The term 'tandem spinal stenosis' (TSS) is usually used to describe a double stenotic lesion in the cervical and lumbar spine, which are the most mobile segments of spine. There have also been a few reports describing the clinical course of tandem thoracic and lumbar spinal stenosis. Triple-region spinal stenosis (TRSS), or concurrent stenosis in the cervical, thoracic, and lumbar spine is the least documented variety of tandem spinal stenosis in literature. Combination of three co-existing pathologies may make the clinical picture very confusing with co-existing upper and lower motor neuron signs when lesions at all 3 levels are symptomatic. Also, it may become confusing for a clinician to distinguish between the upper motor neuron signs resulting due to Cervical and thoracic compressions. We have put forth a case series of 5 patients with TRSS, operated in staged manner in an attempt to shed more light on TRSS and its management. More attention in form of larger studies for management of TRSS, one of the most complex degenerative spinal pathologies is the need of the hour for enlightening the spine surgeons.
Tandem spinal stenosis, TRSS
With advancement of medical science and increased longevity of the population, the incidence of spinal stenosis is on rise. Spinal stenosis is narrowing of the neural canal and foramina, resulting in the compression of the neurologic structures with resultant symptoms [1]. Cervical and Lumbar regions, the most mobile segments, are most commonly affected. Tandem spinal stenosis (TSS) is defined as significant spinal stenosis occurring in two different regions of the spine [2]. TSS typically presents with concomitant cervical and lumbar stenosis. Thoracic canal stenosis is less reported in the literature than the other two regions. Triple-region spinal stenosis (TRSS), or concurrent stenosis in the cervical, thoracic, and lumbar spine is the least documented variety of tandem spinal stenosis in literature. Combination of three co-existing pathologies may make the clinical picture very confusing with co-existing upper and lower motor neuron signs when lesions at all 3 levels are symptomatic. Also, it may become confusing for a clinician to distinguish between the upper motor neuron signs resulting due to Cervical and thoracic compressions. The classic clinical TSS triad consists of (1) Intermittent claudication, (2) Mixed upper and lower extremities symptoms and signs, and (3) Progressive gait disturbances [3]. Additional thoracic compressive pathology can alter this characteristic picture and can make surgical decision-making very difficult. Even though the incidence might be much higher actually, only one case of TRSS has been reported in the literature till now as per our knowledge and there is a serious lack of consensus about the approach to surgical management of these patients [4]. We have put forth a case series of 5 patients with TRSS, operated in staged mannerin an attempt to shed more light on TRSS and its management and draw the attention towards this complex pathology.
An 80-year-old farmer was referred with bilateral leg pain with inability to walk for long distances since 1 year. He also had started developing weakness of both lower limbs since 6 months. Weakness had progressively worsened and now patient was losing balance while walking. Patient didn't have any complaints related to bowel or bladder dysfunction. Hoffman reflex and Grip sign was positive with hyperreflexia in both upper limbs. Both Knee and ankle reflexes were hyporeflexic. Power in all joints of upper and lower limbs was grade 4. Spasticity was uniform in all 4 limbs. Babinski's sign was absent bilaterally. In view of contrasting clinical picture, MRI cervical and lumbar spine with whole spine screening was done. MRI revealed Triple-Region Spinal Stenosis. It showed Cervical canal stenosis from C5 to C7 with myelomalacia signals in cord. At thoracic spine, stenosis was seen at D10-11 level due to Hypertrophied ligamentum flavum. Opinion of three different radiologists was taken who confirmed absence of cord oedema or myelomalacia at that level. On MRI Lumbar spine, significant canal stenosis was observed at L3-4 & L4-5. Patient was a known case of IHD and was treated with CABG 6 years back.
Management: Since spasticity was same in both upper and lower limbs, C5-6, C6-7 ACDF was carried out in stage one and L3-L5 Microscopic posterior decompression was carried out in stage two, 4 days later. Staged procedure was carried out keeping the co-morbidities of the patient in mind. Following the procedure, Patients' gait imbalance improved to a great extent by 8 months with Nuric grading improving to Grade 1 from Grade 3, with no bladder/bowel complaints. As a result, thoracic decompression was not carried out and the patient has been on a close watch for 1.5 years post op (Figure 1).
