The information about symptomatic pulmonary cement embolism (PCE) following vertebroplasty and cement-augmented pedicle screw fixation is limited. To our knowledge, this is the first reported case of severe acute respiratory distress syndrome (ARDS) caused by a relatively small amount of peripheral PCE, which resulted in mortality.
A 78-year-old man underwent L1 corpectomy and reconstruction and posterior fixation for painful T11, T12, and L1 burst fracture and concurrent osteonecrotic changes of the L1 vertebral body. Cement-augmented pedicle screws with bis-GMA cement injection were applied to increase the fixation strength. Mild productive cough occurred on the third postoperative day, and chest computed tomography revealed scattered small cement emboli over bilateral lung fields. The patient's performance was fair until the clinical scenario deteriorated rapidly and dramatically to ARDS on the sixth postoperative day. Delayed presentation of severe symptomatic PCE was observed. Despite the venous-venous extracorporeal membrane oxygenation implementation (VV-ECMO) for respiratory support, his clinical condition did not improve. The patient passed away 46 days after the surgery.
Small scattered PCE could be catastrophic. Although most cases seem to be asymptomatic or run a subclinical course, clinicians should pay attention to the potential for rapid aggravation.
Pulmonary cement embolism, Acute respiratory distress syndrome, Bis-GMA, Bone cement, Cement-augmented pedicle screws, Vertebroplasty
ARDS: Acute Respiratory Distress Syndrome; Bis-GMA: Bisphenol A-Glycidyl Methacrylate; CT: Computed Tomography; EVVP: External Vertebral Venous Plexuses; ICU: Intensive Care Unit; IVC: Inferior Vena Cava; IVVP: Internal Vertebral Venous Plexuses; MRI: Magnetic Resonance Imaging; PCE: Pulmonary Cement Embolism; VV-ECMO: Venous-Venous Extracorporeal Membrane Oxygenation Implementation; VVS: Vertebral Venous System
Since percutaneous vertebroplasty was established in 1987, cement augmentation of the vertebral body has been widely used around the world. Percutaneous vertebroplasty is used in the treatment of osteoporotic fracture or osteolytic lesions caused by tumors for patients who have medically intractable debilitating pain. Osteoporotic patients who have instability that requires instrumentation also benefit from cement-augmented pedicle screw implantation to increase the fixation strength. Cement leakage is not uncommon according to the previous literature, but is easily neglected by clinicians because most patients remain asymptomatic. The information about cement leakage causing symptomatic PCE is limited, and the treatment strategies are uncertain. Severe symptomatic PCE has been described in a few previous reports, and most of the reported cases were related to a large central PCE. We experienced a rare case of ARDS caused by a relatively small amount of peripheral PCE following cement-augmented pedicle screw fixation.
A 78-year-old man with a history of hypertension and atrial fibrillation under regular and effective medical control presented and was hospitalized for disabling back pain for four months. Prior to this episode, the patient revealed a history of T11 incomplete burst fracture with spinal cord compression two years ago, and underwent surgery of laminectomy from lower T9 to upper T11, posterior fixation with pedicle screws implantation (T9, T10, T12, and L1), and T11 vertebroplasty at another hospital. Unfortunately, the kyphosis progressed and the lower screws pulled out. They were removed nine months ago at the same institution. However, the mechanical back pain progressed in the past four months. Magnetic resonance imaging (MRI) revealed a recent T12 and L1 complete burst fracture in addition to the old T11 fracture. The pain gradually increased and was refractory to analgesic therapy. Suspicious of non-union with osteonecrosis of the L1 vertebral body was noted on the follow-up MRI (Figure 1). Therefore, he came to our institution for help.
