Melanoma is the 5th most common cancer in males and 7th in females with an annual incidence of 32,100 patients in the US. CNS spread of melanoma represents approximately 10% of all brain metastases [1-3]. The vast majority of CNS involvement is either in the form of intraparenchymal metastasis, leptomeningeal or dural-based. Intraventricular involvement, on the other hand, is extremely rare [4]. We report two cases of intraventricular metastatic melanoma in this publication.
A 55-year-old male with a history of left thigh invasive melanoma resected a year ago with negative margins, presented to emergency department with a few days of severe headaches followed by urinary incontinence and decreased level of consciousness. Initial computerized axial tomography (CT) revealed a third ventricle/pineal region mass with effacement of the cerebral aqueduct with acute obstructive hydrocephalus. At the time of neurosurgical assessment, the patient was localizing and opening his eyes to noxious stimuli and making incomprehensive sounds. Given the poor neurological exam and the scan findings, an urgent right frontal external ventricular drain was inserted to decompress the patient's ventricles. Following stabilization, brain MRI with gadolinium was obtained which demonstrated a heterogeneously enhancing third ventricular/pineal region mass with obstruction of the aqueduct (Figure 1). Right frontal endoscopic third ventriculostomy with septostomy and biopsy of the mass was performed with image guidance. The tumor was extremely vascular, and the patient developed significant intraventricular hemorrhage which was managed with an external ventricular drain (EVD). A week later the EVD was removed and the patient was discharged neurologically intact.