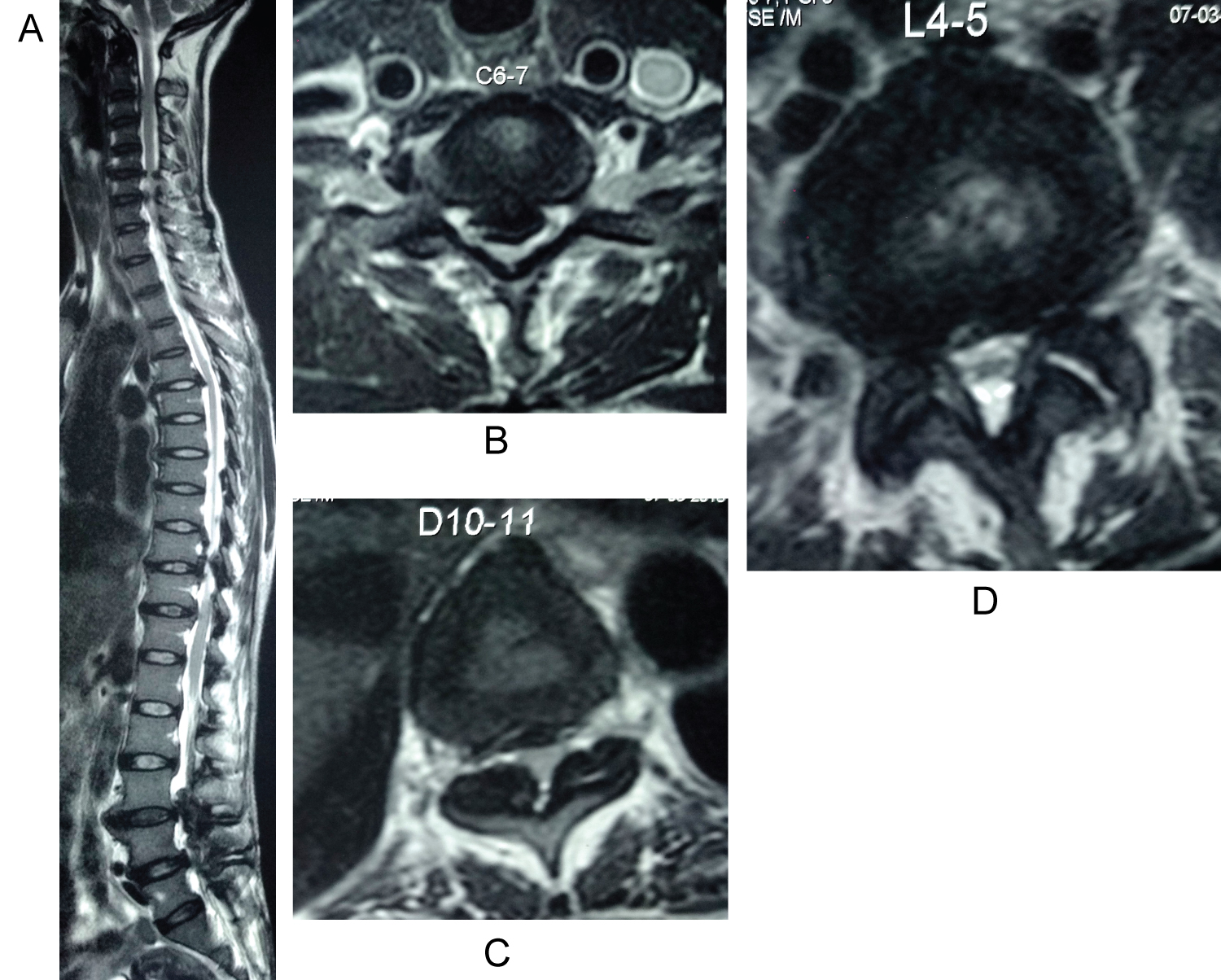 Figure 1: Whole spine sagittal cut showing TRSS at C5-C7, D10-11, L3-5. Axial section at the level with maximum compression - Cervical cord at C6-7, Thoracic cord at D10-11 and Lumbar spine at L4-5.