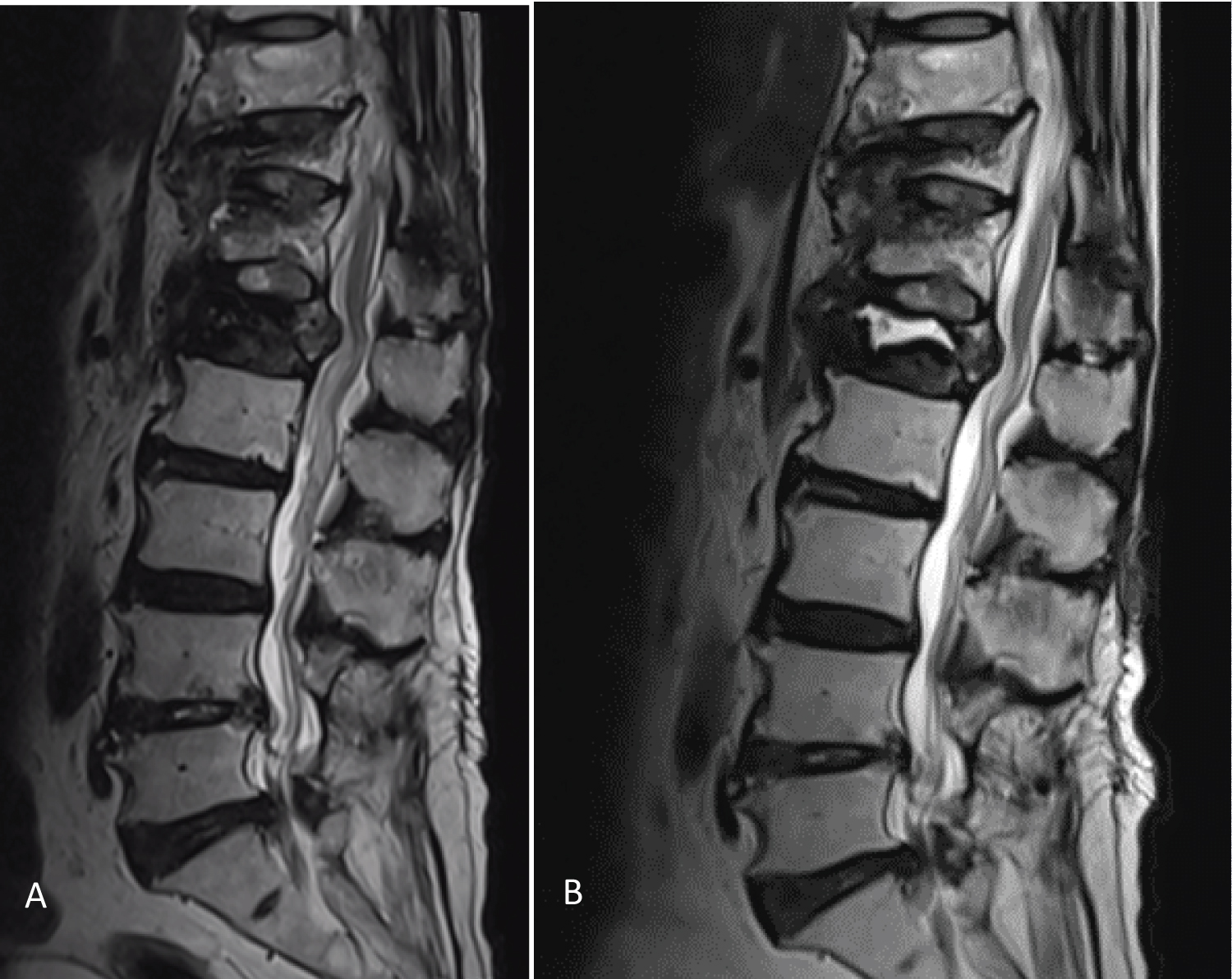 Figure 1: Preoperative magnetic resonance imaging.
Figure 1: Preoperative magnetic resonance imaging.
Initial magnetic resonance imaging showed burst fracture over T11, T12, and L1 vertebral bodies (A). 3 months later (B), T2-weighted image showed homogeneous hyperintensity at the anterior superior portion of the L1 vertebral body. The margin of the hyperintense area is well demarcated. Osteonecrosis is present.
View Figure 1
Upon admission, the patient was not ambulatory due to severe pain. His muscle strength was normal during an examination when he lay on the bed. No abnormality was noted during the physical and neurological examination, except for the numbness over the bilateral lower extremities, sequelae of a previous episode. The preoperative electrocardiogram showed a normal sinus rhythm and no evidence of myocardial ischemia or infarction. Ultrasound cardiography showed a borderline left heart size but preserved ejection fraction. A mild restrictive ventilatory defect was noted on a pulmonary function test. Bone mineral density revealed osteopenia (the T-score was -2.3 over the L3 level). Laboratory parameters were within the normal range.