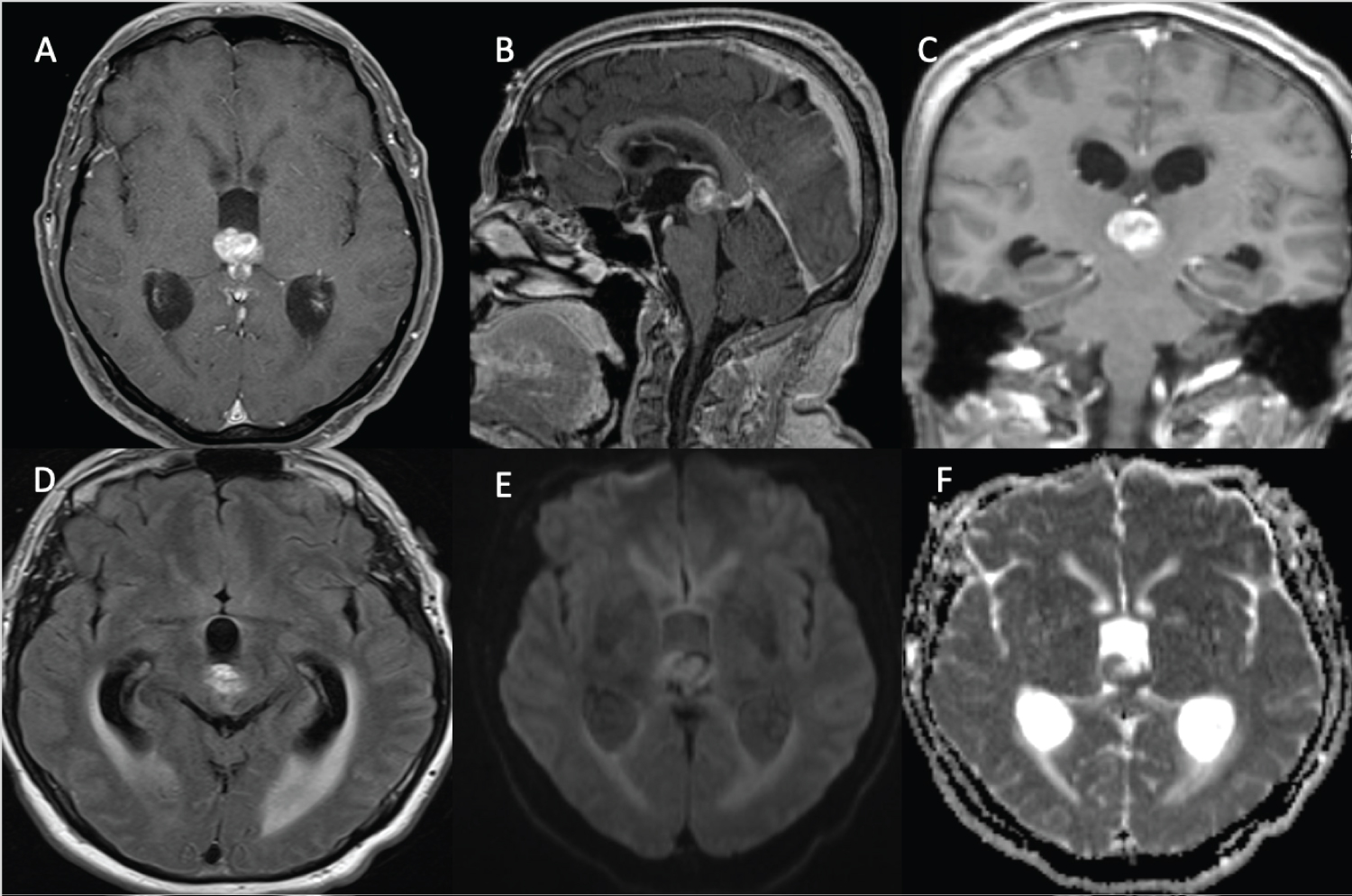 Figure 1: Intraventricular/Pineal melanoma metastasis. (A, B & C) axial, sagittal and coronal T1 with GAD shows heterogeneously enhancing third ventricular/pineal region mass. (D) Axial FLAIR demonstrates mild ventriculomegaly with ballooning of third ventricles and trans ependymal flow secondary to the mass. (E & F) Axial diffusion-weighted imaging (DWI & ADC) demonstrates peripheral diffusion restriction. Findings are compatible with intraventricular/pineal region metastatic melanoma.
View Figure 1
Figure 1: Intraventricular/Pineal melanoma metastasis. (A, B & C) axial, sagittal and coronal T1 with GAD shows heterogeneously enhancing third ventricular/pineal region mass. (D) Axial FLAIR demonstrates mild ventriculomegaly with ballooning of third ventricles and trans ependymal flow secondary to the mass. (E & F) Axial diffusion-weighted imaging (DWI & ADC) demonstrates peripheral diffusion restriction. Findings are compatible with intraventricular/pineal region metastatic melanoma.
View Figure 1
Pathological examination of the biopsied tissue showed a malignant epithelioid tumor with sheet-like growth and mitosis (Figure 2). Immunohistochemistry revealed focally positive S100, Melanoma Cocktail, MelanA and HMB45, minimal staining of synaptophysin and glial fibrillary acidic protein, negative EMA and AE1/AE3, and a high Ki67 proliferation index of 30-40%. These pathological features are consistent with metastatic melanoma in addition to the patient known history of invasive melanoma. Further molecular studies revealed that the lesion is BRAF wild type.