View Figure 1
Figure 1: Whole spine sagittal cut showing TRSS at C5-C7, D10-11, L3-5. Axial section at the level with maximum compression - Cervical cord at C6-7, Thoracic cord at D10-11 and Lumbar spine at L4-5.
View Figure 1
A 65-year-old male patient came to OPD with Chief complaints of loss of balance while waking and inability to walk without support. Patient was having these symptoms since 4 months which worsened over the time. He also had back pain, bilateral leg pain with inability to walk for long distances since 14 months but had learnt to live with it. Since last one month he had 2 episodes of urinary retention which were resolved with simple rubber catheter insertion. On examination, Power in both upper limbs was grade 4 and grad 3 in both lower limbs. Lower limbs were more spastic as compared to the upper limbs. Both upper and lower limbs showed hyper-reflexia with positive Babinski's and Hoffman's sign. Patient was a known diabetic and hypertensive since 10 years and was on regular medications with good glycemic control. Grip release test was positive and Hoffman's sign was present. MRI Cervical spine with whole spine screening revealed Triple-Region Spinal Stenosis. MRI of Cervical spine revealed severe canal stenosis secondary to Ossified Posterior Longitudinal Ligament from C3-C7. Signals of myelomalacia were present at these levels. Thoracic spine showed cord compression due to hypertrophied ligamentum flavum at D5-6. Lumbar spine had canal stenosis at L1-2, L3-4, and L4-5 levels.
Management: In view of clinical examination, more spasticity in lower limbs than in upper limbs, co-morbidities and severity of compression of cervical and thoracic cord, only Cervical and thoracic decompression was carried out in first stage in a same sitting by two spine surgeons simultaneously. Unfortunately, Post-operatively, patient developed respiratory failure and succumbed due to the same on 14th post-operative day (Figure 2).
