Thrombosis of cerebral artery, Fibrinolysis, Clip reposition, Clip reposition, Iatrogenic complication
CT: Computed Tomography; MCA: Middle Cerebral Artery
The most common complication of intracranial aneurysms clipping is brain ischemia, which is observed in 5.6% of patients with unruptured cerebral aneurysm [1,2]. Brain infarction is primarily observed within the first 24 h after clipping and associated with vasospasm, thrombosing of the feeding artery, and/or migration of an atheromatous plaque after manipulations with an aneurysm [3]. Factors increasing the risk of postoperative complications are complex aneurysms, atherosclerosis, and calcification of the aneurysm neck [1,2].
A rare cause of brain infarction in the early postoperative period may be improper clip position with compression of parentartery [2,3]. Micro-Doppler or other intraoperative methods of blood circulation control can help reduce the risk of such complications [4]. Reoperation with a microsurgical resolution of stenosis can improve the outcome in patients with iatrogenic complications associated with improper clip positioning [5].
The presented clinical case demonstrates a successful early diagnosis of artery occlusion after aneurysm clipping and resolution of thrombosis during urgent reoperation by intracranial intra-arterial injection of a fibrinolytic agent.
Patient F, male, 43-years-old, presented with a subarachnoid hemorrhage. CT angiography revealed an 8 mm saccular aneurysm in the trifurcation of the left middle cerebral artery (MCA) (Figure 1). When the patient's condition stabilized, he was transferred to our center for surgical treatment 30 days after the hemorrhage.
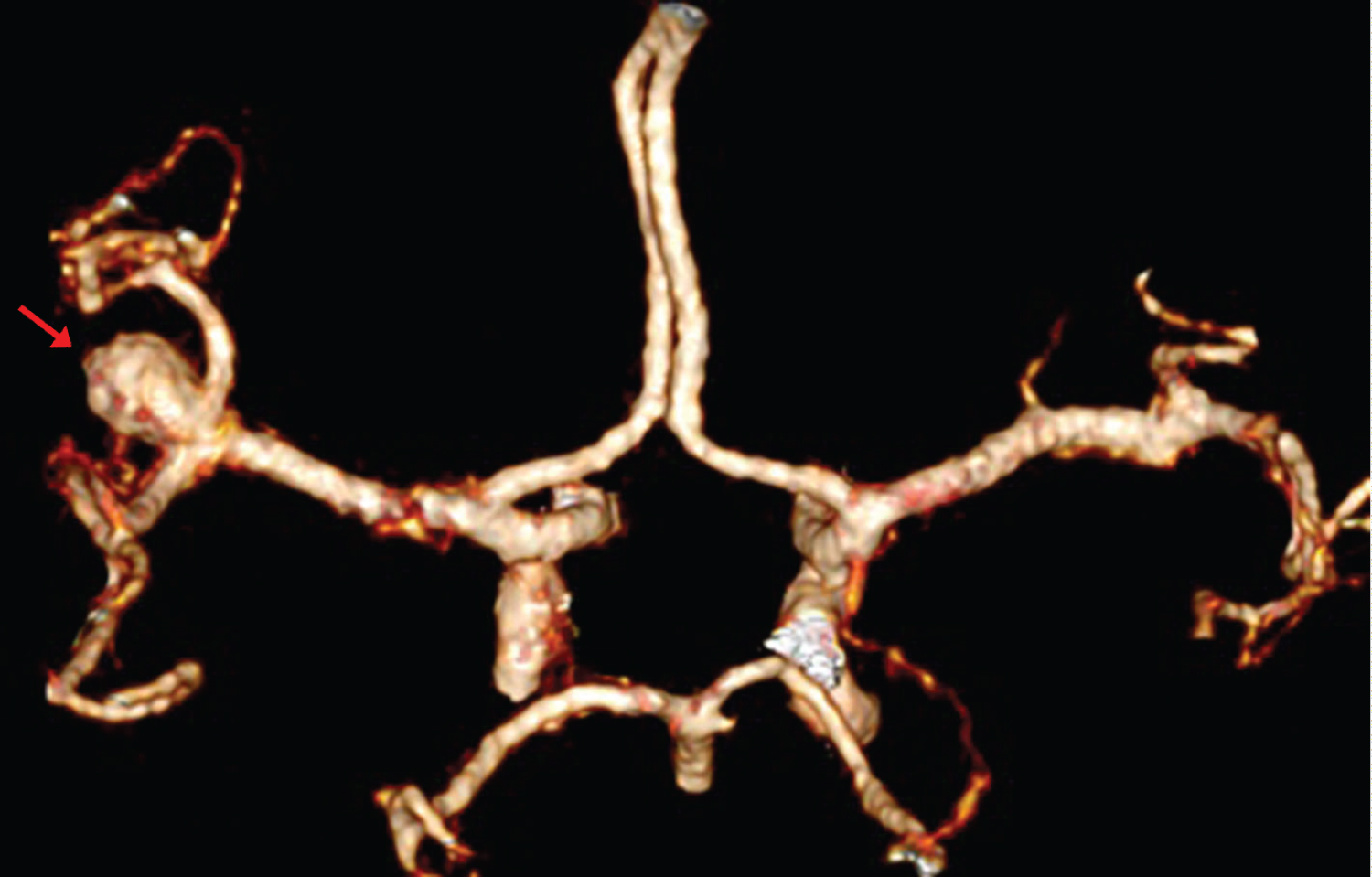 Figure 1: 3D CT-angiography of the brain revealed a middle-size aneurysm in the trifurcation of the left MCA (arrow).
View Figure 1
Figure 1: 3D CT-angiography of the brain revealed a middle-size aneurysm in the trifurcation of the left MCA (arrow).
View Figure 1
The patient's condition was satisfactory at admission. No cerebral neurological symptoms were detected. The patient underwent microsurgical clipping of the aneurysm neck in the trifurcation of the left MCA. During the surgery, a middle-size aneurysm was revealed. The dissection of M2 segments and the aneurysm neck was performed. The aneurysm neck was clipped with a standard straight clip. The aneurysm dome was incised, and no bleeding was detected. Micro-Doppler showed good blood flow in two M2 segments that remained within normal values (35 cm/s). Fluorescent video angiography also verified good blood filling of M2 branches. The time of the surgical stage was 2.5 h (10:00-12:30).