The patient underwent a combined anterior and posterior approach for the surgery. The first stage was L1 corpectomy and reconstruction with a body cage through a left retropleural approach in the right decubitus position. Then, the patient was changed to a prone position for the second stage of the surgery with posterior fixation over the T8, T9, T10, T12, L2, and L3 level; cement-augmented screws were applied to the T8 and L3 levels. The total volume of injected bone cement was 1 ml (0.5 ml per pedicle) at T8, and 2 ml (1 ml per pedicle) at L3. No intraoperative cement leakage was detected. The total duration of the operation was 466 minutes, with an estimated blood loss of 900 ml. During the operation, hypotension was noted, and it was stabilized with inotropic agents and component therapy. No desaturation or change in end-tidal CO2 was reported.
The patient was admitted to the intensive care unit (ICU) postoperatively, and the hemodynamics were stabilized with taper off of the inotropic agent. Thoracolumbar spine computed tomography (CT) was performed on the first postoperative day to check the instrument position. All of the implants were in a good position, but a small amount of cement leakage was suspected over the left side segmental artery of L3 (Figure 2).
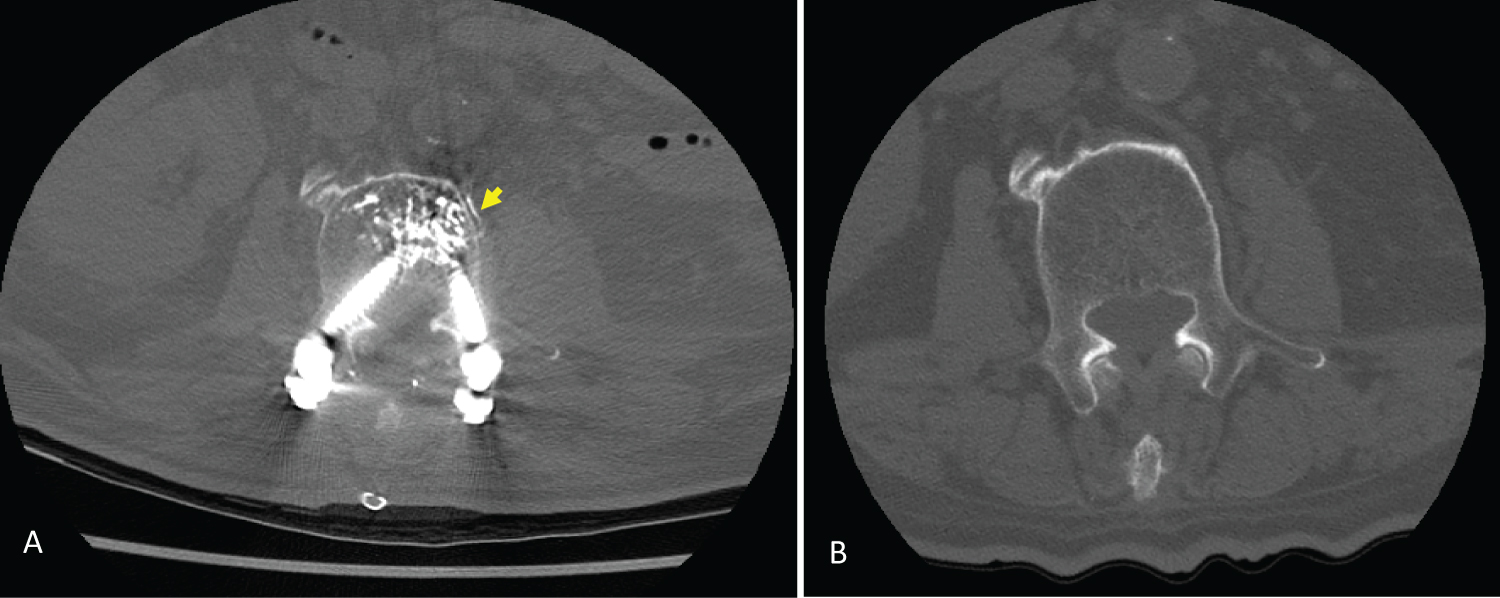 Figure 2: Postoperative lumbar spine computed tomography.
Figure 2: Postoperative lumbar spine computed tomography.
High attenuation bone cement (arrow) was noted over the left side segmental artery of L3 in postoperative computed tomography (A), which was not seen on preoperative computed tomography (B).
