Frontosphenoidal craniosynostosis is an extremely rare and often misdiagnosed cause of anterior plagiocephaly. Careful clinical examination and radiological features allow to differentiate between this entity and other forms of frontal asymmetry. This study aims to describe the impact of premature fusion of the frontosphenoidal suture in the development of orbital and cranial morphology, to compare it with the effect caused by coronal synostosis and to detail the surgical procedure used to correct both.
We report three patients diagnosed with anterior plagiocephaly caused by frontosphenoidal synostosis and compare it with the clinical features and surgical implications of a patient affected by unilateral coronal craniosynostosis.
Isolated frontosphenoidal synostosis must be taken into account in the differential diagnoses of frontal plagiocephalies. Key clinical features such as the displacement of the supraorbital edge, morphology of the temporal region on the affected side and deviation of the nasal root and chin can help to differentiate it from coronal craniosynosotosis and, consequently, to select proper surgical techniques.
Craniosynostosis, Anterior plagiocephaly, Frontosphenoidal craniosynostosis, Synostotic plagiocephaly
CT Scan: Computed Tomography
Forehead and orbital deformities represent a common finding in simple suture craniosynostosis. Plagiocephaly is described as a unilateral flattening of the forehead and orbital dystopia, the most common underlying cause being usually an unilateral coronal suture synostosis. Differential diagnoses done mainly with anterior deformational asymmetries [1]. However, frontal craniosynostosis could be related to isolated involvement of other components of the coronal ring such as frontosphenoidal suture [2]. In 1995, Francel and collegues reported the first case of isolated frontosphenoidal craniosynostosis [3] and so far, only isolated case reports [2,4-18] and small retrospective studies have been published in the literature [19,20]. Both forms of monosutural craniosynostosis - coronal and frontosphenoidal - may lead to a similar but subtly distinct phenotype and