Suprasellar Arachnoid Cysts (SAC) are rare heterogenous entities that can be diagnosed and treated prenatally or postnatally, depending on their type and symptoms. We report a case of a prenatally diagnosed suprasellar arachnoid cyst treated postnatally.
The cyst was diagnosed on a routine ultrasound at 22 weeks of gestation. It was a very large cyst in the prepontine region, compressing the brain stem and the 4th ventricle, causing a ventriculomegaly. The cyst was rapidly evolutive in the ultrasounds and the MRI of the 29th week which showed difficult access to treat the cyst antenatally.
It then became symptomatic at 30 weeks with episodes of bradycardia, independent to the uterine contractions, leading to deliver the baby despite the prematurity by C-section.
Though well tolerated postnatally, the cyst continued to grow. Progressive ventriculomegaly that had started prenatally was monitored; it allowed us to perform a ventriculo-cysto-cisternostomy on the 5th day of birth. Despite progressive reduction of cyst, residual brainstem compression lead us to perform a transient extrathecal internal shunting.
SAC are rare lesions without a consensus for treatment. The numerous case series and reports allow a better theoretical understanding of the disease but cannot predict the best practical type or time for treatment, especially with the dynamic effect due to their size, that caused a hydrocephalus in our case.
Our case suggests that these cysts require a continuous management. We should adapt to the anatomy, the rapidity of evolution of the cyst and the symptoms to determine the best timing to treat the patient, whether it is before or after birth.
Arachnoid cyst, Prenatal diagnosis
Suprasellar Arachnoid Cysts (SAC) are rare heterogenous entities that account for 9% to 21% of all pediatric arachnoid cysts [1].
They seemingly develop from a splitting of the arachnoid membrane when the basilar artery pierces it, in the prepontine cistern, creating a slit-valve mechanism from the CSF going upwards from the 4th ventricle and the foramina of Luschka, making them grow [2].
Their classification is still discussed in several reports; there has been a radiological and anatomical classification proposed by Miyama, et al. [3] without taking into account their clinical aspects. However, the classification proposed by Andre, et al. takes into account their pathophysiological origin, their anatomy and their clinical repercussions [1] (Figure 1, Figure 2 and Figure 3).
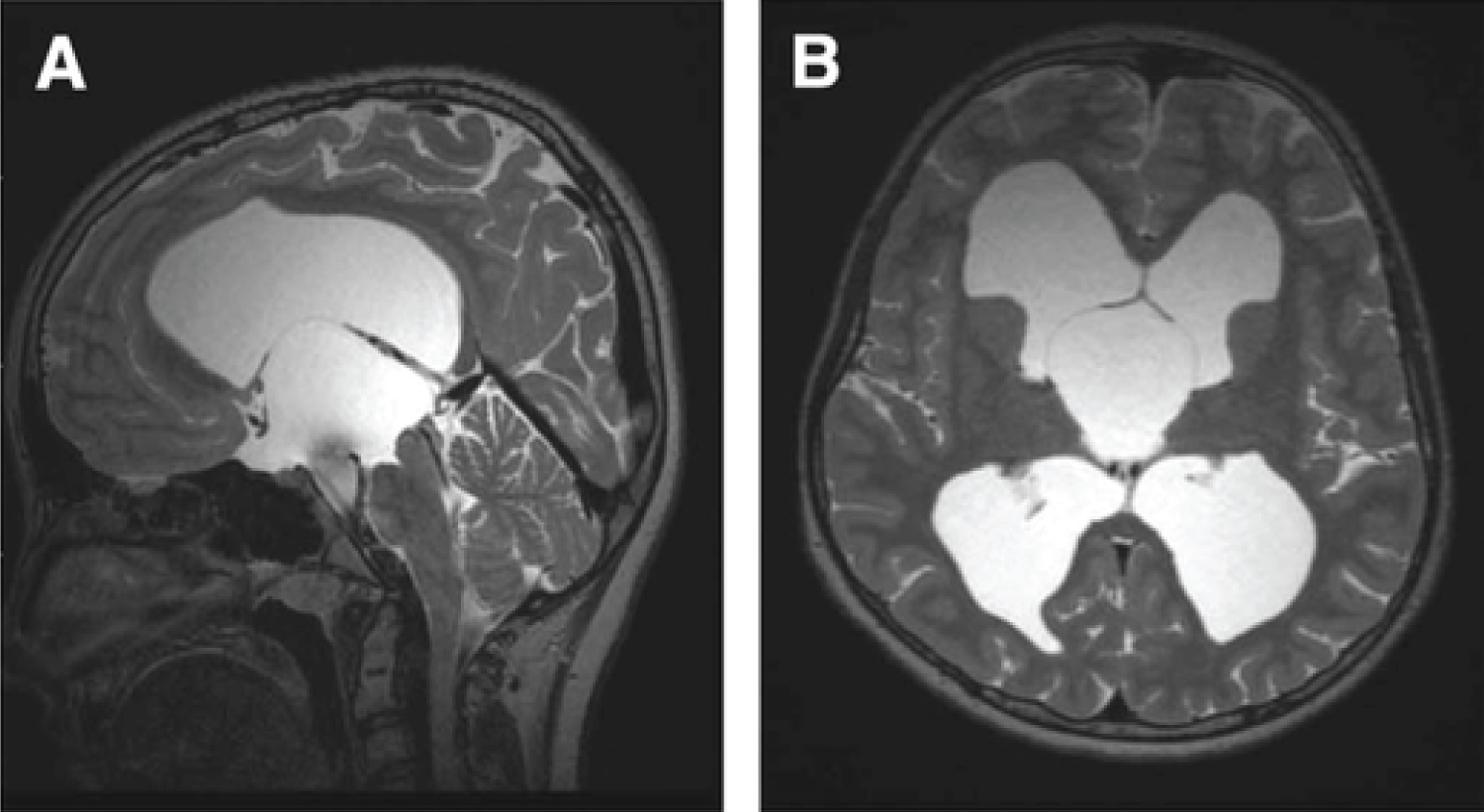 Figure 1: SAC - 1 come from an expansion of the diencephalic leaf of the membrane of Lilliequist towards the third ventricle, causing a CSF blockage by obstructing the foramina of Monro. They cause a rapid hydrocephalus and need a surgical treatment.