View Figure 2
On the third postoperative day, the patient developed a mild productive cough with yellowish sputum, and chest plane film showed pronounced lung markings. Chest CT revealed subsegmental cement embolism at the bilateral upper lung field with reduced perfusion (Figure 3A, Figure 3B and Figure 3C). Owing to a fair respiratory condition and lack of other symptoms except a productive cough, no anticoagulant agent was prescribed. Extubation was done smoothly. After two more days of close observation and monitoring in the ICU, the patient was transferred to the ordinary ward on the fifth postoperative day.
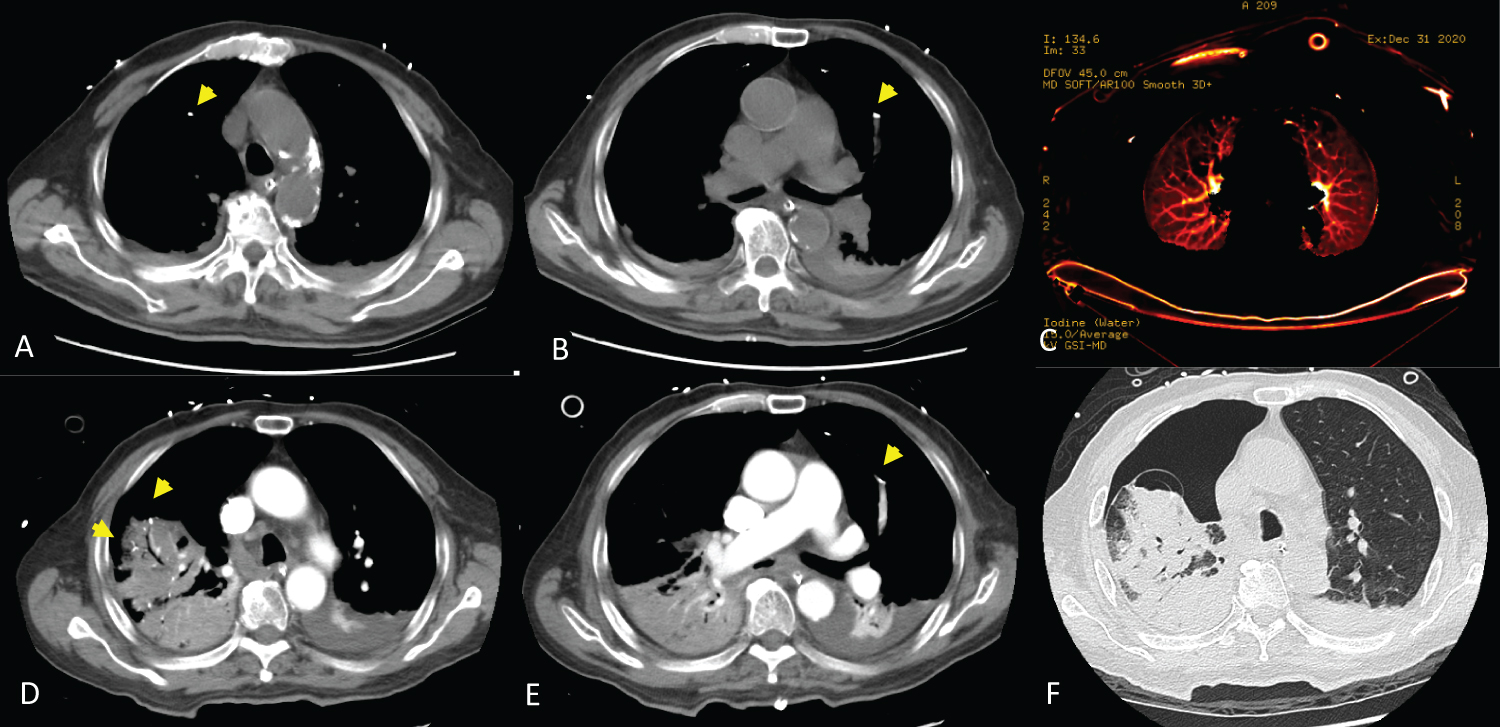 Figure 3: Postoperative chest computed tomography.
Figure 3: Postoperative chest computed tomography.
Chest computed tomography on the third postoperative day showed scattered small tubular and branching dense opacities (arrow) along the course of the subsegmental arteries over bilateral anterior upper lung fields, with pulmonary cement emboli (A,B); Reduced perfusion was noted over those regions (C); Chest computed tomography on the fifth postoperative day revealed many visible cement emboli (D,E); Right lung atelectasis, bulla formation over the right upper lung adjacent to the cement embolus, and right-sided pneumothorax (F).
