We present a rare cause of increased Intracranial Pressure (ICP) and papilloedema in a male adult. The presenting symptoms of blurred vision and headaches were investigated with brain imaging which revealed an intradiploic epidermoid cyst, extending intracranially compressing the torcular Herophilli.
Epidermoid cyst, Torcular herophilli, Papilloedema, Calvarial lesion, Visual symptoms
Presence of papilloedema should trigger cranial imaging to look for causes of raised intracranial pressure.
Obstruction of the venous sinuses flow is a recognized cause of raised intracranial pressure. Most commonly it is due to thrombosis. It has been described compression by tumours, causing obstruction of the sinuses flow. Usually metastatic deposits are responsible for that kind of compression [1]. In our case the compression on the venous sinuses is due to a calvarial epidermoid cyst.
Intraosseous epidermoid cysts can occur at any site of the calvarium [2,3]. Most commonly, they are congenital and they are observed in children or young adults [4]. Occipital intraosseous epidermoid cysts represent a rare location of development of these lesions [5]. It is even more rare to cause increased ICP because of compression on an intracranial venous sinus. To the best of our knowledge, this is the only case reported, of an adult having increased ICP accompanied by visual symptoms, because of a calvarial epidermoid cyst causing compression on the torcular Herophili.
In our case, a 44-year-old male presented to his GP with intermittent headache for the last two years and a lump at the area of the external occipital protuberance, but since October 2019, he started having blurred vision bilaterally. The GP attempted to excise the lump in his surgery, but because of profuse bleeding, he had to stop. Following this attempt and because of the visual symptoms the patient was referred for a formal ophthalmology assessment, which revealed bilateral optic disc swelling and VA 6/9 in both eyes. Subsequently, he had an MRI/MRV, which showed that the lump was an intraosseous lesion, extending intracranially, causing compression on the torcula. The lesion had characteristics of epidermoid cyst. Apart from the palpable mass, the optic disc swelling and the VA 6/9, there were no other findings on the clinical examination. The patient was discussed at the neuro-oncology MDT and the outcome was surgical treatment, as the lesion was compromising patient's vision. The patient underwent an elective operation for excision of the lesion found on the MRI. Intraoperatively, as demonstrated on the imaging the lesion had thinned out the outer and inner table of the skull, so directly under the skin incision we encountered the mass. The content of it appeared to be consistent with epidermoid cyst. After reaching the deepest part of the cyst and excising the capsule, we ended up in the posterior fossa extradurally, as expected according to the imaging. The specimen was sent for histology, which confirmed the findings of an epidermoid cyst. Post-operatively the patient remained neurologically stable and his blurred vision resolved.
Calvarial epidermoid cysts are most commonly seen in children or young adults [6]. Extradural lesions have been reported in the fontanels, periorbital, nasal, frontotemporal, eustachian tube, parietal, occipital, cavernous sinus, and petrous apex locations [7]. Although most of the calvarial cysts are asymptomatic, the skull epidermoid cysts that extend intracranially can present with symptoms of increased ICP due to mass effect, with aseptic meningitis due to rupture of the cystic content, seizures, infection or abscess if the cyst gets infected [8].
Epidermoid cysts become symptomatic in early age usually, in childhood, second or third decade of life [9]. Large calvarial epidermoid cysts can cause symptoms because of mass effect [10], but in our case, the patient became symptomatic because of direct compression on the torcular Herophilli, resulting in partial occlusion of the sinuses, causing increased intracranial pressure. There have been described calvarial epidermoids in occipital midline, in children, without any symptoms/signs of increased ICP though [11]. Also, going through the literature, there are intracranial epidermoids in adults, causing compression on the Superior Saggital Sinus (SSS), but no intraosseous epidermoids, extending intracranially [12]. To the best of our knowledge this is the first case reported of an intraosseous epidermoid cyst, in an adult, extending intracranially causing compression on the venous sinuses, resulting in increased ICP and subsequently visual symptoms.
In our case, the patient was an adult, diagnosed with a palpable mass at his occiput, which was proven to be an intraosseous epidermoid cyst, compressing on the confluence of the sinuses, causing increased ICP and visual symptoms and papilloedema. It is advisable for scalp lesions, especially overlying important anatomical structures, to perform brain imaging, before attempting excision (Figure 1, Figure 2, Figure 3 and Figure 4).