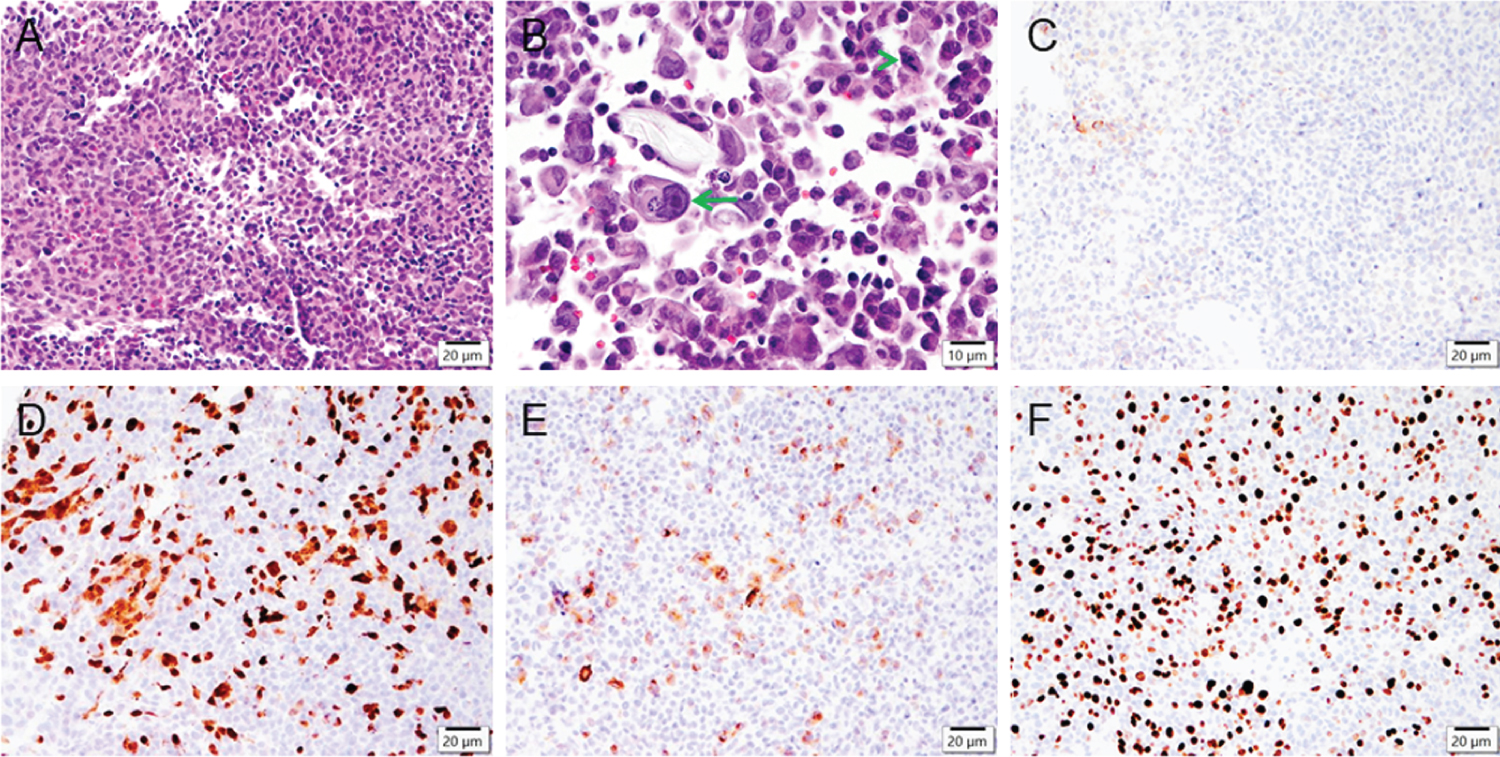 Figure 2: Intraventricular/pineal region tumor pathology. Microphotographs of the biopsied tissue shows a patternless tumor (A) composed of epithelioid cells with large irregular nuclei containing prominent nucleoli (B, arrow) and mitosis (B, arrowhead). Immunohistochemistry reveals minimal staining of synaptophysin (C), focally positive S100 (D) and Melanoma cocktail (E), and a markedly high Ki67 proliferation index (F). Scale bars: 20 μm (A, C-F), 10 μm (B).
View Figure 2
Figure 2: Intraventricular/pineal region tumor pathology. Microphotographs of the biopsied tissue shows a patternless tumor (A) composed of epithelioid cells with large irregular nuclei containing prominent nucleoli (B, arrow) and mitosis (B, arrowhead). Immunohistochemistry reveals minimal staining of synaptophysin (C), focally positive S100 (D) and Melanoma cocktail (E), and a markedly high Ki67 proliferation index (F). Scale bars: 20 μm (A, C-F), 10 μm (B).
View Figure 2
At two months follow-up, the patient remains neurologically intact, had received 5 fractions of stereotactic radiosurgery and waiting for 2 cycles of immunotherapy.
A 69-year-old female with a history of malignant scalp melanoma resected previously presented with nausea and vomiting which was found to be caused by a large right lateral ventricular mass. The headache was constant and severe for five days prior to presentation and further laboratory workup revealed hyponatremia attributed to SIADH. Brain MRI with contrast revealed a large lateral intraventricular heterogeneously enhancing mass with mild supratentorial ventriculomegaly (Figure 3). Neurosurgical consultation was prompted.