View Figure 3
However, his symptoms were rapidly aggravated by the next morning, and he became agitated, dyspnea, and increased oxygen demand. His oxygen saturation by pulse oximetry (SpO2) dropped to 88% despite oxygen supplementation with a mask (98% oxygen at 10 L/min), the respiratory rate was 36 breaths/min, the pulse rate was 96 beats/min, and the blood pressure was 98/72 mmHg. Arterial blood gas was pH 7.44, PaO2 53.6 mmHg, and PaCO2 37.2 mmHg.
Endotracheal intubation was performed for respiratory failure, and he was transferred to the ICU. Chest CT was repeated and revealed right lung atelectasis, bulla formation over right upper lung adjacent to the cement embolus, and right-sided pneumothorax (Figure 3D, Figure 3E and Figure 3F). The bulla formation, which might be related to a pulmonary infarction and resulted in pneumothorax, was not seen on previous CT series. A chest tube was inserted into the right pleural cavity for drainage. Due to pneumothorax with persistent air leakage, the setting of the mechanical ventilator was conservative. The inspired oxygen fraction could barely taper. Arterial PO2 (PaO2) on an FiO2 of 0.8 was 86.1 mmHg. The ratio of PaO2 to inspired oxygen fraction (P/F ratio) was 107.6, which confirmed ARDS. Delayed presentation of severe symptomatic PCE was observed. Laboratory profile revealed elevated D-dimer 3.77 mg/L (normal range: less than 0.56) and C-reactive protein 12.33 mg/dL. Other laboratory parameters were within the normal range. Antibiotics were prescribed for coverage of any possible infection.
Because of the persistent air leakage, chest surgeon was consulted. The patient underwent biportal video-assisted thoracic surgery for right upper lobe wedge resection and decortication on the tenth postoperative day. Necrotizing parenchyma of the lung, bulla formation with air leakage from right upper lobe, moderate thick whitish pleural peel deposition, and around 200 mL turbid pleural effusion were noted during the operation. The operative findings were compatible with pulmonary infarction resulting in pneumothorax.
His respiratory condition improved transiently to a P/F ratio 138.29 (96.8/0.7), but worsened on the next day. PaO2 on an FiO2 of 1.0 dropped to 43.9 mmHg, and VV-ECMO support was indicated. The VV-ECMO implantation was performed by a cardiovascular surgeon smoothly on the eleventh postoperative day. Sedative agents and heparin infusion began after VV-ECMO implantation. The activated partial thromboplastin time was around 40 to 60 seconds. The patient's lung condition did not improve despite the full support of VV-ECMO. Follow-up chest CT on the twenty-first (Figure 4) showed further consolidation of bilateral lung parenchyma and persistent right-sided pneumothorax. A grave prognosis was apparent, and the patient expired within a half hour after withdrawal of VV-ECMO support on the forty-sixth postoperative day.
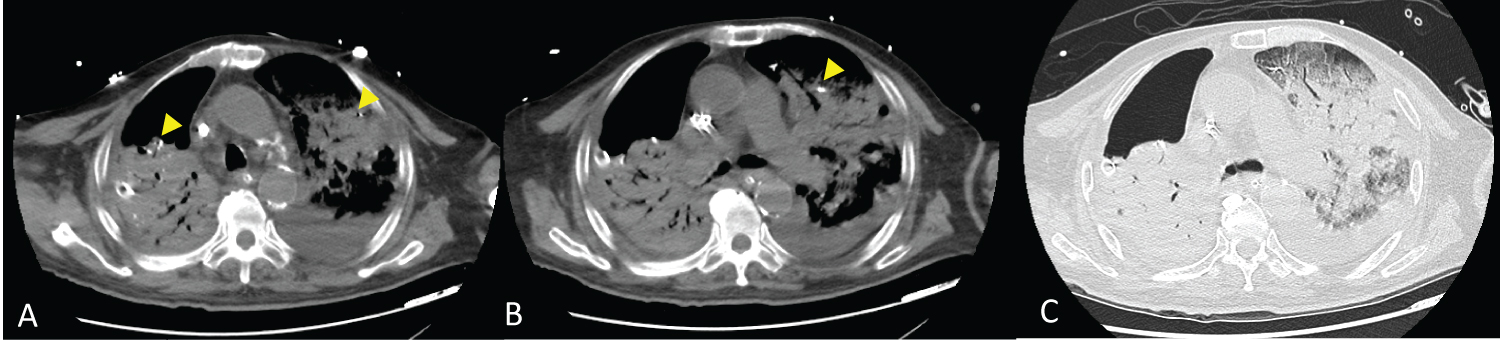 Figure 4: Chest computed tomography on the twenty-first postoperative day showed pulmonary cement emboli (arrow), further consolidation of bilateral lung parenchyma, and persistent right-sided pneumothorax.