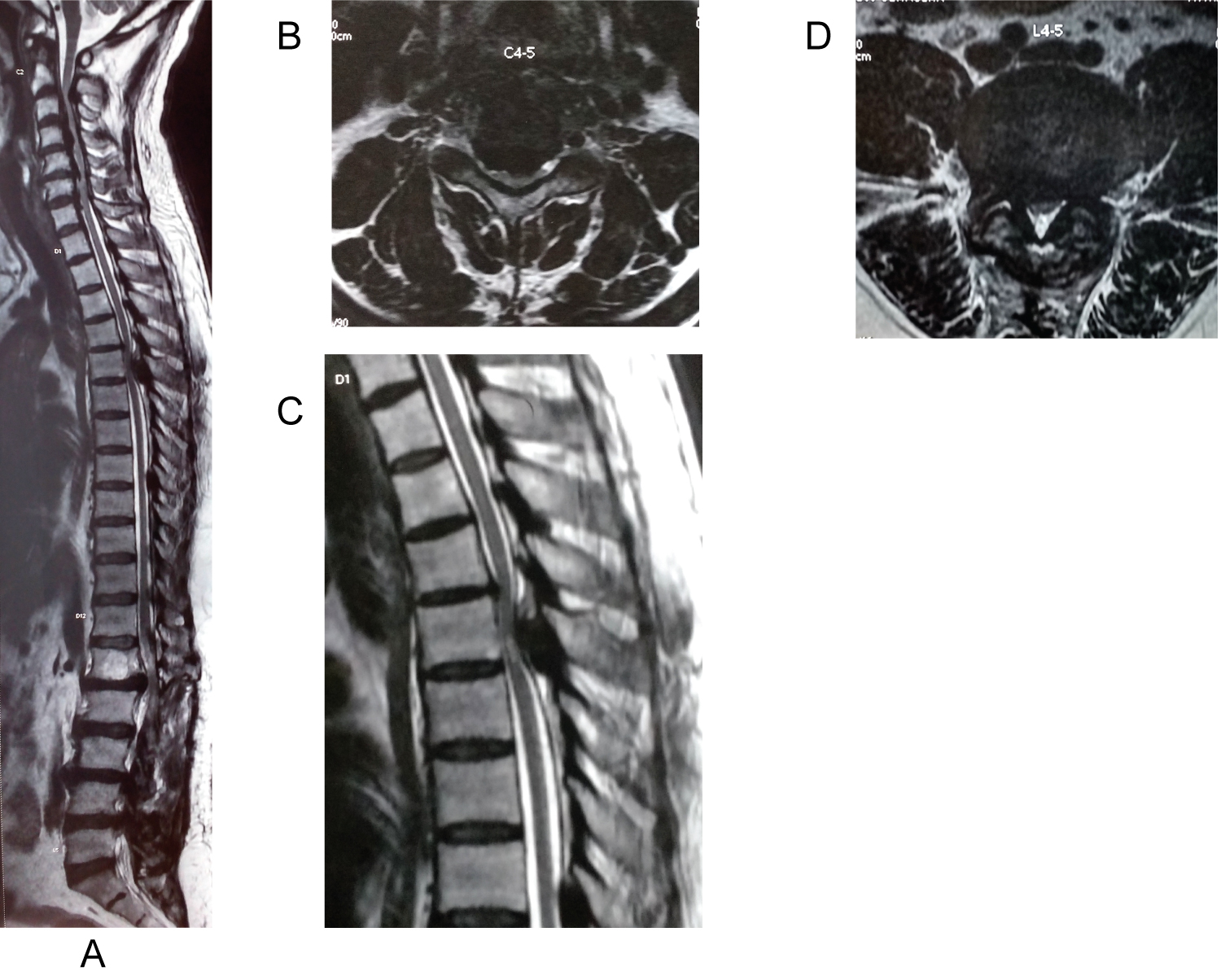 Figure 2: Whole spine sagittal cut showing TRSS at C3-C7, D5-6, L1-2 & 3-L5. Axial section at the level with maximum compression - Cervical cord at C4-5, thoracic cord with cord myelomalacia at D5-6, lumbar spine at L4-5.
View Figure 2
Figure 2: Whole spine sagittal cut showing TRSS at C3-C7, D5-6, L1-2 & 3-L5. Axial section at the level with maximum compression - Cervical cord at C4-5, thoracic cord with cord myelomalacia at D5-6, lumbar spine at L4-5.
View Figure 2
A 71-years-old female, a domestic worker had a fall at home 1 year prior to presentation complicated by chronic back pain and bilateral leg pain without claudication on clinical presentation, she reported a 3-month-old history of loss of balance while walking, worsening leg weakness, with numbness in both of her forearms and hands, with difficulty while dressing up and combing the hair. He had increased urinary frequency and occasional constipation since 3 weeks.
On examination, Power in both upper limbs and lower limbs was 4.Lower limbs were more spastic as compared to the upper limbs. Both upper and lower limbs showed hyper-reflexia with positive Babinski's. Grip release test was positive. Patient was a known diabetic and hypothyroid since 15 years and was on regular medications. MRI Cervical spine with whole spine screening revealed Triple-Region Spinal Stenosis. MRI of Cervical spine revealed severe canal stenosis secondary to Ossified Posterior Longitudinal Ligament from C3-T1. Signals of myelomalacia were present at these levels. Thoracic spine showed cord compression due to hypertrophied ligamentum flavum at D10-11 with cord oedema. Lumbar spine had canal stenosis at L4-5 levels.