View Figure 1
Figure 1: SAC - 1 come from an expansion of the diencephalic leaf of the membrane of Lilliequist towards the third ventricle, causing a CSF blockage by obstructing the foramina of Monro. They cause a rapid hydrocephalus and need a surgical treatment.
View Figure 1
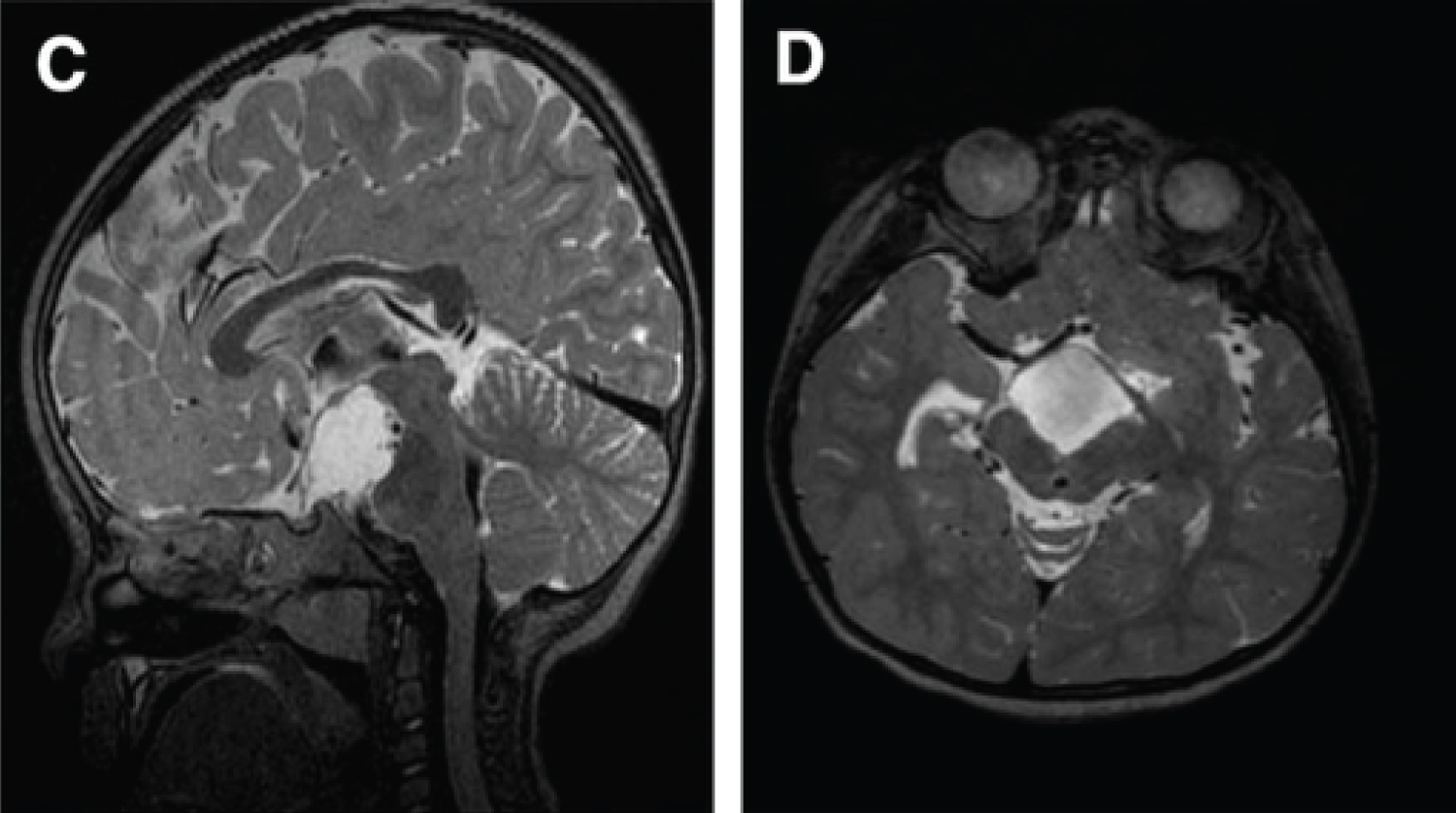 Figure 2: SAC - 2 come from a defect of the mesencephalic leaf of the membrane of Lilliequist, causing a dilatation of the interpeduncular cistern without a hydrocephalus but with a compression of the upper part of the brainstem. They are often diagnosed antenatally and do not always require surgery. However, they tend to cause endocrine disorders due to the mass effect.
View Figure 2
Figure 2: SAC - 2 come from a defect of the mesencephalic leaf of the membrane of Lilliequist, causing a dilatation of the interpeduncular cistern without a hydrocephalus but with a compression of the upper part of the brainstem. They are often diagnosed antenatally and do not always require surgery. However, they tend to cause endocrine disorders due to the mass effect.
View Figure 2
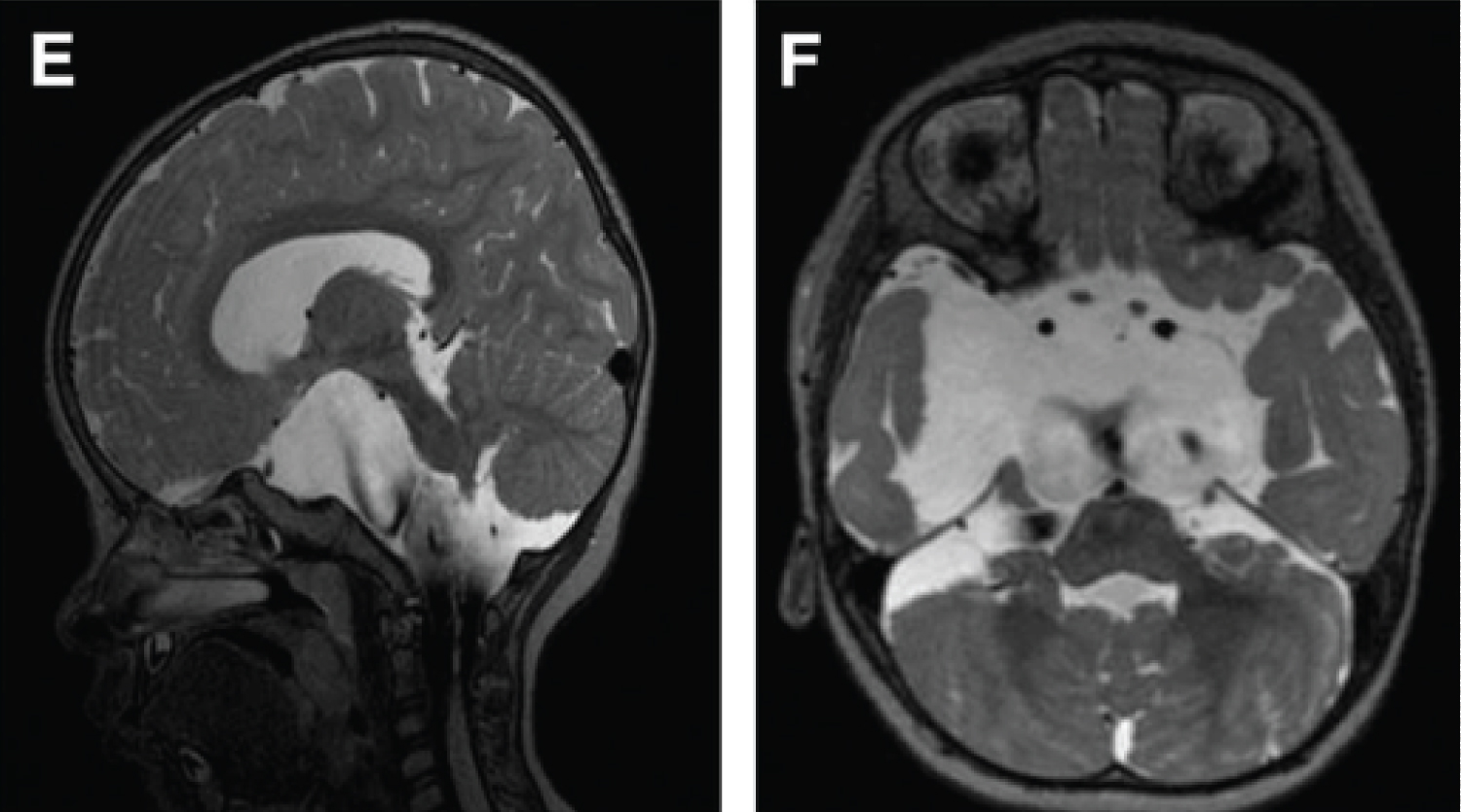 Figure 3: SAC - 3 are asymmetric and secondary to dilatation of other subarachnoid spaces; they are usually more lateral. They present with macrocrania, can cause a mild or no hydrocephalus and do not cause any endocrinological disorders. They can be observed or surgically treated.
View Figure 3
Figure 3: SAC - 3 are asymmetric and secondary to dilatation of other subarachnoid spaces; they are usually more lateral. They present with macrocrania, can cause a mild or no hydrocephalus and do not cause any endocrinological disorders. They can be observed or surgically treated.
View Figure 3
These cysts can thus be diagnosed prenatally or postnatally, depending on their type and symptoms.
The clinical characteristics range from hydrocephalus, macrocrania, developmental delay, ophthalmologic/oculomotor disturbances, endocrine perturbations of epilepsy [1].
The gold standard of imaging is the MRI, once the cyst has been seen on an ultrasound, because it allows to have a better understanding of the underlying anatomy and classify the cyst.
The differential diagnoses are other non-neoplastic cysts as described by Iqbal, et al. [4] (Table 1).
Table 1: Tissue and anatomical origin of non-neoplastic sellar region cysts. View Table 1
However, there have been case reports of germ cell tumors or ecchordosis physaliphora mimicking a SAC [5,6]. Also, an aqueductal stenosis can mimick the presence of a supra-sellar cyst in the prepontine region, as described by Wang, et al., [2] when the capsule is not visible (ref) (Figure 4).