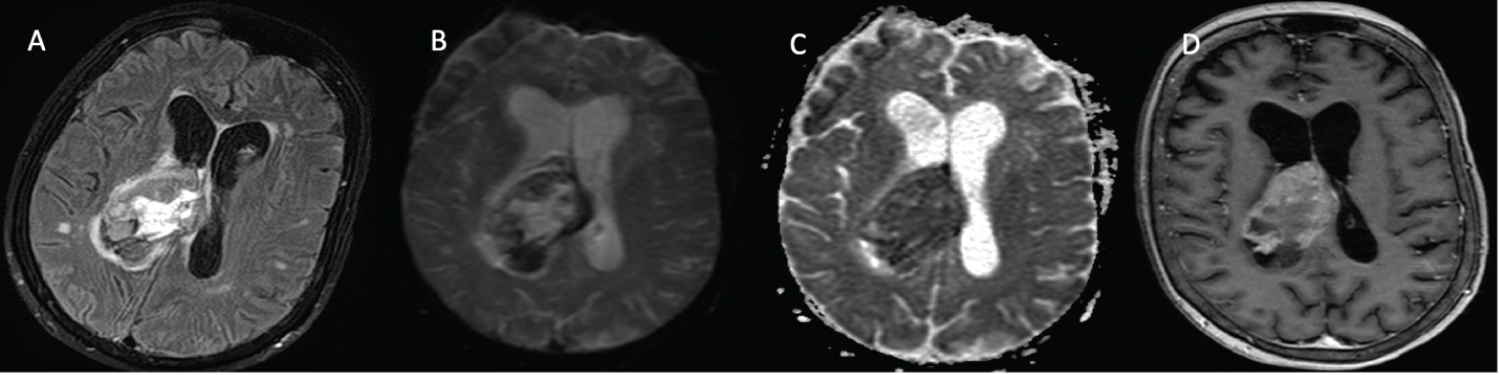 Figure 3: Intraventricular melanoma metastasis. (A) Axial FLAIR demonstrates mild ventriculomegaly with obliteration of the right lateral ventricle by a heterogeneous and hyperintense mass. In addition, there is a significant periventricular FLAIR hyperintensity signal consistent with trans ependymal flow; (B & C) Axial diffusion-weighted imaging (DWI & ADC) demonstrates a ventricular mass with marked diffusion restriction. (D) Axial T1 post contrast sequence shows avidly enhancing mass that is compatible with intraventricular metastatic melanoma.
View Figure 3
Figure 3: Intraventricular melanoma metastasis. (A) Axial FLAIR demonstrates mild ventriculomegaly with obliteration of the right lateral ventricle by a heterogeneous and hyperintense mass. In addition, there is a significant periventricular FLAIR hyperintensity signal consistent with trans ependymal flow; (B & C) Axial diffusion-weighted imaging (DWI & ADC) demonstrates a ventricular mass with marked diffusion restriction. (D) Axial T1 post contrast sequence shows avidly enhancing mass that is compatible with intraventricular metastatic melanoma.
View Figure 3
This patient had malignant melanoma of the scalp excised with negative margins ten years prior to this presentation. In spite of systemic immunotherapy, biopsy-proven lung metastasis developed subsequently, requiring more systemic therapy with eventual disease control until this presentation.
Neurologic assessment demonstrated a lethargic patient utilizing a wheelchair to ambulate yet without any significant focal deficit. The consensus between neurosurgery and oncology was favoring surgical resection followed by adjuvant therapy, given her overall clinical status and disease control. Therefore, a right parietal transcortical craniotomy with the use of Metrx tubular retractor system (Medtronic) and the overpass technique with image guidance was performed [5]. Given the extremely vascular nature of the lesion, gross total resection and hemostasis were difficult to achieve. Intraoperative EVD was placed, and the patient was transferred to the intensive care unit (ICU) intubated for further monitoring and stabilization. Postoperative imaging showed significant intraventricular hemorrhage necessitating the insertion of a contralateral EVD.
Microscopic examination (Figure 4) demonstrated that the tumor is composed of sheets of epithelioid-type cells with prominent nuclei and nucleoli (predominantly amelanotic). There are multiple areas of tumor necrosis, overall estimated at approximately 50%. Mitotic activity is brisk in areas. Immunohistochemistry shows patchy positivity of tumor cells for HMB45, while diffuse positivity is present for melanoma cocktail. Furthermore, the sample was positive for BRAF codon p.V600 mutation.