When the patient awakened from anesthesia at 14:30, right-sided hemiplegia and severe aphasia were observed. CT was performed at 15:00. It did not reveal any postoperative hemorrhagic complications (Figure 2). The patient was transferred to an endovascular suite at 16:00. Cerebral angiography revealed occlusion of a large branch in the trifurcation of the left MCA.
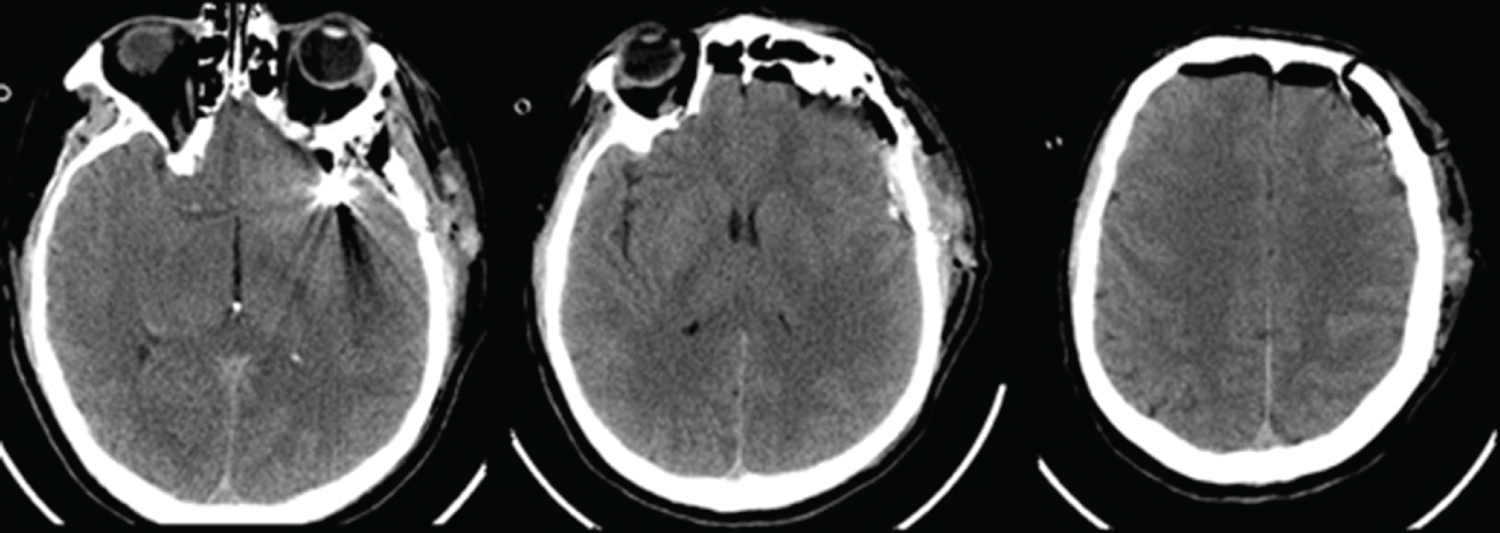 Figure 2: CT after the aneurysm surgery. There are no signs of hemorrhagic complications.
View Figure 2
Figure 2: CT after the aneurysm surgery. There are no signs of hemorrhagic complications.
View Figure 2
Urgent reoperation was started at 17:30. The patient underwent a re-exposure of an operating wound. The revision of the clipping area revealed a large M2 branch posterior to the aneurysm that was compressed by the clip. The clip reposition and release of the stenosed vessel were made. According to the micro-Doppler, there was no blood flow in the released branch because it was occluded by a blood clot. Recombinant prourokinase (100,000 IU) was injected into the branch. Restoration of blood circulation in the branch was detected in 5 min, which was verified by micro-Doppler and fluorescent video angiography (Figure 3).
