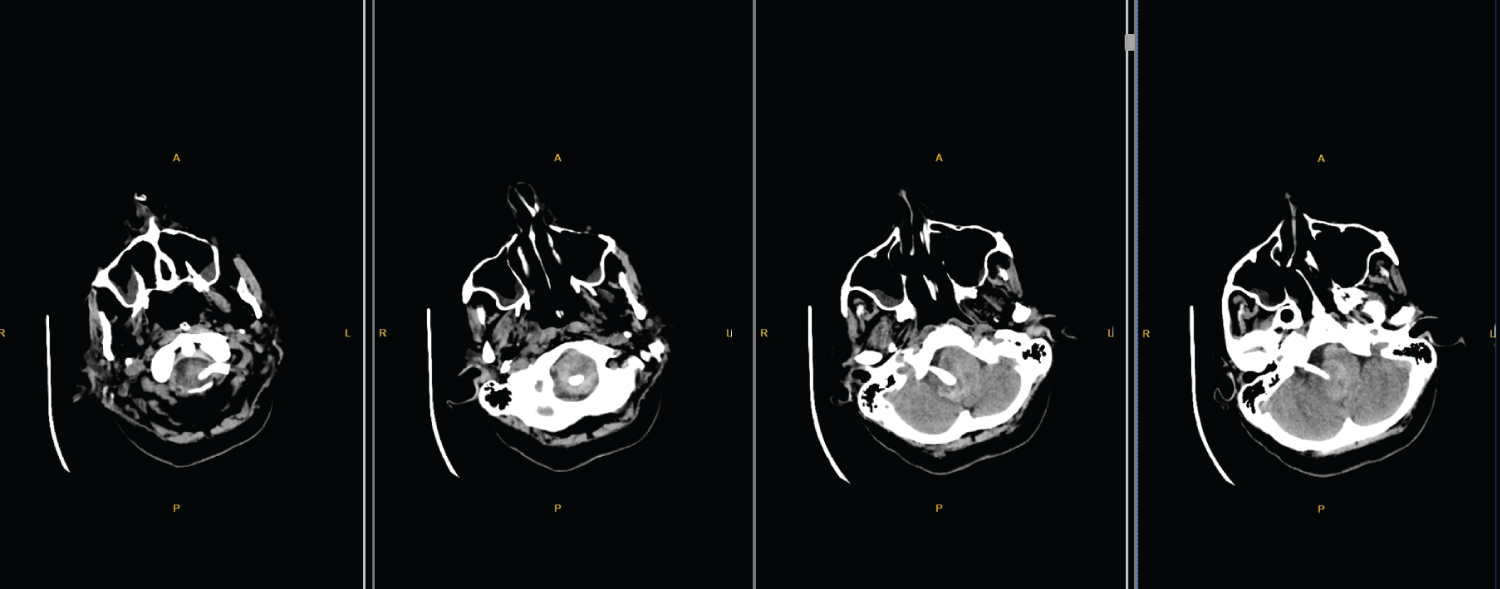 Figure 4: No stenosis in the parent artery on MRI. View Figure 4
Figure 4: No stenosis in the parent artery on MRI. View Figure 4
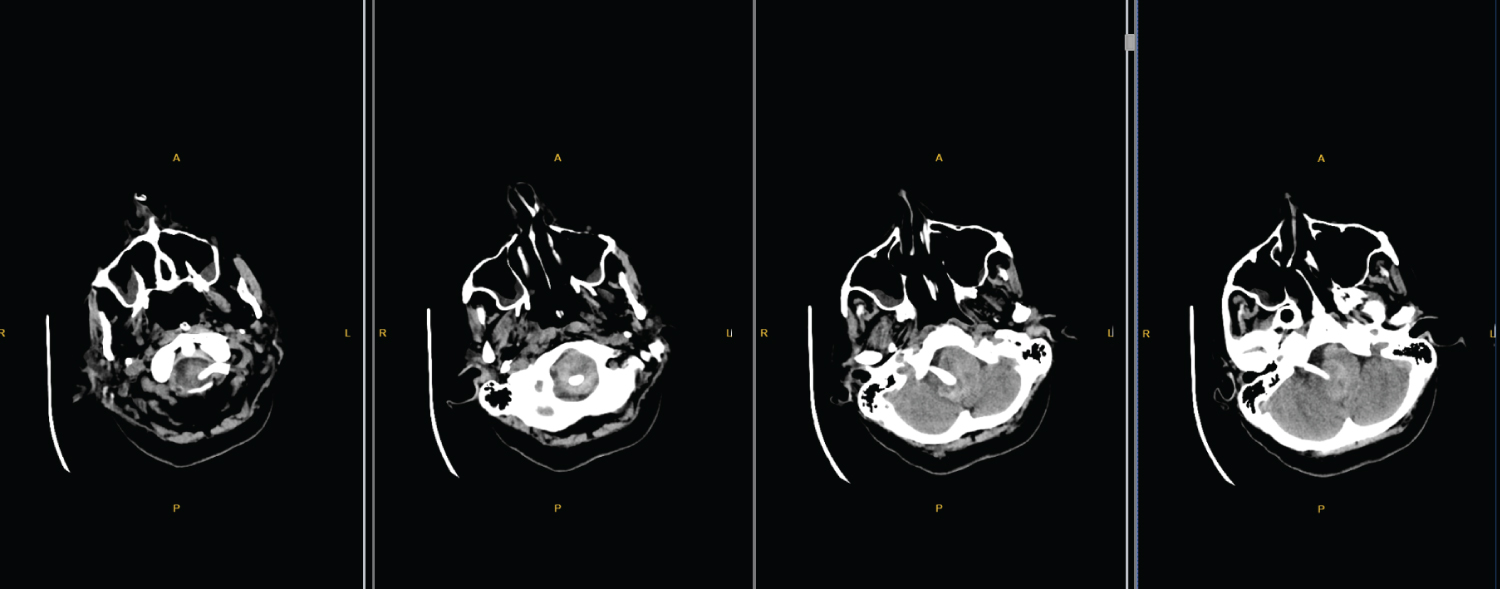 Figure 5: Computer tomography angiography. View Figure 5
Figure 5: Computer tomography angiography. View Figure 5
Flow diverters are a more widely accepted tool for aneurysm treatment within the last decade.
A recent meta analysis by Ye, et al. [5] reported an aneurysm occlusion rate of 78.8% after an average follow up of 6.3 months, and neurological morbidity and mortality rates after FDD treatment were 9.8 and 3.8%, respectively. The rupture rate of giant, unruptured, posterior circulation aneurysms within 5 years may be up to 50% [8]. The relevant factors to be considered when treating such complex aneurysms include the shape, location, vascular architecture and collateral circulation of the aneurysm's parent artery. Treatment of these aneurysms has always posed a great challenge for neurosurgery. Though, the complication rate (the number of complications divided by the number of patients) of complex posterior circulation aneurysms treated with flow diversion devices is significantly higher compared with that of anterior circulation aneurysms, reconstruction of the parent artery with coil embolization is a suitable alternative when surgical treatment fails. Up To date, only a small number of studies have reported on the treatment of giant aneurysm at the VBJ. Liang, et al. [8] described the endovascular treatment of 99 patients with large or giant aneurysms of the posterior circulation, 12 of which were located at the VBJ; 3 of those 12 cases were treated by occluding the contralateral VA with coils, and the bilateral VA was sacrificed in 1 of the 12 cases. Beyond shadow of doubt, cough and dyspnea can be the only symptoms of the aneurysms. Vertebral aneurysm should be in the differential diagnoses of coughs that doesn't alleviate.
This report followed guidelines to be HIPAA compliant and permission was obtained from the patient to publish identifiable photographs. Written informed consent was obtained from the patient for publication of this case report and accompanying images. The study adhered to the tenets of the Declaration of Helsinki.
None of the authors have a proprietary interest in this study or any conflicts of interest to disclose.
We declare no financial support of this case report.
The authors confirm contribution to the paper as follows: study conception and design: Ergun Daglioglu and Ilkay Akmangit; data collection: Yigit Can Senol and Ayberk Karaman. Draft manuscript preparation: Bige Sayın. All authors reviewed the results and approved the final version of the manuscript.