Management: In view of cord signals in cervical and thoracic spine, hyper-reflexia in all 4 limbs Posterior Cervical decompression (C3-T1 decompression with Lateral mass fixation) and thoracic decompression (D10-11 posterior decompression with Left facetectomy and fusion) was carried out in first stage in a same sitting by two spine surgeons simultaneously. Patients gait improved over 6 months from Nurick Grade 3 to Nurick Grade 2, but bladder symptoms didn't resolve. Patient gradually started having worsening of bilateral leg pain and claudication so was operated L4-5 posterior decompression after 6 months after trying conservative management (Figure 3).
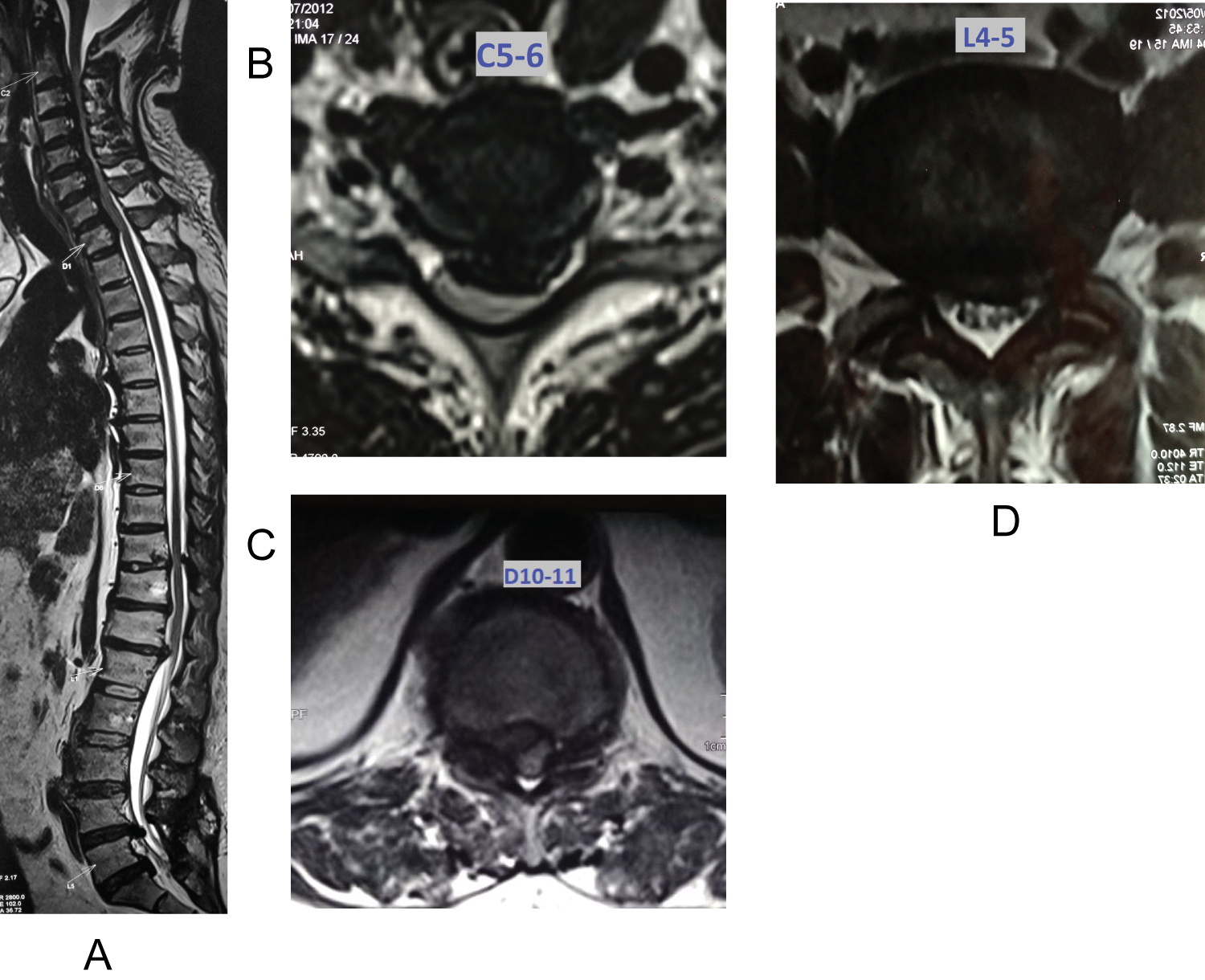 Figure 3: Whole spine sagittal cut showing TRSS at C3-T1, D10-11, L4-5. Axial section at the level with maximum compression - Cervical cord at C5-6, Thoracic at D10-11, lumbar at L4-5.