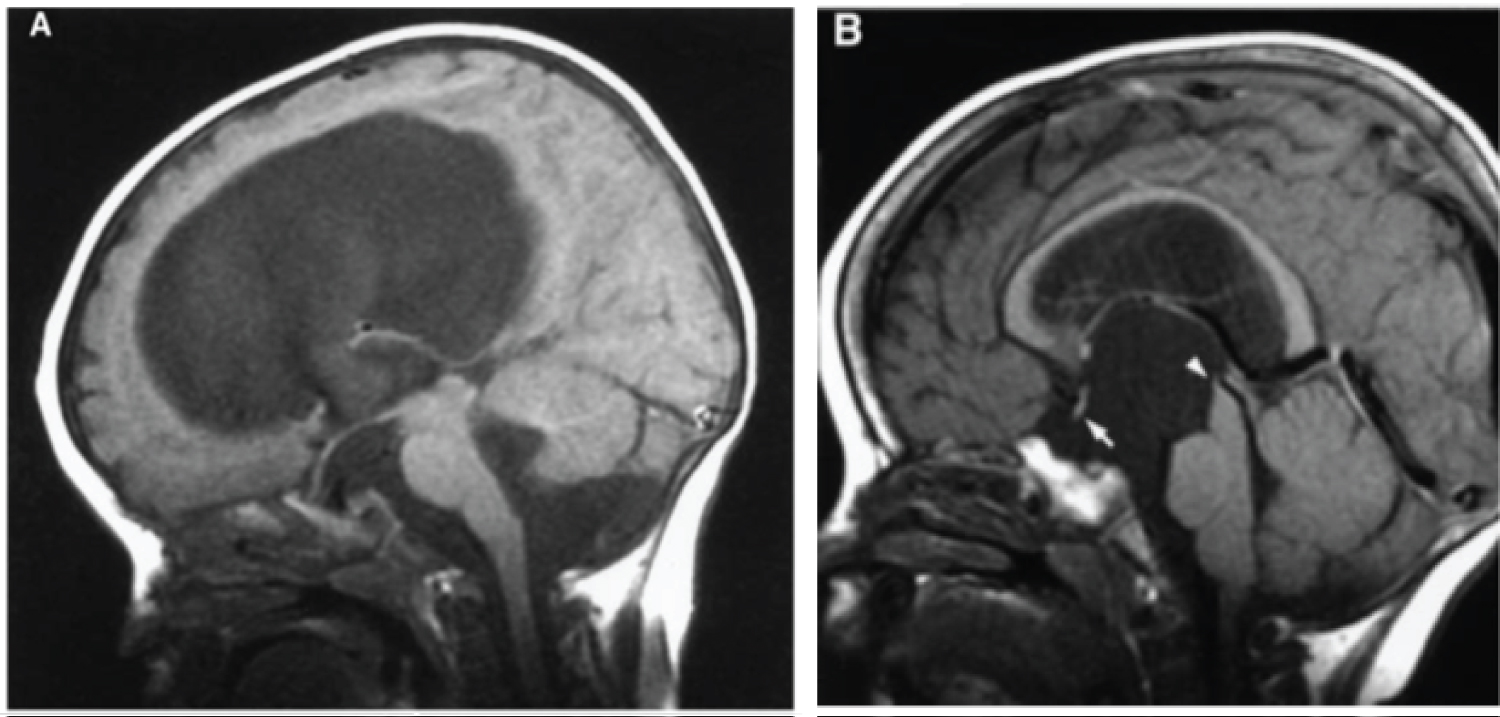 Figure 4: They have described criteria to differenciate the cysts when the capsule if not visible from an aqueductal stenosis [2]: vertical optic chiasm, upward mamillary bodies, flattening of the pons.
View Figure 4
Figure 4: They have described criteria to differenciate the cysts when the capsule if not visible from an aqueductal stenosis [2]: vertical optic chiasm, upward mamillary bodies, flattening of the pons.
View Figure 4
Indeed, it is essential to diagnose them to offer the best treatment.
There is no clear consensus regarding their management. Some SAC can be observed and never treated (usually SAC-3), as described by Peterson, et al. in their review of the literature [7].
Historically, these cysts were treated by cystoperitoneal shunting. However, the endoscopic treatment has overtaken open or stereotactic surgeries.
Ventriculo Cystocisternostomy (VCC) with a fenestration of the rostral and caudal membranes or an open surgery with marsupialization of the cyst are the most applied. The experience of endoscopic treatment of all arachnoid cysts published by Oertel, et al. [8], where they had 21% of SAC, showed that among all procedures, ventriculocystostomies and ventriculocystocisternostomies were the most successful treatments. Other reports by Maher, et al., Ozek, et al. and Decq, et al. confirm that VCC is the best treatment [9-11].