View Figure 4
Figure 4: Chest computed tomography on the twenty-first postoperative day showed pulmonary cement emboli (arrow), further consolidation of bilateral lung parenchyma, and persistent right-sided pneumothorax.
View Figure 4
Cement augmentation had been applied to successfully treat patients with osteoporotic fractures, metastatic tumors, multiple myeloma, and vertebral hemangiomas [1,2]. Indications for vertebroplasty are severe refractory pain or progressive collapse as a result of osteoporotic compression fractures or pathological compression fracture without signs of instability, myelopathy, or radiculopathy [1,3-5]. In patients with signs of instability, posterior fixation is usually required. However, the risk of instrumentation failure is increased in the osteoporotic spine due to poor bone quality, and cement-augmented pedicle screws could significantly increase the fixation strength in osteoporotic bone [6,7]. Both percutaneous vertebroplasty and cement-augmented pedicle screw fixation require an injection of bone cement into the vertebral body.
In the previous literature, cement leakage is common in both surgical procedures, with rates from 5% to 87% in vertebroplasty [8-18] and from 13% to 93.6% in cement-augmented pedicle screws [6,7,19,20]. Venous leakage reported in the previous literature might affect up to 43% of cases [14-17,20,21]. More than 98% of the leakages remained asymptomatic [18]. Occasionally, major complications of cement leakage occurred, including intracardiac embolism, cardiac perforation [12-14,16,22,23], pulmonary embolism [2-7,9,11,12,14-17,19-21,24-40], pulmonary infarction requiring pulmonary wedge resection [27], ARDS [24], paradoxical cerebral arterial embolism [23,41], and it might result in a catastrophic outcome in rare cases.
Pulmonary cement embolisms during augmented vertebral procedures have been extensively reported. The frequency of PCE ranged from 2.1% to 26% in previous reports [2-4,9,10,12,15,25-27], depending on the types of images studied. Some authors suggested routine postoperative chest radiography [4,24]. On the other hand, CT scan has been considered the "gold standard" to assess cement leakage by some authors because the incidence dramatically increased when chest CT was performed rather than chest radiography [5,8,12,15]. The cement emboli may appear with a punctuate, tubular or branching, high attenuation area of more than 500 Hounsfield units [2,13,26]. The locations, the lengths, and the number of pulmonary cement pieces could be clearly visualized on CT angiography [3].
Most of the patients remained asymptomatic [1-3,8,9,11-13,25,39]. Symptoms related to PCE were noted in only 0.4% to 0.9% of cases [2,12]. It might present as dyspnea, tachypnea, chest tightness, chest pain, cough, tachycardia, palpitation, cyanosis, hemoptysis, pleural effusion, dizziness, and sweating [3-5,7,11-13,16,17,24,25,36-39,42]. Symptoms can occur during the operation, but more commonly begin days to weeks, or even months or years, after the procedure [2,5,16,27,39]. The mean time until the appearance of symptoms begins 2 days after the procedure [42]. Careful attention must be given to patients who have respiratory symptoms, especially among those with fever or hypotension [37]. If there is dyspnea, chest pain, and hemodynamic instability, this indicates a poor prognosis or the requirement for invasive intervention or emergency cardiopulmonary resuscitation [25].