View Figure 3
Figure 3: Whole spine sagittal cut showing TRSS at C3-T1, D10-11, L4-5. Axial section at the level with maximum compression - Cervical cord at C5-6, Thoracic at D10-11, lumbar at L4-5.
View Figure 3
A 66-years-old male presented with low back pain and bilateral leg pain since 6 months and difficulty while walking since 2 months. He also complained of increased urinary frequency and urgency since 1 month. He had no previous history of trauma to back.
On examination, Power in both upper limbs was grade 5 and lower limbs was grade 4. Lower limbs were more spastic as compared to the upper limbs. Grip release test and fine activities of hand were normal. Upper limbs reflexes were exaggerated, in lower limbs, knee reflex was exaggerated and ankle reflex was diminished. Patient was a known hypertensive since 12 years and diabetic since 8 years and was on regular medications. MRI Cervical spine with whole spine screening revealed Triple-Region Spinal Stenosis. MRI of Cervical spine early cervical canal stenosis secondary to localised Ossified Posterior Longitudinal Ligament from C5-C7. Thoracic spine showed cord compression due to a disc protrusion and calcification at D7-8 with cord oedema. Lumbar spine severe had severe canal stenosis at L4-5 level.
Management: In view of normal upper limb power and normal fine activities, Patient was operated for posterior Lumbar and thoracic decompression in first stage. D7-8 Transforaminal fusion and L4-5 Transforaminal fusion was only was carried out in a same sitting by two spine surgeons simultaneously. Patient's nurick grade (grade3) did not worsen, upper limb power and fine activities remained normal, so patient has been kept on close watch for 1 year post-operatively and has not been operated for cervical decompression yet (Figure 4).