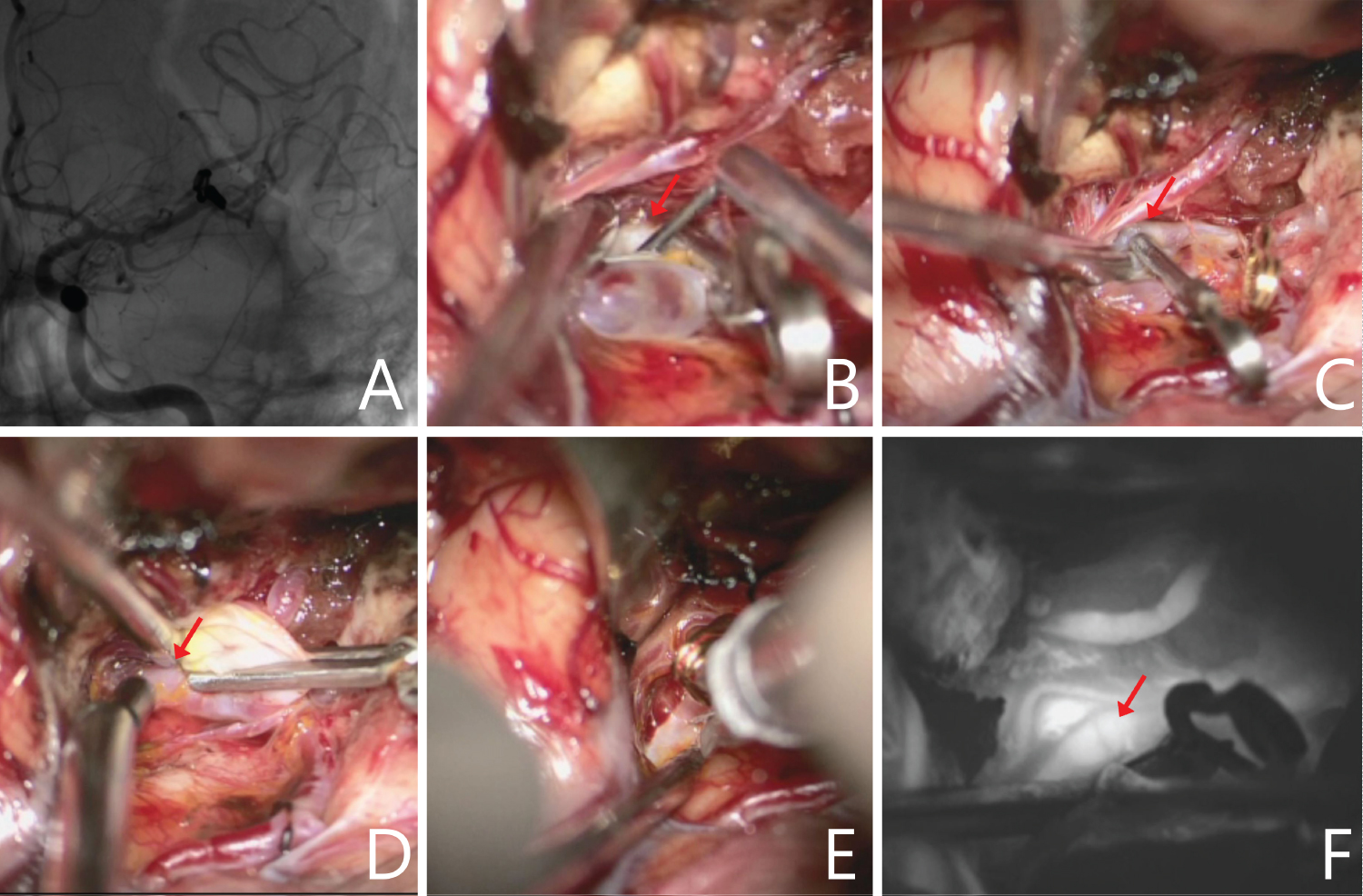 Figure 3: А) Angiography after the first operation demonstrated contrast of two M2 branches of the left MCA; B,C) Intraoperative view: Stenosis of the parietal M2 branch (arrow); D) Micro-Doppler did not reveal blood flow in the artery (arrow) after clip reposition; E) Fibrinolytic agent is injected into the lumen of the thrombosed branch; F) Video angiography showed good contrast of the artery (arrow) after the fibrinolytic agent injection.
View Figure 3
Figure 3: А) Angiography after the first operation demonstrated contrast of two M2 branches of the left MCA; B,C) Intraoperative view: Stenosis of the parietal M2 branch (arrow); D) Micro-Doppler did not reveal blood flow in the artery (arrow) after clip reposition; E) Fibrinolytic agent is injected into the lumen of the thrombosed branch; F) Video angiography showed good contrast of the artery (arrow) after the fibrinolytic agent injection.
View Figure 3
Postoperative cerebral angiography showed a good flow of three MCA branches (Figure 4). CT in dynamics revealed an ischemic focus in the left temporal area with a partial resolution (Figure 5).