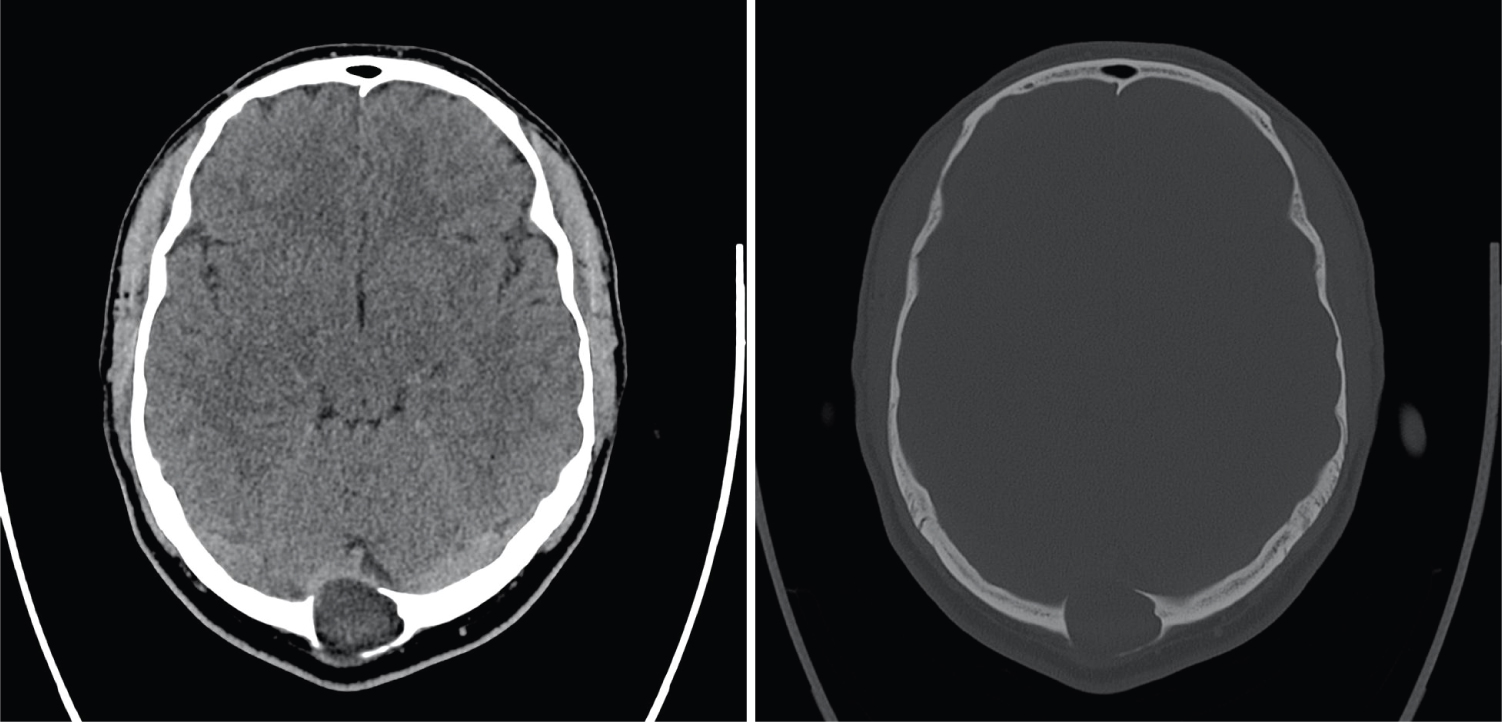 Figure 1: Axial CT. A) Hypodense intra-osseous lesion at the level of the torcula; B) Image at the same level with reconstruction in bone algorithm clearly shows the expansile nature of the lesion with thinning of both the internal- and external table of the skull.
View Figure 1
Figure 1: Axial CT. A) Hypodense intra-osseous lesion at the level of the torcula; B) Image at the same level with reconstruction in bone algorithm clearly shows the expansile nature of the lesion with thinning of both the internal- and external table of the skull.