radiological presentation. Therefore, it is capital to differentiate these entities to select the most appropriate surgical correction. We report three patients with a diagnosis of frontosphenoidal craniosynostosis and compare them with the more frequent: coronal craniosynostosis. The aim of this paper is to describe and identify the differences between the two craniofacial deformities and to detail the surgical procedures to correct them.
A 8-months-old first born boy was referred to our Department due to frontal asymmetry. Antenatal history was unremarkable and delivery was uncomplicated. A progressive flattening of the left forehead was observed by his parents at the age of 5-6 months. After consultation with his primary care pediatrician, a suspected diagnosed of anterior plagiocephaly was done and then, referred to a Neurosurgery specialist. Under physical examination, the patients showed retrusion and downward displacement of the orbital rim, moderate flattening of the forehead, a deviation of the nasal root towards to the non-synostotic side and ipsilateral hollowing of temporal squama. CT imaging was performed demonstrating as shown in Figure 1 a widely patent frontoparietal suture and a clearly synostotic frontosphenoidal suture. Postoperative medium-term CT follow-up and clinical evaluation showed progressive improvement and subsequent stability of orbital displacement and frontal projection as shown in the Figure 2.
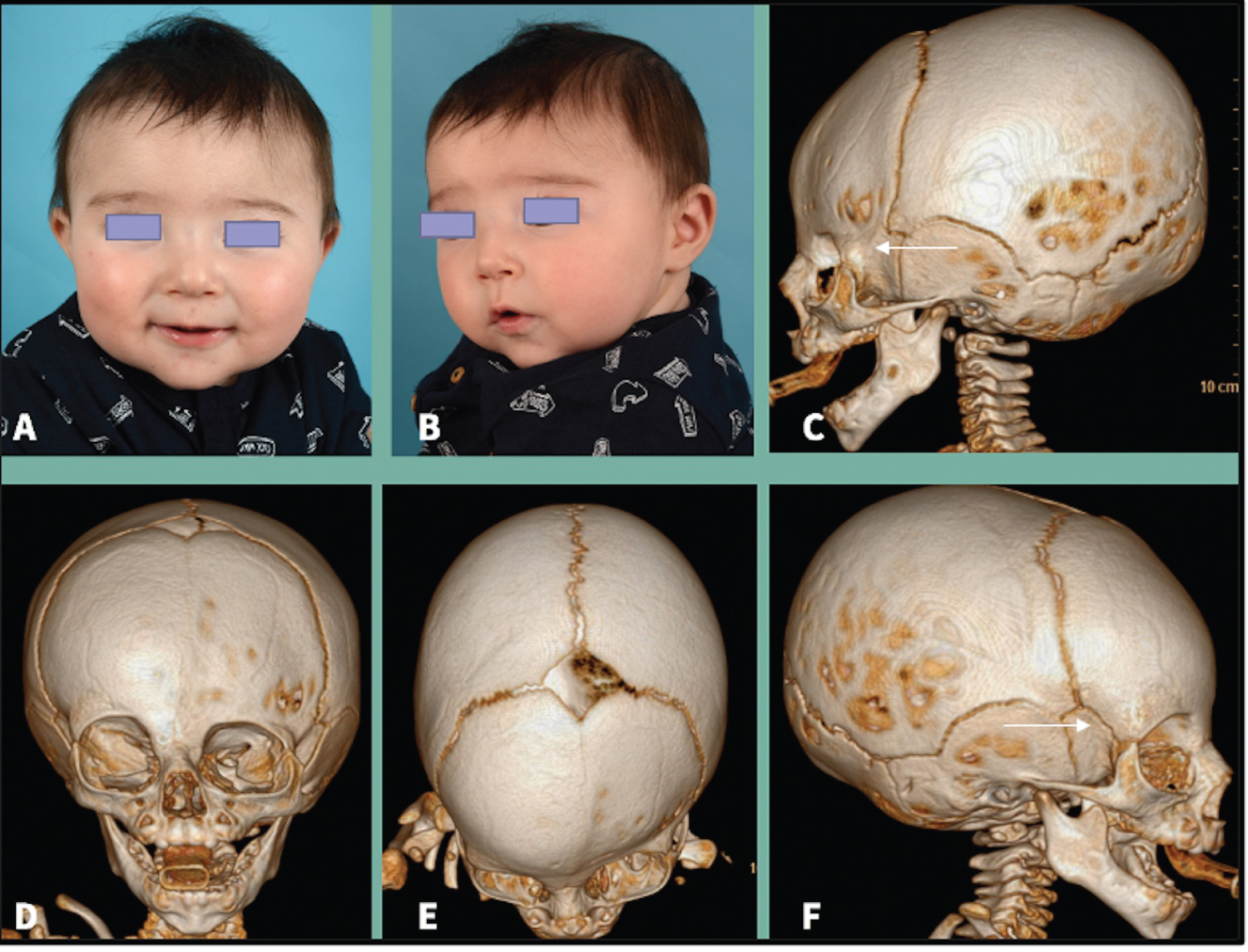 Figure 1: A, B) Preoperative pictures and CT scan with three-dimensional reconstruction show frontal (D), vertex (E) and lateral views (C, F) of a child with frontosphenoidal craniosynostosis. C. The arrow shows a synostotic frontosphenoidal suture. F. On the opposite side, the arrow marks a patent frontosphenoidal suture.
View Figure 1
Figure 1: A, B) Preoperative pictures and CT scan with three-dimensional reconstruction show frontal (D), vertex (E) and lateral views (C, F) of a child with frontosphenoidal craniosynostosis. C. The arrow shows a synostotic frontosphenoidal suture. F. On the opposite side, the arrow marks a patent frontosphenoidal suture.
View Figure 1
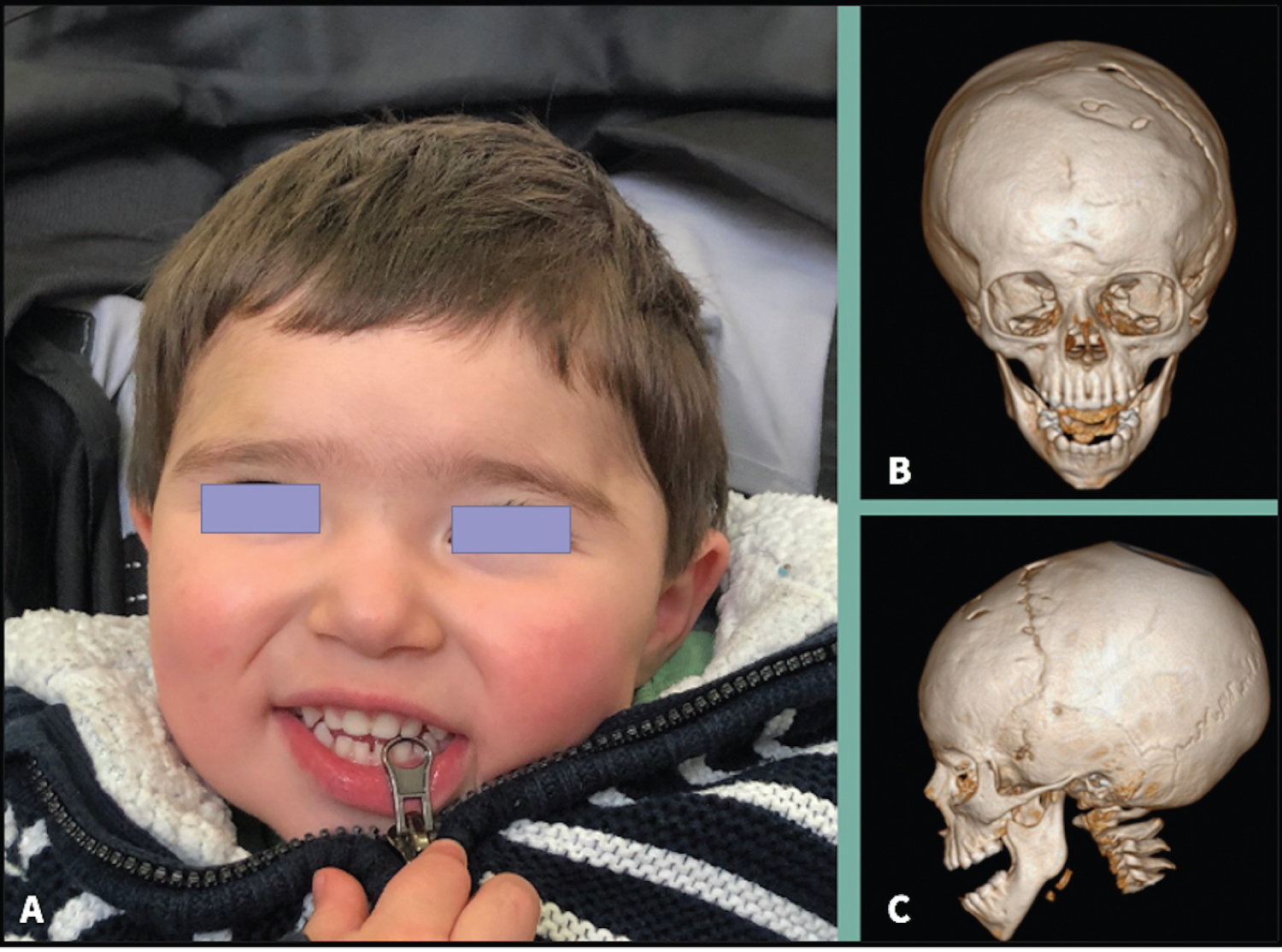 Figure 2: Posoperative picture. A) CT scan; B,C) At one and a half years follow-up showing correction of downward orbital rim and frontal flattening.
View Figure 2
Figure 2: Posoperative picture. A) CT scan; B,C) At one and a half years follow-up showing correction of downward orbital rim and frontal flattening.
View Figure 2
A 7-5 months-old male patient came to our consultation referred for anterior plagiocephaly with a suspected diagnosis of coronal synostosis. The patient was the first-born from a non- consanguineuos young couple. Antenatal and obstetrical history was otherwise irrelevant. He presented to our examination with a left frontal flattening with a ipsilateral downward eyebrow and supraorbital rim. Nasal tip was desviated to the left side and the chin centered on the midline. Ophtalmological examination excluded strabismus or amblyopia. CT scan revealed a left frontosphenoidal suture fusion and a patency of the right frontosphenoidal suture as shown in the Figure 3.
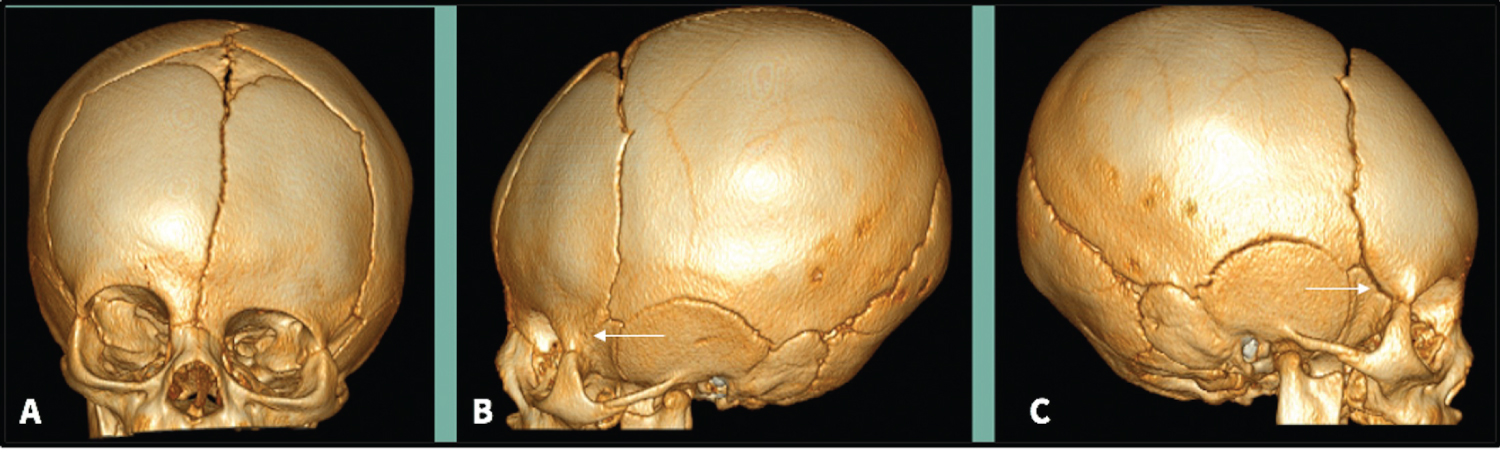 Figure 3: A) Three-dimensional CT reconstruction shows frontal; B,C) Lateral views. The arrow in image B represents left frontosphenoidal fusion and in C a right frontosphenoidal suture patency.
View Figure 3
Figure 3: A) Three-dimensional CT reconstruction shows frontal; B,C) Lateral views. The arrow in image B represents left frontosphenoidal fusion and in C a right frontosphenoidal suture patency.
View Figure 3
A five-months-old male patient was sent by his pediatrician to evaluate anterior facial asymmetry. On clinical examination, he had a left frontal flattening, a nasal tips lightly offset toward flattening, but no harlequin's eye. No ophthalmological problems were reported. CT scan showed closure of the left frontosphenoidal suture with a descent and retrusion of the ipsilateral orbit, while the right frontosphenoidal suture and both coronal sutures were patent as shown in the Figure 4.
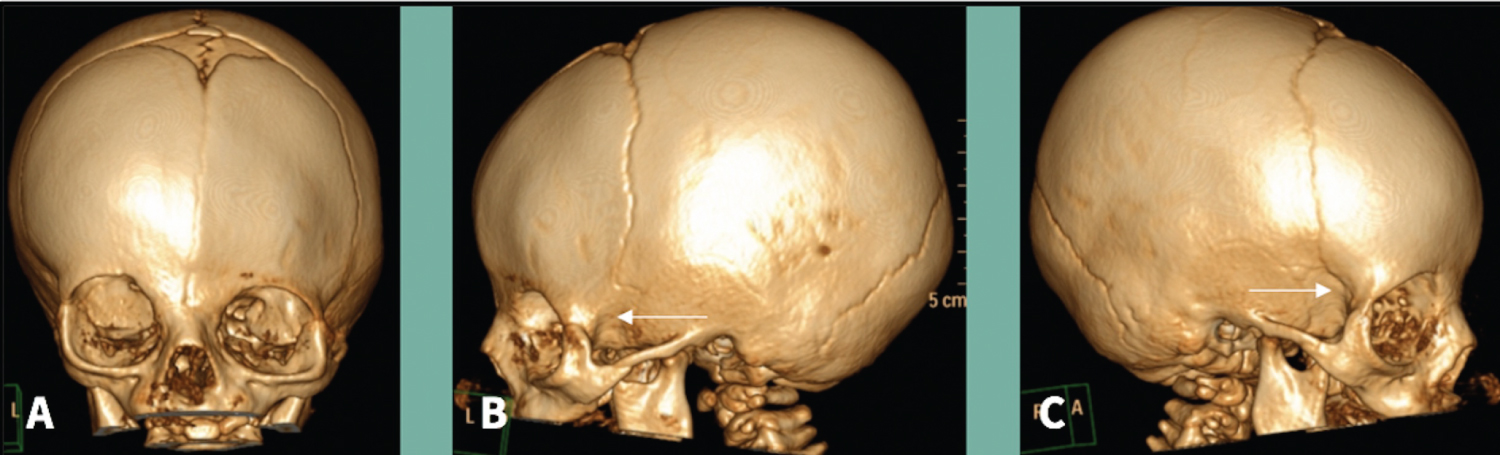 Figure 4: A,B) The images show descent and retrusion of the orbit; B) The arrow indicates closure of the suture on the left side; C) The arrow points the suture is patent.
View Figure 4
Figure 4: A,B) The images show descent and retrusion of the orbit; B) The arrow indicates closure of the suture on the left side; C) The arrow points the suture is patent.
View Figure 4
Genetic studies were not carried out in any of the three patients as they were all considered isolated craniosynostosis.
In our three patients, a left-sided advancement of a fronto-orbital bandeau was performed with frontal reshaping in "shell" variant [21] or with a Tessier bone bender as shown in Figure 5 and Figure 6. In frontosphenoidal craniosynostosis the orbital rim is displaced downward and backward compared to healthy side. So, the aim of surgical correction consists of advancement of the orbital edge and achievement of a elevation of the lateral canthus of the affected side together with a symmetric frontal bone flap on the synostotic side to create a normal-looking forehead. Bandeau reshaping and advancement in conjunction with the frontal bone were tailored to the magnitude of the craniofacial deformity in each individual patient, and unaffected side was used as a template for accurate surgical correction. The different bony segments were fixed with resorbable plates and screws. The surgery was well tolerated in all cases and the patients had an uneventful postoperative course.
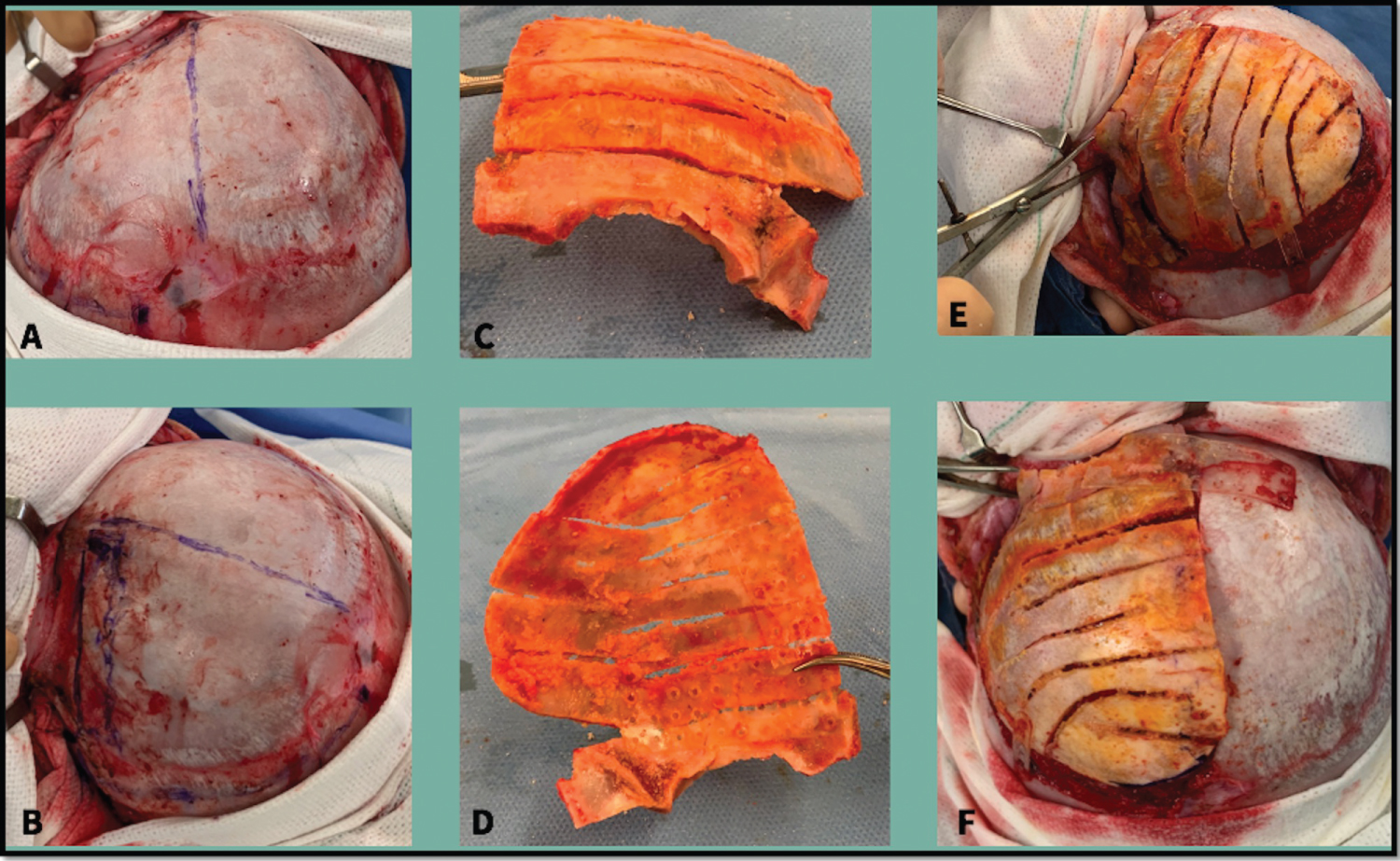 Figure 5: Surgical technique. D) Detail of the osteosynthesis on the inner side of the bone flap; E) The compass shows the orbital advancement performed; F) The compass indicates the ascent of the orbit obtained.
View Figure 5
Figure 5: Surgical technique. D) Detail of the osteosynthesis on the inner side of the bone flap; E) The compass shows the orbital advancement performed; F) The compass indicates the ascent of the orbit obtained.
View Figure 5
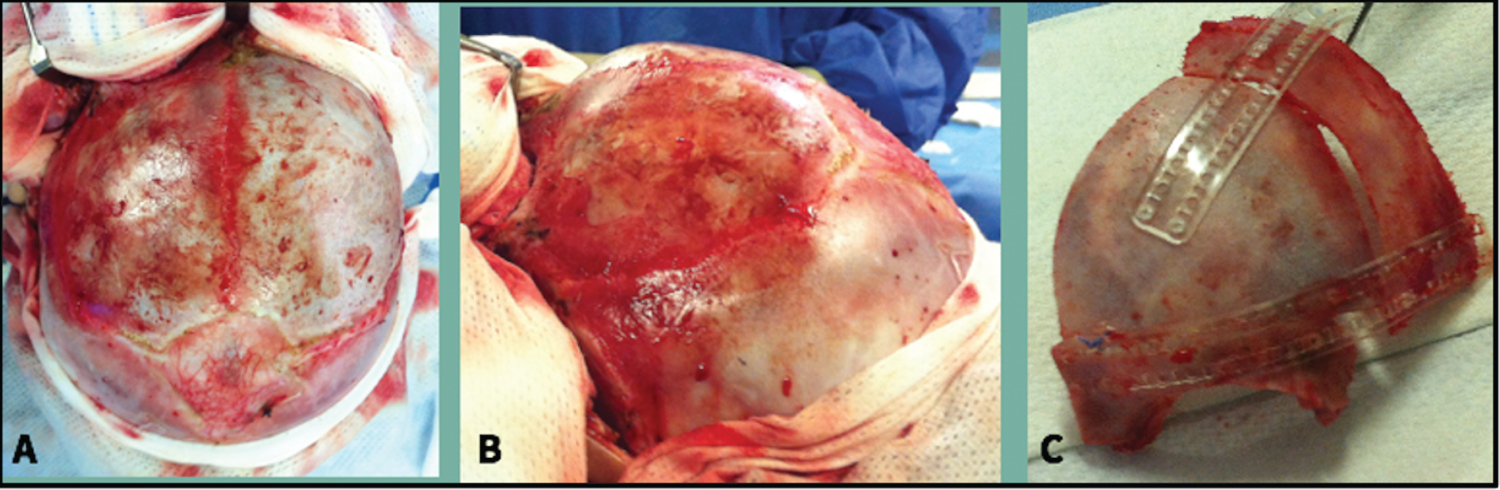 Figure 6: A,B) Show the retrusion and downward displacement of the orbital rim associated with synostosis; C) Remodeling obtained after frontal advancement and elevation of the supraorbital rim.
View Figure 6
Figure 6: A,B) Show the retrusion and downward displacement of the orbital rim associated with synostosis; C) Remodeling obtained after frontal advancement and elevation of the supraorbital rim.
View Figure 6
Frontoorbital craniosynostosis is a rare form of anterior craniosynostosis. Mostly, case series are reported in literature [2-18] with the exception of two retrospective series comprising 12 and 17 years that reported only 12 patients [19,20]. This report adds another three patients to the clinical series and faces the unique challenges regarding appropriate diagnosis and surgical treatment of these patients.
The phenotype of frontosphenoidal craniosynostosis is milder compared to unilateral coronal synostosis. This difference is explained by the time and the area where the synosotosis occurs. Synostosis of the coronal suture usually as often happens around 16 weeks of embryological development. This fusión promotes the absence of the coronal suture and therefore, permits only the peripheral growth of the frontal and parietal bone. Fixation of the frontal bone to the parietal bone restricts the growth of the orbit in an antero caudal direction, leading to cranial displacement of the supraorbital rim. Conversely, the milder presentation of frontosphenoidal craniosynostosis is due to the fact that the fusion of this suture takes place several weeks later, around the 21st week of embiological development. The premature fusión restricts the growth of the fronto-orbital border and orbital roof in an an anterocaudal direction. Thus, the resulting cranial deformity is characterized by a downward displaced orbital edge and a descent of the pterion and orbital roof [6].
Surgical correction of craniofacial deformity is indicated due to the ophthalmological implications of ocular malposition (astigmatism, amblyopia, strabismus) [22,23] and not so much because of the risk of developing intracranial hypertension, sleep apnea or optic atrophy which are typically associated with synostosis of other cranial vault sutures [23]. A skull-molding helmet has been reported for the treatment of this condition. However, this therapy ultimately failed and required surgical treatment [6,11,18].
In our three cases, the surgical technique consisted of unilateral fronto-orbital advancement and frontal remodeling to achieve symmetry with the non-synostotic side. Before starting bone osteotomies, the cranial vault was carefully examined looking for a new forehead and orbit with adequate and harmonic shape. The osteotomies performed during harvesting of fronto-orbital bandeau incorporated the fused frontosphenoidal suture, but the classic tongue-in-groove procedure was not necessary because resorbable fixation material provides adequate stability as other groups have reported [1]. This technical variation helps to reposition the supraorbital bandeau when a rotation in coronal plane is required to confer an elevation to lateral canthus of the orbit. Otherwise, we observed a pathological pterion with a rough appearance and vertical displacement, which leads to deeper osteotomies just like Lloid and coworkers has described [16]. The orbital rim is smoothed and shaped as necessary prior to repositioning. Pterion is removed to promote ventral expansion of brain in the anterior cranial fossa. The abnormal frontal bone flap is reshaped with a Tessier bone bender as needed. Relief cuts are made when necessary to facilitate the frontal remodeling and placed over the dura at the donor site. Ipsilateral flattening of temporal squamais corrected by autologous bone graft and fixed to frontal bone.
Given the phenotypic differences between frontosphenoidal craniosynostosis and coronal synostosis, we tailor our surgical approach to correct the specific deformities of each entity [5,12]. This is opposite to prior studies that suggested the same techniques for both craniosynostosis [14,24]. In Figure 7, we show the typical harlequin deformity described in coronal synostosis, with horizontal narrowing and elevation in the coronal plane of the affected orbit as compared to the non-affected side. In this manner the pathological orbit can be corrected advancing and descending the superolateral-edge.
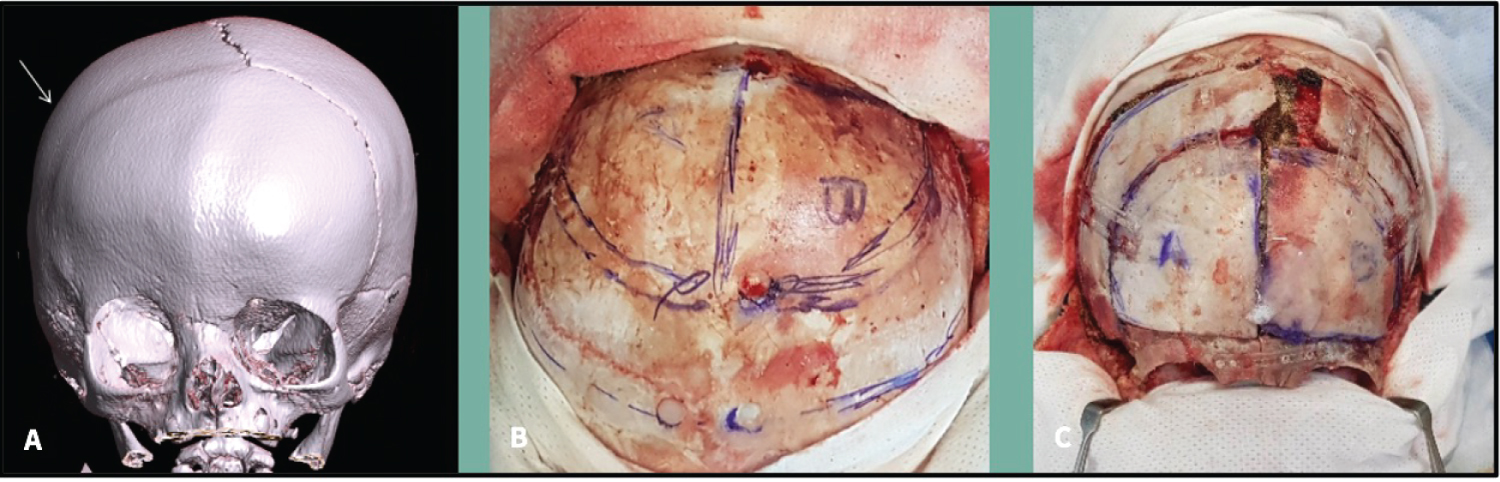 Figure 7: A) Three-dimensional CT reconstruction shows a coronal craniosynostosis with ipsilateral retrusion of the forehead and elevation of the superior orbital rim; B) Intraoperative picture represents the outline of the craniotomies; C) Repositioning and fixation of the reshaped bifrontal bone and correction of the supraorbital rim.
View Figure 7
Figure 7: A) Three-dimensional CT reconstruction shows a coronal craniosynostosis with ipsilateral retrusion of the forehead and elevation of the superior orbital rim; B) Intraoperative picture represents the outline of the craniotomies; C) Repositioning and fixation of the reshaped bifrontal bone and correction of the supraorbital rim.
View Figure 7
Regarding the surgical approach, we describe a unilateral correction of synostotic side in contrast to what most authors have reported so far [5,6,11,13-15,17,20]. Plooji and Mittermiller presented a patient, who underwent a unilateral procedure with good cosmestic outcomes [8,18]. Based in our results, we believe that this variation in the technique provides a satisfactory and stable correction of preoperative deformities as long as there is no contralateral compensatory craniofacial malformation.
Unilateral frontosphenoidal craniosynostosis is an infrequent cause of anterior plagiocephaly. Differential diagnosis with coronal synostotsis may be difficult and could result in delayed and improper treatment. Unilateral fronto-orbital advancement constitutes an option for surgical correction in frontosphenoidal craniosynostosis in the absence of compensatory deformity on the non-synostotic side.
Acknowledgement are not applicable.
This submission complies with the guidelines for human studies and was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. Ethical approval was not required for this study in accordance with national guidelines as there was no changes in the surgical tecnhiques as compared with previous cases and none of the patients could be traced after imaging procesing.
Written informed consent for publication of this case report and accompanying images was obtained from parents, as patients are minor, following the specific written protocol from our own institution.
Images were processed to completely anonymize patients, and they do not allow recognition.
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
No funding has been received for this case report. All authors confirm that they have no affiliations with or involvement in any organization or entity with any financial or nonfinancial interest in the issue or materials discussed in this manuscript.
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the Corresponding author.
Dra. Victoria Becerra and Dr. José Hinojosa contributed equally to the design, writting and revision of this manuscript, imaging procesing, as well as to the surgery of these patients.
Dr. Santiago Candela, Dr. Diego Culebras and Dra. Mariana Alamar critically reviewed the images and manuscript of this submission.