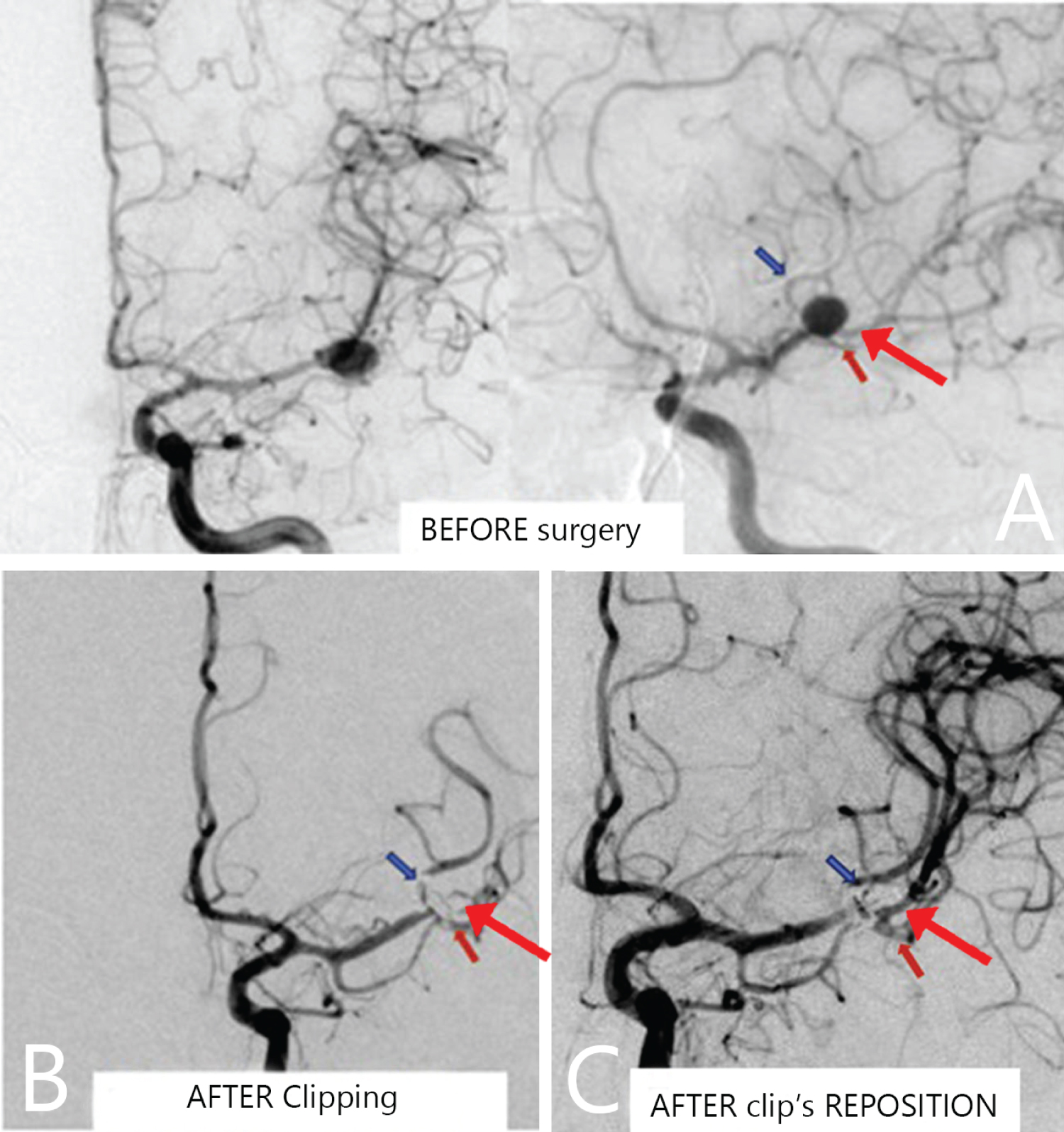 Figure 4: А) Digital subtraction angiography before surgery. An aneurysm is visualized in the M1 trifurcation of the left MCA (two large branches: frontal (blue arrow) and temporal (red arrow), and a small parietal branch (large red arrow); B) Digital subtraction angiography within 2 h after the surgery. The vascular-free area is visualized in the projection of the parietal branch of MCA; С) Digital subtraction angiography showed a good flow of the three M2 segments after the reoperation.
View Figure 4
Figure 4: А) Digital subtraction angiography before surgery. An aneurysm is visualized in the M1 trifurcation of the left MCA (two large branches: frontal (blue arrow) and temporal (red arrow), and a small parietal branch (large red arrow); B) Digital subtraction angiography within 2 h after the surgery. The vascular-free area is visualized in the projection of the parietal branch of MCA; С) Digital subtraction angiography showed a good flow of the three M2 segments after the reoperation.