View Figure 1
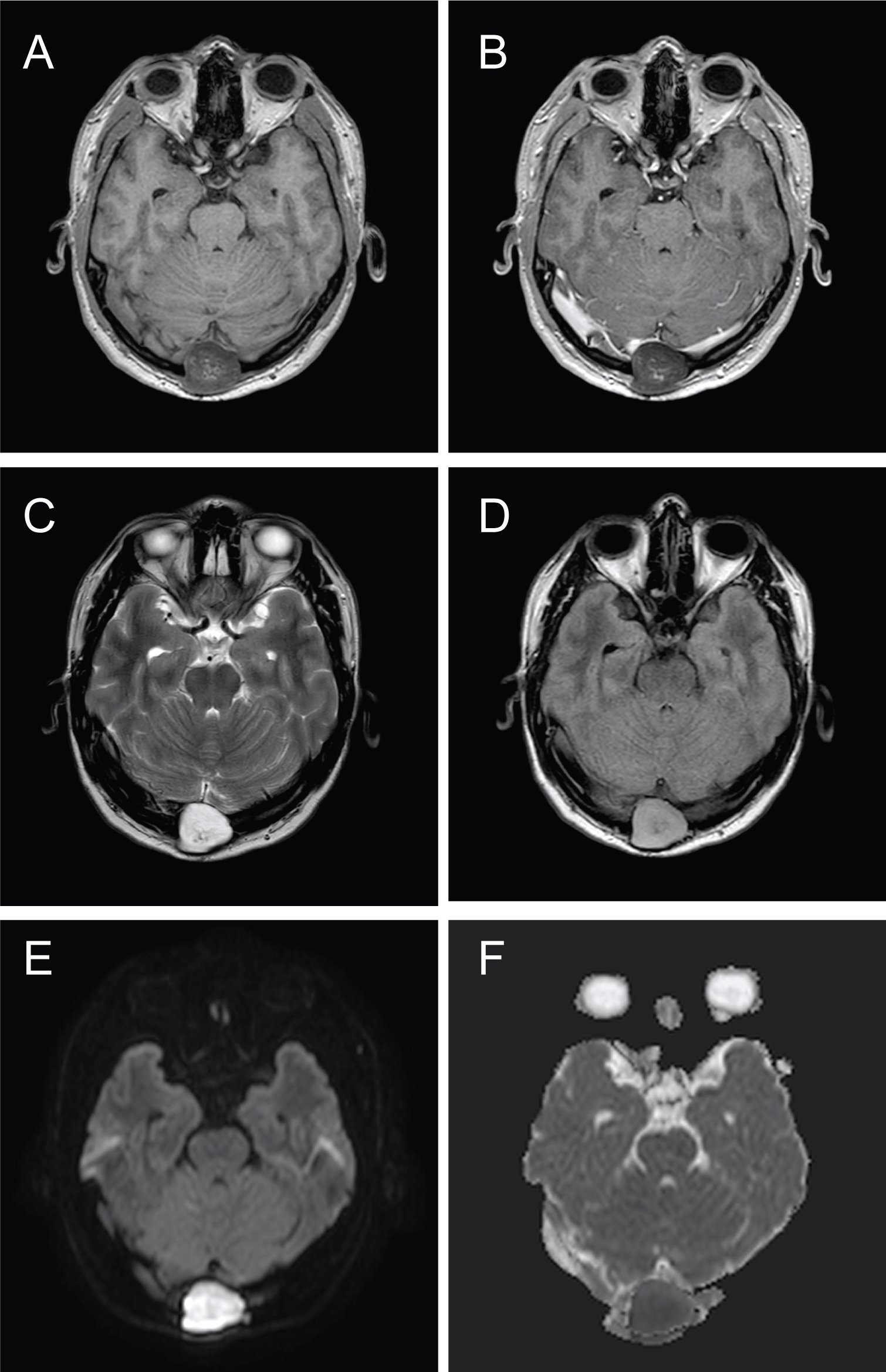 Figure 2: Axial MRI shows typical features of epidermoid. Mixed signal lesion on T1 (A). No enhancement after injection of gadolinium (B). Predominantly high signal on T2 (C). Slightly heterogenous signal on the T2 flair, higher than cerebrospinal fluid (D). Striking high signal on the diffusion weighted images (DWI) (E) with corresponding low signal on the apparent diffusion coefficient (ADC) map (F) consistent with restricted diffusion.
View Figure 2
Figure 2: Axial MRI shows typical features of epidermoid. Mixed signal lesion on T1 (A). No enhancement after injection of gadolinium (B). Predominantly high signal on T2 (C). Slightly heterogenous signal on the T2 flair, higher than cerebrospinal fluid (D). Striking high signal on the diffusion weighted images (DWI) (E) with corresponding low signal on the apparent diffusion coefficient (ADC) map (F) consistent with restricted diffusion.