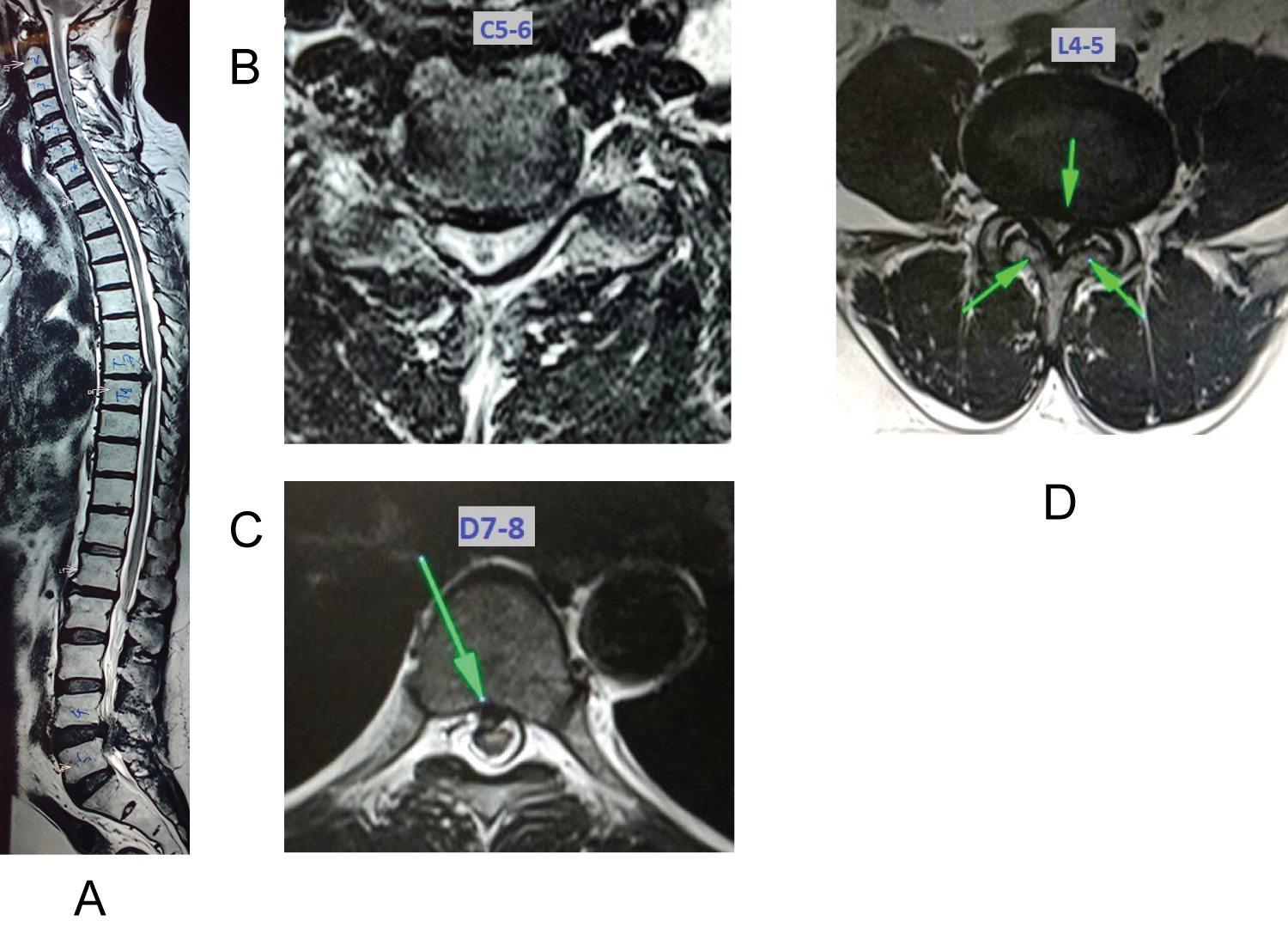 Figure 4: Whole spine sagittal cut showing TRSS at C5-C7, D7-8 and L4-5. Axial section at the level with maximum compression - cervical cord at C5-6, thoracic cord at D7-8, Lumbar spine at L4-5.
View Figure 4
Figure 4: Whole spine sagittal cut showing TRSS at C5-C7, D7-8 and L4-5. Axial section at the level with maximum compression - cervical cord at C5-6, thoracic cord at D7-8, Lumbar spine at L4-5.
View Figure 4
A 72-years-old male presented with weakness of both lower limbs since 3 months. He also had bilateral leg pain with inability to walk for long distances since 8 months with walking distance without taking a halt decreasing gradually. Weakness in lower limbs had progressively worsened over 3 months and now patient was losing balance while walking. Hoffman reflex and Grip sign was positive with hyperreflexia in both upper limbs and hyporeflexia in both lower limbs. Power in all joints of upper and lower limbs was grade 4. Babinski's sign was absent bilaterally. Patient didn't have any complaints related to bowel or bladder dysfunction. Patient was a known case of IHD, Hypertension and Hypothyroidism. In view of contrasting clinical picture, MRI cervical and lumbar spine with whole spine screening was done. MRI revealed Triple-Region Spinal Stenosis. It showed Cervical canal stenosis at C3-4 and C5-6. At thoracic spine, stenosis was seen at D8-D11 level due to Hypertrophied ligamentum flavum and disc herniations. On MRI Lumbar spine, significant canal stenosis was observed at multiple levels from L2 to L5.
Management: C3-C7 posterior Cervical Laminectomy and L2-L5 posterior Lumbar decompression was performed in a single setting, and patient was monitored for functional betterment. 4 months post-operatively, patient started having urinary hesitancy and constipation, so he was operated with D8-D11 posterior decompression (Figure 5 and Table 1).