View Figure 4
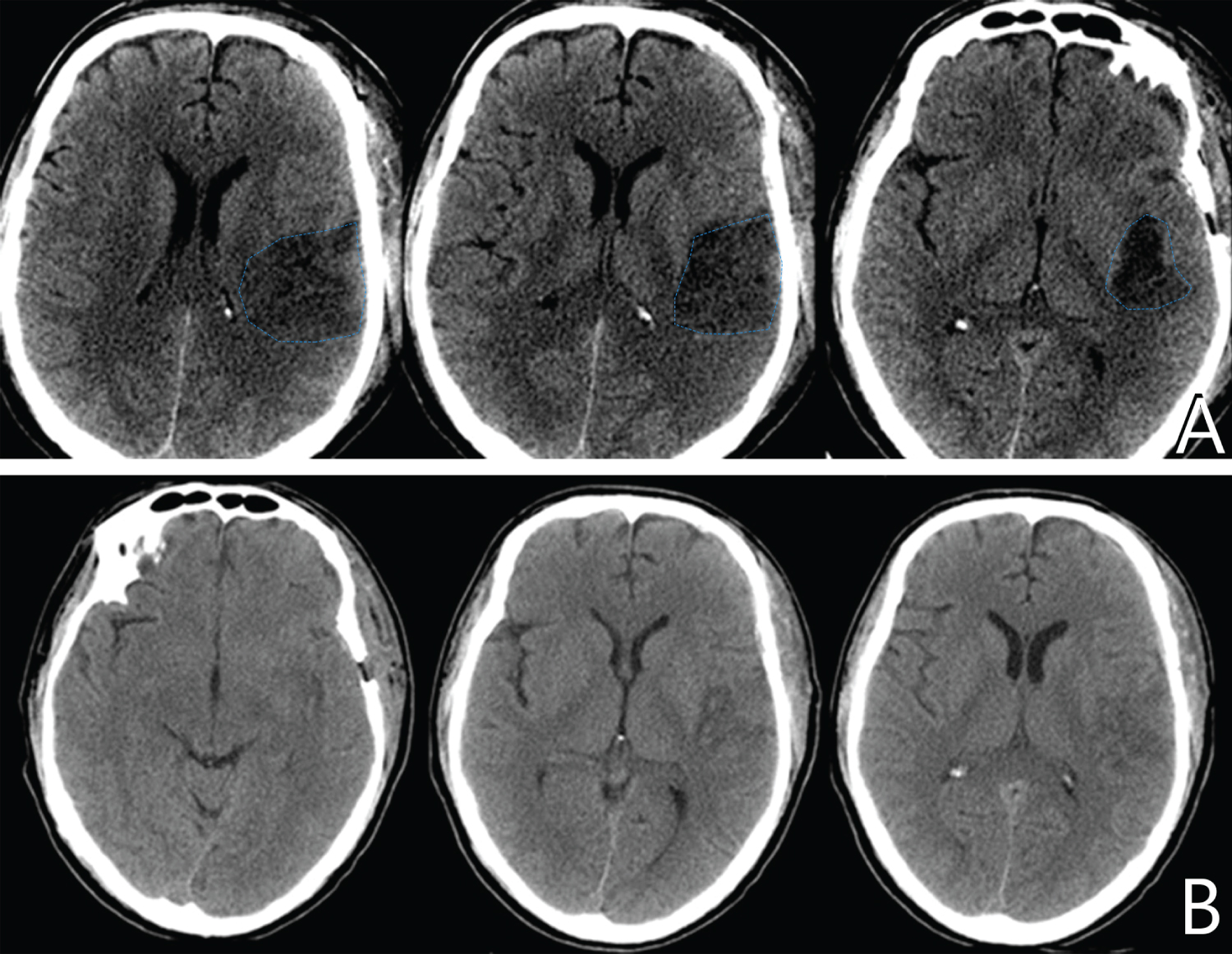 Figure 5: А) CT of the brain on the 5th day after the surgery revealed an ischemic focus in the area of the left MCA (blue contour); В) A partial resolution of cerebral ischemic alterations is observed on the 14th day after the surgery.