View Figure 2
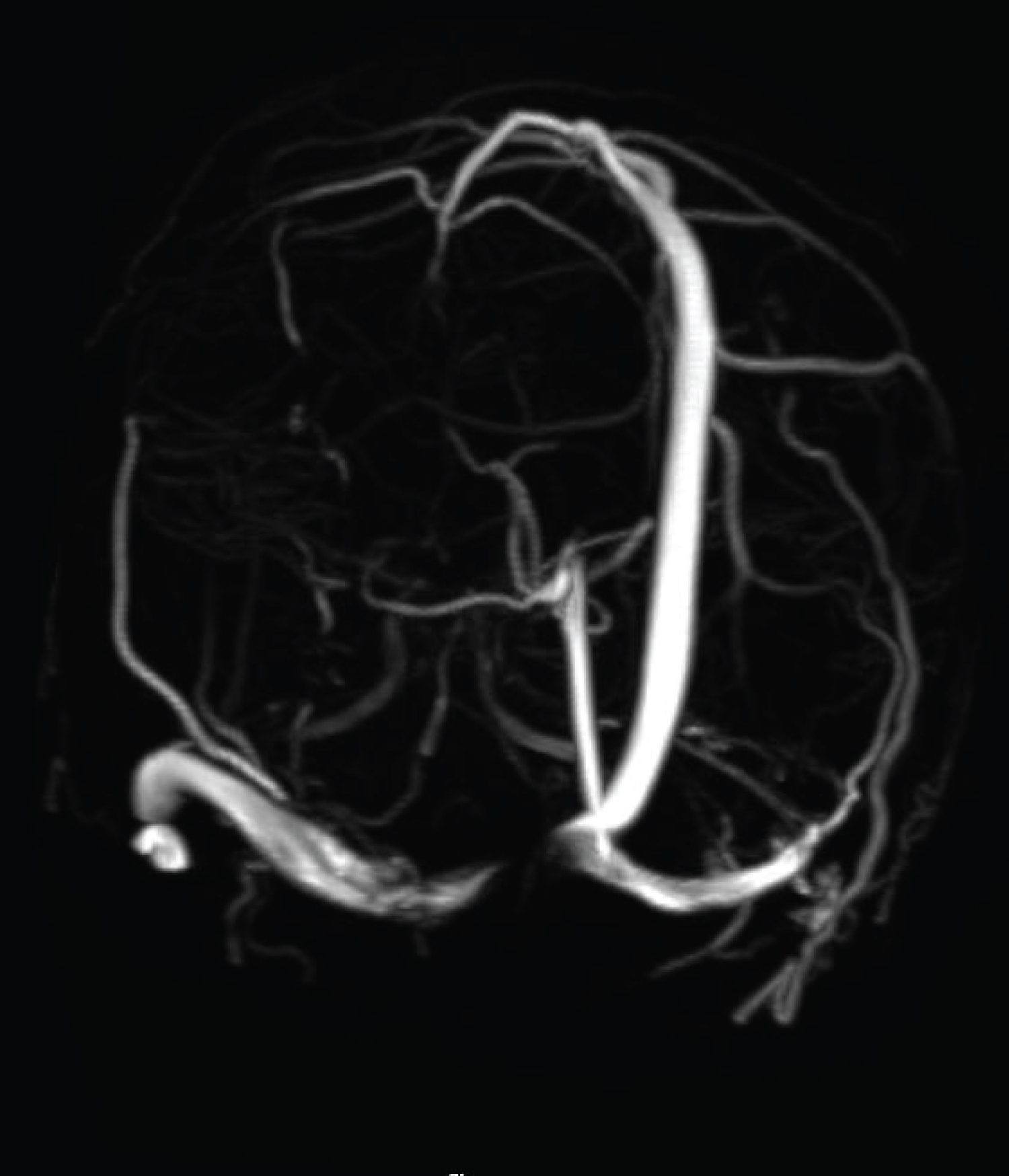 Figure 3: 3D MR venogram time-of-flight shows interruption of the normal flow in the right proximal transverse sinus due to compression of underlying intraosseous epidermoid. Note normal straight sinus.