Pulmonary cement embolism is attributed to the venous leakage of bone cement through the vertebral venous system (VVS). The VVS is a complicated valveless network, comprised of basivertebral veins, internal vertebral venous plexuses (IVVP), and external vertebral venous plexuses (EVVP). The basivertebral veins are within vertebral bodies, the IVVP consist of an epidural network surrounding the thecal sac, and the EVVP surrounding the vertebral column. The VVS connects to the systemic venous system mainly by the EVVP. With a connection between the anterior EVVP and lumbar/intercostal veins, the blood flow could reach the inferior vena cava (IVC), azygos vein, hemiazygos vein, and superior vena cava. The blood flow is bidirectional, depending on the changes of the intrathoracic and intraabdominal pressure [10]. Pathophysiologically, the leaked bone cement drained through the basivertebral veins or the anterior EVVP into the systemic venous system, reaching the cardiopulmonary system and resulting in PCE [5,10,11,24,42]. In previous studies, cement leakage into the azygos vein [6,15] and IVC [33,38] exposed the patient to a risk of PCE. Nevertheless, most cement leakages were not detected intraoperatively, and nearly all reported PCE cases were detected postoperatively [4,5,9,15,17,23,26,35,38]. Highly vascularized lesions, such as pathological fractures associated with malignancy, have a higher risk of cement venous leakage [5,37]. The osteoporotic compression may destroy the vertebral body and thereby reduce bony hindrance of the venous drainage, allowing a direct shunt of the cement fragment to the venous system [24].
Pathophysiologically, although incompletely understood, ARDS might result from an increase in capillary permeability, which can be attributed to obstruction of the pulmonary arterial circulation, a direct cytotoxic effect of pulmonary cement embolus on pulmonary endothelial cells, and activation of inflammatory cascades [4,5,24,34]. Prothrombotic effects caused by a cement embolus have also been described and could additionally lead to progressive occlusion of the pulmonary artery [3,16,27].
The actual effect of bone cement on lung damage remains uncertain. Many studies or case reports showed variable parenchymal changes on chest CT, at least in the acute stage [24,27,35,42], regardless of whether they have symptoms or not [9]. Conversely, some studies did not find reactive pulmonary changes on CT scans performed immediately [9,26] and 1 year after the operation [26]. The VERTOS II study indicates that cement emboli do not cause long-term structural changes of the pulmonary parenchyma after a mean follow-up of almost 2 years [15]. Venmans, et al. reported that incidentally found pulmonary cement embolism had no significant impact on all-cause mortality [11].
Several recommendations have been made to prevent cement leakage into the circulation [2-5,10,13,14,17,18,24,25,36,40,43]. First, the cement should be injected when it has a viscous, toothpaste-like consistency [2,3,39]. Second, high-resolution fluoroscopy is required for better leakage detection. Biplane fluoroscopy is recommended by many authors [1,4,18,24,35,42,44]. Third, an appropriate volume of cement injected in repeated small quantities is preferred [4,5,7,9,17,18,25,26]; It is recommended that a single injected volume should not exceed 0.3 ml [25]. The total amount of injection should be limited to 4 to 6 mL per vertebral body in vertebroplasty [2,5], and 1.5 to 2 ml per pedicle screw in cement-augmented pedicle screw instrumentation [7,21]. In cement-augmented pedicle screw instrumentation, injection of volumes above 3 mL per pedicle would seem to confer an increased risk without obvious benefit in terms of fixation strength [19]. Fourth, the augmentation of many vertebral bodies in one session should be avoided, and greater attention should be paid during a multilevel procedure [5,13,45]. It is not recommended that more than three vertebral segments be filled with bone cement at a time in vertebroplasty [14,25]. In cement-augmented pedicle screw instrumentation, there is a statistically significant relationship between PCE and > 7 instrumented levels, > 14 cement-augmented pedicle screws, and > 20-25 ml total cement volume [6]. Fifth, the injection should be stopped or held when the bone cement reaches the posterior quarter or least two-thirds of the vertebral body, fills the fracture gap, or if any leakage is detected [2-5,8,26,36,38,40]. Sixth, the risk of cement leakage will decrease obviously in a delayed operation (> 2 weeks after fracture) [25]. Last, cortical destruction, the presence of an epidural soft-tissue mass, highly vascularized lesions and severe vertebral collapses are factors that increase the rate of complications [1,5,8,37,45].
The utility of antecedent vertebral venography is controversial [1,4,5,17,18,35,36]. The venography might identify a direct shunt from the needle tip to the venous system; however, the contrast medium has a different viscosity and flow characteristics, which could not represent that of bone cement [1,4,36]. The venography could predict cement leakage into endplates or central defects in 100% of cases, but could only predict leakage into the venous structures in 29% of cases [43]. Furthermore, the opacification of the contrast agent could hinder and disturb the evaluation of intraoperative cement detection [1,4,5].