View Figure 5
Figure 5: А) CT of the brain on the 5th day after the surgery revealed an ischemic focus in the area of the left MCA (blue contour); В) A partial resolution of cerebral ischemic alterations is observed on the 14th day after the surgery.
View Figure 5
There was a gradual regression of neurological symptoms. The patient had light right-sided hemiparesis (scored up to 4) and light apathetic disorders manifested as paraphasias at discharge. There were no inflammatory complications or wound cerebrospinal fluid leakage.
Cerebral ischemic complications are the main causes leading to patients' disability after neurosurgical interventions. The prevalence of this complication can reach 12% [6]. About 20% of all ischemic complications are asymptomatic [5]. More often, ischemic complications result from surgical treatment of so-called “complex” aneurysms. However, the risk of vascular occlusion after clipping of small and medium-size aneurysms reaches 5.6% [2].
Early endovascular revascularization is actively applied in patients with thromboembolic strokes of the MCA region. These methods include fibrinolysis and clot retreaval [7]. In patients with acute ischemic stroke, endovascular clot retrieval is effective within 24 h after ictus for brain cell saving [8]. Some studies showed that clot retrieval could have positive results besides a 24-hour period [9]. If this concept is applied to microsurgical clipping, it can be suggested that clip reposition can lead to an improvement of neurological deficit if it is performed in the early postoperative period. Unfortunately, there are no studies that evaluated the time interval and the effectiveness of direct revascularization. However, we believe that this interval is only several hours after the onset of symptoms associated with arterial stenosis. This point of view is explained by the fact that thrombosis is progressing gradually, which reduces the chance of its effective resolution.
Early diagnostics of the cause of ischemic complications with direct cerebral angiography is a modern method applied in hybrid surgery [10]. Neurologic symptoms or vascular thrombosis in patients with stenosis can manifest not immediately but several hours later (for example, 9 h), as it was described in the clinical case presented by Goertz, et al. [5]. This is one previously published case that describes effective early reoperation in a patient with iatrogenic ischemia after aneurysm clipping in the bifurcation of the MCA. That case was similar to ours. Nine hours after MCA bifurcation, aneurysm clipping left-sized hemiparesis and aphasia developed in the patient. The patient underwent urgent CT angiography that revealed stenosis in the area of the parietal M2 branch. CT did not reveal any ischemic lesion or hemorrhage. CT perfusion showed a forming ischemic zone in the left temporal lobe. The patient underwent a second surgery 19 h after the onset of symptoms. Clip reposition was performed. After the reoperation, an improvement in the blood circulation in the temporal lobe and regression of neurological symptoms were observed. The patient was discharged in a satisfactory condition. CT visualized an infarction focus in the temporal area [5].
It should be noted that clip reposition alone can be ineffective in patients with stenosis and thrombosis. In our case, a technique of a fibrinolytic agent injection in a vascular lumen is applied (Figure 6). This method was described in 2016 [11] and is still used in our department for patients with intraoperative thrombosis during microsurgical interventions. A puncture is made by an insulin needle in the proximal area of the thrombosed vessel or aneurysm neck, and recombinant prourokinase is injected intraarterially (Figure 6). The mean dose is100,000 IU [11]. Pinpoint bleeding that developed after a puncture is stopped by cotton tamponade within 1-2 min. The restoration of the blood circulation is observed in 1-5 min after the injection of a fibrinolytic agent. The effectiveness of recanalization reaches up to 70% [11]. We have never observed postoperative hemorrhagic complications after intra-arterial intracranial injection of a fibrinolytic agent during surgery. The authors chose this method of blood flow restoration in the thrombosed artery as an alternative to endovascular fibrinolysis to reduce the time required for the repeated transportation of the patient to the endovascular suite.