View Figure 3
Figure 3: 3D MR venogram time-of-flight shows interruption of the normal flow in the right proximal transverse sinus due to compression of underlying intraosseous epidermoid. Note normal straight sinus.
View Figure 3
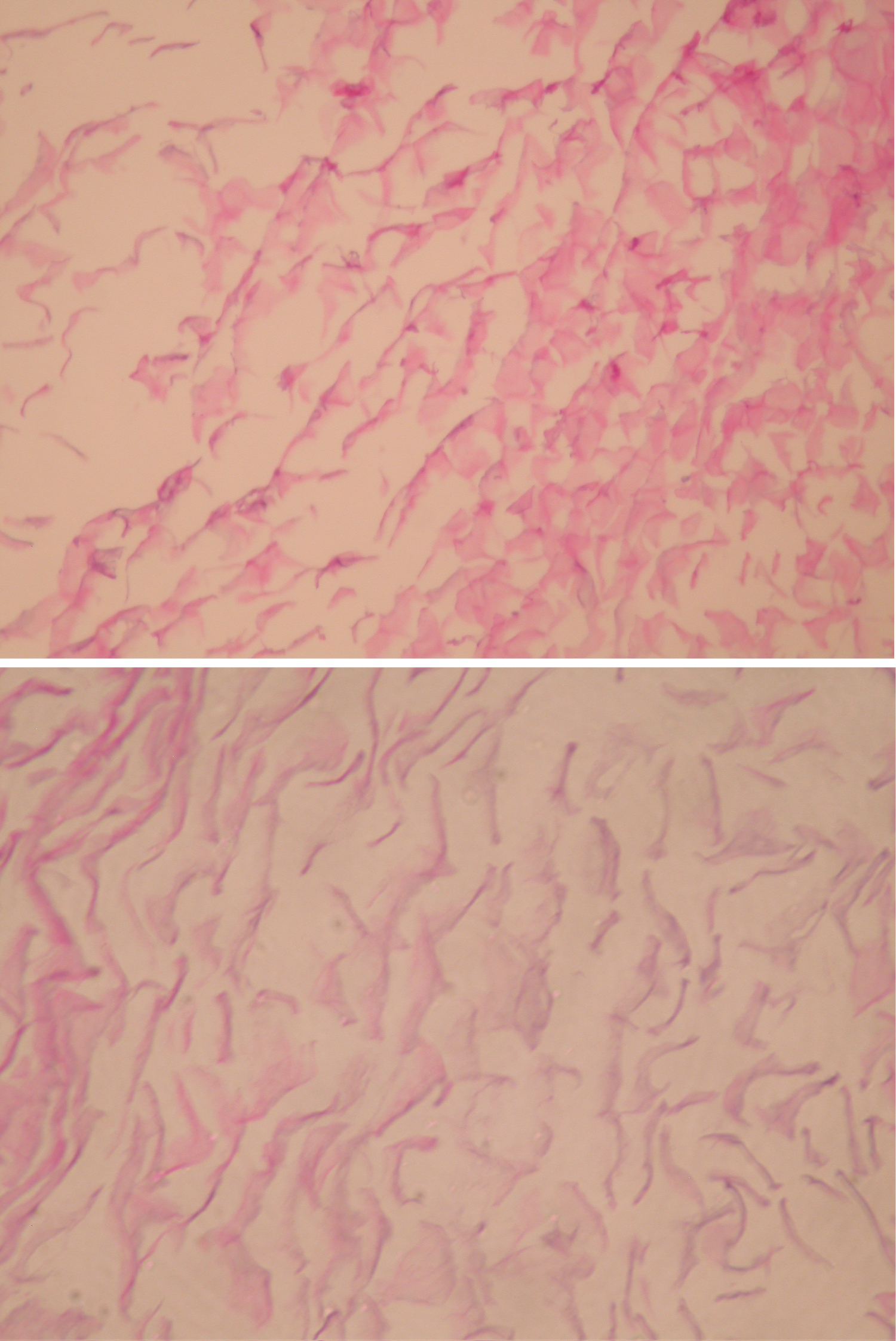 Figure 4: Original magnification ×200, haermatoxylin and eosin stain, showing keratin flakes in keeping with the contents of an epidermoid cyst.
View Figure 4
Figure 4: Original magnification ×200, haermatoxylin and eosin stain, showing keratin flakes in keeping with the contents of an epidermoid cyst.
View Figure 4