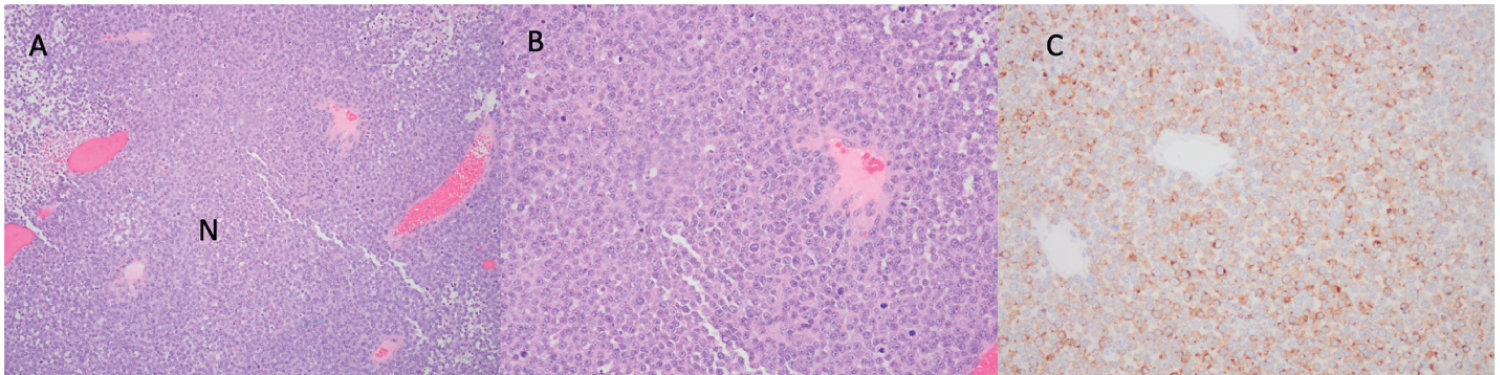 Figure 4: Intraventricular tumor pathology. (A) 100x H&E staining demonstrating largely amelanoticfocal necrosis; (B) 200x H&E staining showing frequent mitoses; (C) 200x Immunohistochemistry is positive for melanoma cocktail.
View Figure 4
Figure 4: Intraventricular tumor pathology. (A) 100x H&E staining demonstrating largely amelanoticfocal necrosis; (B) 200x H&E staining showing frequent mitoses; (C) 200x Immunohistochemistry is positive for melanoma cocktail.
View Figure 4
Postoperatively, the patient remained difficult to rouse in spite of the reversal of all other possible reversible causes for decreased level of consciousness. Given the patient's previously stated goals of care and her poor neurological status, the family elected to proceed with palliation with the patient passing away ten days postoperatively.
Intraventricular melanoma metastasis is rare and up to date, there are fifteen reported cases in the literature [6]. The primary site of origin tends to be the skin and in extreme circumstances primary CNS melanocytes. In up to 14% of cases of metastatic melanoma, in general, the primary site can be difficult to localize due to intraocular or GI mucosa origin [7]. The most common presenting symptoms are headache, nausea and vomiting which can be signs of early hydrocephalus [6]. The typical imaging characteristics are hyperdense avidly enhancing masses on head CT scans as well as T1 enhancement on brain MRIs [8]. Typically, intraventricular melanomas tend to favour the lateral ventricles, however, rarely, the third ventricle occurrence has been reported as in our first case [6]. Overall management relies on the patient Karnofsky performance scale (KPS) score, the lesion location and accessibility, followed by systemic adjuvant therapy. As illustrated earlier, transcortical approaches aiming for gross total resection can be feasible for accessible lesions whereas endoscopic biopsy is reasonable in deep-seated masses [9]. Furthermore, BRAF inhibitors can be useful in tumors with BRAF oncogene mutation, however, this is still under investigation [10]. Despite the current advancement, patient survival is poor in all reported cases [6].
Intraventricular melanoma spread is rare and poorly understood due to the rarity of the condition. The principles of neuro-oncological management still apply in terms of surgical resections followed by adjuvant therapy when feasible for suitable candidates. The overall prognosis however appears to be poor thus far.