We report a case of a prenatally diagnosed suprasellar arachnoid cyst treated postnatally.
The cyst was diagnosed on a routine ultrasound at 22 weeks of gestation. It was a very large cyst in the prepontine region, compressing the brain stem and the 4th ventricle.
We classified it as a SAC-2 cyst with SAC-1 characteristics.
The cyst was rapidly evolutive in the ultrasounds, leading us to conduct a foetal MRI on the 29th week which showed the large cyst, its compression on the brain stem and 4th ventricle, without a ventriculomegaly and no other cerebral anomalies (no sign of parenchymal ischaemia, no morphologic anomalies).
The mother was then hospitalized because of a threat of premature delivery, with episodes of bradycardia even after tocolysis, which made us suspect that cyst was the cause of the symptoms.
We had a multi-disciplinary discussion with the teams in charge (gynecology and obstetrics, radiopediatrics, pediatrics) and because of the gravity of the symptoms, we decided to deliver the baby despite the prematurity by C-section, at 35 weeks + 2 days, without any complications.
The successive transcranial ultrasounds showed a progressive dilatation of the ventricles compared to the MRI before birth. However, the baby tolerated the gradually increasing intracranial pressure well.
We realized another MRI that showed an asymmetric ventriculomegaly (prevailing on the left side) and a dilatation of the foramen magnum. With this favorable anatomy, we decided to perform a ventriculocystocisternostomy on the 5th day of life.
The MRI after surgery showed a decrease in the size of the ventricles. Unfortunately the ventricles continued to dilate and on the MRI of the 19th day of life, there was a stability in size of the cyst but also a clear tetraventricular hydrocephalus due a residual mass effect on the ambiens cistern and the pons.
We then decided to place a ventriculoperitoneal shunt.
The next MRI showed a reduction of the size of the ventricles and an absence of mass effect of the cyst. The patient was discharged on day....
The follow-up MRIs showed a normal size of the ventricles, a decrease in size of the cyst and a patency of the stomy. One of those MRIs showed a migration of the proximal catheter, under the skin, without any consequence on the size of the ventricles or cyst. We then removed the VP shunt.
The patient has a normal psychomotor development. The last clinical check-up was at 1 year and a half and the cyst and ventricles are stable. A long-term follow-up is planned.
SAC are rare benign lesions without a consensus for management. Depending on their type and size, several clinical repercussions can be found and therefore, their management can go from a simple radiological follow-up to surgery/ies, as described by Di Rocco, et al. [12].
The main issue is the best time to treat them.
The classification created by Andre, et al. [1] that we chose to use, allowed to consider the cyst as a SAC-2 lesion with SAC-1 characteristics (hydrocephalus, by a mechanical origin). It allowed a better understanding of the disease, a better preparation to treat the case and prevent complications.
In 2010, Gedikbasi, et al. [13] had reported all cases of existing prenatal diagnosis of SAC and their treatment [13]. Among the 6 cases, none of them was treated before birth.
There was only one case of induced birth (polyhydramnios secondary to the cyst); of all the other births, there were 3 cesarean deliveries for obstetric reasons.
There were 2 cystoperitoneal shunts, 3 cases of VCC and one case of combined treatment.
The global outcome was favourable in all cases.
However, they have described that the MRI was only an adjunct to the global management, which was best with the ultrasound. In our case, the MRI was essential for the diagnosis and the planning.
The common factor of all these cases is that the reasons to treat the patients were not the antenatal diagnosis but the evolutivity of the cysts.
In our case, we have also treated the cyst only when it was symptomatic.
Our case suggests that suprasellar arachnoid cysts require a continuous management from the diagnosis. The MRI is essential to classify the cyst and foresee the possible treatment options and complications. Nevertheless, we should adapt to the anatomy, the rapidity of evolution of the cyst and the symptoms to determine the best timing to treat the patient, regardless of if it is before or after birth.
Finally, their management needs a multidisciplinary approach with obstetricians, neonatologists, neuroradiologists and neurosurgeons.