There are no treatment guidelines for PCE currently. In previous published studies, initiation and choice of treatment depended on the location of the cement embolus and the presence of clinical symptoms [3,11,12,25]. Supplemental oxygen could be delivered to maintain PaO2 > 60 mmHg and SpO2 > 90% [4]. For patients with asymptomatic peripheral PCE, no anticoagulant is required. In patients with symptomatic peripheral PCE or asymptomatic central PCE, initial intravenous heparinization followed by 6 months of consecutive warfarin is suggested [2,3,13,39]. Anticoagulation therapy reduces the risk of activation of coagulation and thrombus formation on the embolic material, and then prevents further pulmonary infarction and necrosis of the lung parenchyma [3-5,32,36,37,42]. After 6 month of anticoagulation therapy, the foreign object is endothelialized, and the risk of progression of the occlusion is decreased [2,3,13,39]. Although six months of anticoagulant treatment is widely accepted, the actual duration for anticoagulant agents has no consensus [11,25].
Surgical embolectomy or endovascular intervention should only be considered and performed in cases of symptomatic central PCE with respiratory or right-sided heart failure [4,24,39,42]. Some studies also suggested that aggressive surgical or endovascular intervention should be performed in patients with intracardiac emboli and IVC emboli due to a high risk of cement migration, cardiopulmonary failure, and cardiac perforation [2,12,32,45]. Conservative treatments may fail to yield a good result in these patients [4,24,45].
Rarely, a case requiring pulmonary resection resulting from necrosis from PCE has been reported. Rothermich, et al. [27] reported a symptomatic case with right lower lung lobe infarction owing to massive cement embolization to his pulmonary arterial branches. The patient underwent open pulmonary wedge resection and embolectomy through a median sternotomy using cardiopulmonary bypass, and continued to have a chronic and debilitating pulmonary deficit during follow-up.
To our knowledge, only 5 cases reported in previous literatures passed away due to PCE, and most of these cases were related to large central PCE [24,28,29,31,33]. Among the 5 cases, only one patient expired because of ARDS [24]. Two patients developed hemodynamic collapse and received cardiopulmonary resuscitation. One of them presented typical symptoms of grave acute pulmonary embolism about 15 minutes after vertebroplasty, and did not survive after extended cardiopulmonary resuscitation [28]. The other had cardiac arrest about six hours after vertebroplasty, and was successfully resuscitated within 10 min. However, the patient did not regain consciousness over the following 9 days, and eventually died after bilateral occipitotemporal infarctions were confirmed [29]. One patient with right pulmonary and right atrial thromboembolic masses presenting with severe tricuspid regurgitation underwent successful surgical removal of the mass and tricuspid annuloplasty, but eventually died from septic shock [31]. The last patient had ventilatory and hemodynamic symptoms of pulmonary embolism, and died 8 days after vertebroplasty despite treatment with oral anticoagulants. The details are unknown [33].
To our knowledge, our patient is the first patient who had lethal PCE with ARDS resulting from small peripheral PCE after surgery of cement-augmented pedicle screw instrumentation. The clinical course and respiratory failure developed insidiously relative to patients with large central PCE. The clinical condition deteriorated gradually, resulting in extensive pulmonary infarction and necrosis. Our patient passed away despite aggressive treatment.
Our patient is believed to be the first reported patient who had lethal ARDS caused by a relatively small amount of scattered peripheral PCE after surgery of cement-augmented pedicle screw instrumentation. Symptomatic PCE is rare but could bring about catastrophic results to the patients. Clinicians should pay attention to the occurrence of cement leakage during the operation, and observe the patient intensively after the operation whether cement leakage was noted intra-operatively or not. Although there is no uniform treatment guideline for PCE, anticoagulant agents for symptomatic peripheral PCE and asymptomatic central PCE are acceptable. Surgical or endovascular intervention is reserved for symptomatic PCE, intracardiac cement embolism, and perhaps IVC cement embolism.
The authors report no conflict of interest concerning the materials ormethods used in this study or the findings specified in this paper.
Chia-Jung Hsieh and Fon-Yih Tsuang were the patient's neurosurgeons. Chia-Jung Hsieh reviewed the literature and contributed to manuscript drafting; Fon-Yih Tsuang was responsible for the revision of the manuscript for important intellectual content; all authors issued final approval for the version to be submitted.