 Figure 5: Whole spine sagittal cut showing TRSS at C3-4 & C5-6, T9-T11, L1-L5 levels. Axial section at the level with maximum compression- cervical cord at C5-6, lumbar spine at L3-4.
View Figure 5
Figure 5: Whole spine sagittal cut showing TRSS at C3-4 & C5-6, T9-T11, L1-L5 levels. Axial section at the level with maximum compression- cervical cord at C5-6, lumbar spine at L3-4.
View Figure 5
Table 1: Summery of the clinical picture. View Table 1
The first description of tandem Spinal stenosis was probably from by Portal of France in 1803 [5]. Brain and Wilkerson put forth the concept co-existing of spinal stenosis at multiple areas in 1957 [2]. The term tandem spinal stenosis (TSS) was later coined by Dagi, et al. [6]. Epstein stated that 5% of patients with spinal stenosis have symptoms at both levels [7]. The term 'tandemspinal stenosis' is usually used to describe a doublestenotic lesion in the cervical and lumbarspine [8]. There have also been a few reports describing the clinical course of tandem thoracic and lumbar spinal stenosis [9,10]. But Triple-region spinal stenosis (TRSS) has largely been unreported till now. Decision making about the operative management in TRSS can be very challenging when all three stenotic levels are symptomatic.
Literature gives some guidelines about staged/simultaneous decompression procedures in TSS. Eskander MS, et al. in their study of difference between simultaneous or staged decompressions for combined cervical and lumbar stenosis showed that in mean follow up of 7 years, both groups improved in JOA and ODI without significant difference between 2 operative groups [11]. Kikuike K, et al. stated that more is the physiological age of the patient and longer is the duration of symptoms, less satisfactory is the functional outcome in surgeries for tandem stenosis [8]. Though they spoke about stenosis of two regions, the verdict becomes even more valuable when 3 regions are to be operated. Operative time and blood loss could be very significant and can be life threatening in an old patient with co-morbidities, the most common strata presenting with advanced spinal degenerative changes. In the only documented case of TRSS as per our knowledge, Joseph C. Schaffer, et al. reported a case with a severe C5-T1 stenosis, T9-T11 stenosis, and L4-L5 stenosis. They decompressed all the levels simultaneously in the same sitting and reported blood loss of around 600 ml with uncomplicated recovery of the patient [4]. At our centre we performed staged decompression procedures for most symptomatic regions first, for all 5 patients. Due to the complex clinical picture, it is always difficult to point out the most symptomatic levels in a patient in whom all 3 levels are symptomatic.
To determine the regions to be decompressed, we focused on 5 key clinical features-
1. History of clauducation at presentation &Lower limb radiating pain,
2. Un-equal upper and lower limb hyper-reflexia,
3. Un-equal upper and lower limb spasticity,
4. Grip release test and fine motor activities of hand.
These clinical features along with the radiological features were relied upon for the decision making. Most important factor for moving to second stage surgery of the remaining region was patient's clinical improvement. If patient improved clinically and was happy with his improvement/status quo, he was kept under closed watch and next stage of surgery was not carried out. Main concern behind the staging of the procedure was to avoid the risk of putting the patient through a long and extensive surgery. It also was beneficial to observe the patient post-operatively so that if the recovery is significant, the second surgery could be avoided. Out of 5 patient, 2 patients improved post-operatively, so second stage surgery was not carried out. Symptoms worsened in two patients so they were subjected to surgery, one patient succumbed to respiratory failure post-operatively.
With this case series, we have tried shed some light on existence of Triple region spinal stenosis. The purpose is not to put forth any guidelines of managemnt since it comprises of only 5 cases. Also, it is difficult to make generalized recommendations since patient's general condition may or may not allow simultaneous decompressions and surgeon's clinical judgment in planning a staged procedure plays a great role. More attention in form of larger studies for management of TRSS, one of the most complex degenerative spinal pathologies is the need of the hour for enlightening the spine surgeons.