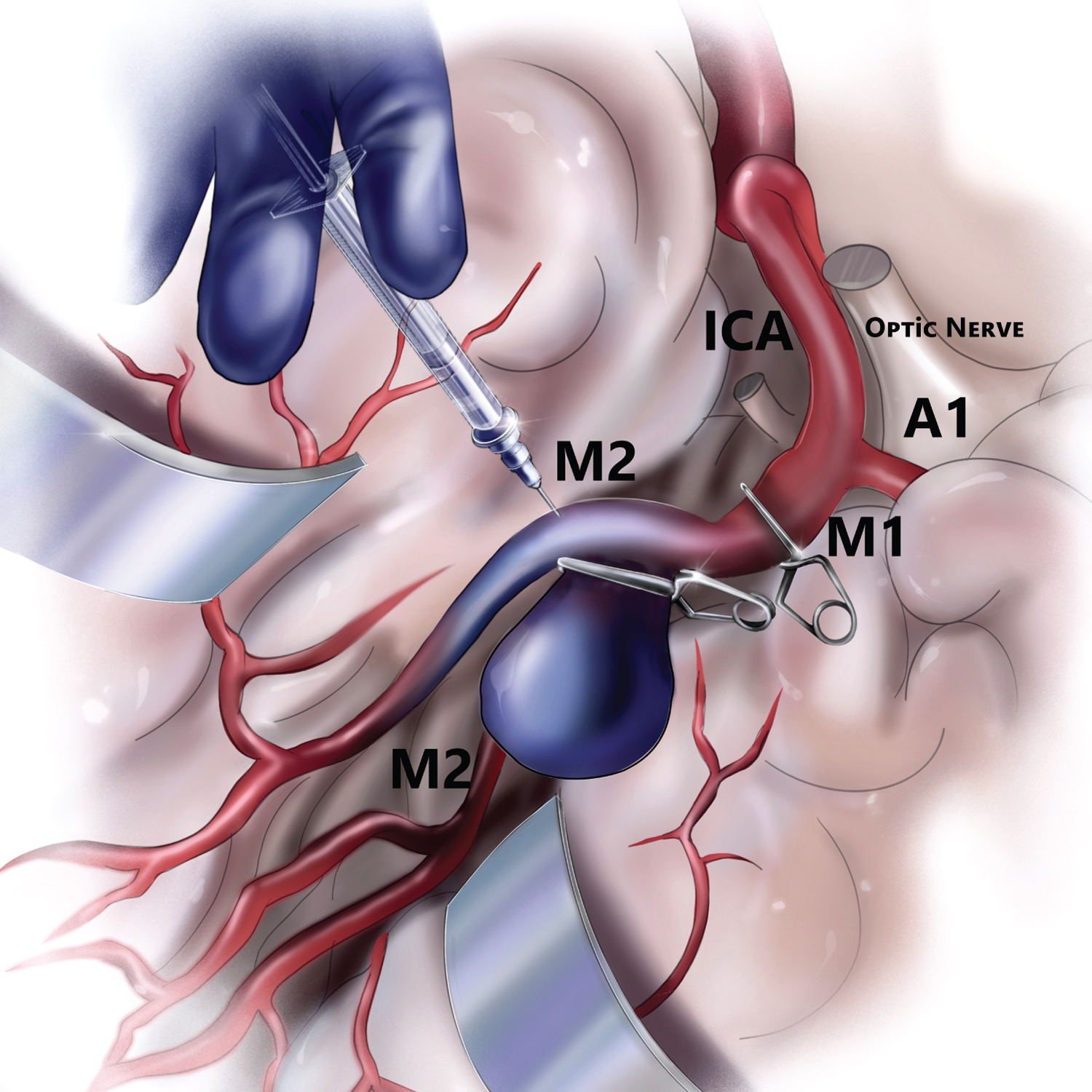 Figure 6: Injection of a fibrinolytic agent in the thrombosed branch of MCA.
View Figure 6
Figure 6: Injection of a fibrinolytic agent in the thrombosed branch of MCA.
View Figure 6
Iatrogenic stenosis of the cerebral artery developed after clipping can be managed with early reoperation and clip reposition. Intracranial intra-arterial injection of a fibrinolytic agent can restore blood flow in a thrombosed vessel and prevent irreversible neurological deficit associated with a cerebral ischemia.
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests.